
Abstract
Introduction
Subcutaneous emphysema of the scrotum due to traumatic pneumothorax is a rare medical situation and only a few cases are reported in the literature.
Case report
We present the case of a 22 year old man who was admitted to the emergency department after a motorcycle accident having a painless crepitant scrotum and chest excoriations. Further evaluation revealed subcutaneous emphysema of the scrotum caused by left pneumothorax.
Conclusion
In conclusion, subcutaneous emphysema of the scrotum (or pneumoscrotum) due to traumatic pneumothorax is not an urgent condition and assessment should be supportive with intervention directed at the etiology, e.g. the pneumothorax.
Similar content being viewed by others


Background
Subcutaneous emphysema of the scrotum (or pneumoscrotum) is a rare condition and receives little or no discussion in standard texts of urology. This paper presents a case of pneumoscrotum due to traumatic pneumothorax and discusses its clinical course, findings and treatment strategy with a review of the relevant literature.
Case presentation
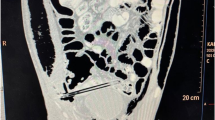
A 22 year old man was admitted to the emergency department following a motorcycle accident. He had chest excoriations and a painless crepitant scrotum (Fig 1, 2.). Palpation of the scrotum was characteristic and gave the impression of palpating "snow". Testicles could not be palpated. During clinical examination, patient complained of incipient dyspnea. Auscultation of the lungs placed the suspicion of pneumothorax. The CT imaging study demonstrated a left pneumothorax (Fig. 3) causing a subcutaneous emphysema that was expanded in the scrotum (Fig. 4). A left haemothorax and three rib fractures were also diagnosed. No lesions of the genitalia were diagnosed. A chest drainage tube was inserted and further assessment was supportive in collaboration with the thoracosurgery clinic. Patient was dismissed eight days after the accident. Pneumothorax was partially absorbed and further control was arranged as an outpatient. By one month, no air was found in the ultrasound imaging of the scrotum.

Oedematous scrotum (profile).

Oedematous scrotum.

CT demonstrates left pneumo-haemothorax with subcutaneous emphysema.

CT demonstrates pneumoscrotum (red arrows).
Discussion
Subcutaneous emphysema of the scrotum – especially of traumatic etiology – is not a common medical condition. Causes that may result in the presence of air in the scrotum are:
-
1.
Iatrogenic: such as various endoscopies (colonoscopy, polypectomy, laparoscopic procedures, tracheostomy, CPR, chest drain tube insertion, dental procedures) [1–3].
-
2.
Gas producing infection (gangrene Fournier).
- 3.
-
4.
Scrotal trauma.
-
5.
Visceral perforation [6].
The true nature of the development of the subcutaneous emphysema of the scrotum has not been fully elucidated. Three possible mechanisms were proposed:
-
1.
Rapture of the alveoli and expansion of the air through the mediastinum in the subcutaneous area [6].
-
2.
Expansion of the emphysema along the Scarpa's Fascia [7].
-
3.
Through the mediastinum air passes in the paranephric space and through the retroperitoneum and the inguinal canal is gathered in the scrotum [8–10].
In the case described above, spread of the subcutaneous emphysema towards scrotum is the most "desirable" potential, given the fact that if this expansion was towards neck it could obstruct the upper airways and lead to suffocation.
Conclusion
We can support that subcutaneous emphysema of the scrotum due to traumatic pneumothorax (blunt trauma), despite its impressive clinical presentation, is not really an urgent situation and assessment should be supportive with intervention directed at the etiology, that is the pneumothorax [11].
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in Chief of this journal.
Abbreviations
- CT:
-
Computed Tomography
- CPR:
-
Cardio Pulmonary Resuscitation.
References
Stavem K, Hoivik B: [Pneumoscrotum after air leak from tension pneumothorax]. Tidsskr Nor Laegeforen. 116 (10): 1214-5. 1996 Apr 20
Humpheys F, Hewetson KA, Dellipianni AW: Massive subcutaneous emphysema following colonoscopy. Endoscopy. 1984, 16 (4): 160-161. 10.1055/s-2007-1018566.
Casey RG, Al-Dousari S, Murphy D, Power RE: Chest drain insertion may result in the acute scrotum. Scand J Urol N ephrol. 2006, 40 (1): 78-9. 10.1080/00365590500522718.
Wakabayashi Y, Bush WH: Pneumoscrotum after blunt chest trauma. J Emerg Med. 1994, 12 (5): 603-5. 10.1016/0736-4679(94)90410-3.
Firman R, Heiselman D, Lloyd T, Mardesich P: Pneumoscrotum. Ann Emerg Med. 1993, 22 (8): 1353-6. 10.1016/S0196-0644(05)80122-2.
Aslan Y, Sarihan H, Dinc H, Gedik Y, Aksoy A, Dereci S: Gastric perforation presenting as bilateral scrotal pneumatoceles. Turk J pediatr. 1999, 41 (2): 267-71.
Millmond SH, Goldman SM: Pneumoscrotum after spontaneous pneumothorax with air leak. J Urol. 1991, 145 (6): 1271-1272.
Heimbach D, Hofmockel G, Wirth M, Frohmuller H: Pneumoscrotum: Case report and review of the literature. Urologe A. 1993, 32 (6): 503-506.
Casey RG, Al-Dousari S, Murphy D, Power RE: Chest drain insertion may result in the acute scrotum. Scand J Urol Nephrol. 2006, 40 (1): 78-79. 10.1080/00365590500522718.
Watson HS, Klugo RC, Coffield KS: Pneumoscrotum: report of two cases and rewiew of the mechanisms or its development. Urology. 1992, 40 (6): 517-521. 10.1016/0090-4295(92)90406-M.
Mateos Colino A, Golpe Gomez R, Gonzalez Rodriguez A, Sousa Escandon A, Gonzalez Uribarri C, Seirulo Salas M: Neumoescroto secundario a efisema sudcutaneo masivo tras el drenale de un neumotorax espontaneo. Actas Urol Esp. 2004, 606-609.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All authors have made substantial contribution to concept this case reports
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Simaioforidis, V., Kontos, S., Fokitis, I. et al. Subcutaneous emphysema of the scrotum (pneumoscrotum) due to traumatic pneumothorax: a case report. Cases Journal 1, 293 (2008). https://doi.org/10.1186/1757-1626-1-293
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1757-1626-1-293