
Abstract
Background
Previous studies on orthodontic treatment need in young adults have shown that up to 50% had malocclusions that needed orthodontic treatment. The aims of this study were to assess the normative and self-perceived need for orthodontic treatment using the Index of Orthodontic Treatment Need (IOTN) and to determine if the treatment need levels were influenced by sex, age and socio-economic status (SES) in a sample of Peruvian young adults.
Methods
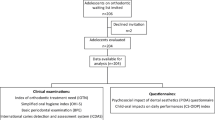
281 first-year students (157 male and 124 female students) with a mean age of 18.1 +/- 1.6 years were randomly selected and evaluated through the Dental Health Component (DHC) and Aesthetic Component (AC) of the IOTN. Structured interview and clinical examination were used to assess the students. Descriptive statistics and Chi-square tests were used for data analysis with statistical significance set at P < 0.05.
Results
An intra-examiner reliability of 0.89 was obtained (weighted Kappa). The percentage of students according to SES was 51.2%, 40.6% and 8.2% corresponding to low, medium and high SES respectively. The percentage of students with DHC grades 4–5 was 29.9% whereas the percentage of students with AC grades 8–10 was 1.8%. There were no significant differences in the distribution of normative and self-perceived orthodontic treatment need based on sex, age and SES comparisons.
Conclusion
Normative orthodontic treatment need was not matched by a similar level of self-perceived treatment need in these young adults. Sex, age and SES were non-significant factors associated with levels of treatment need.
Similar content being viewed by others


Background
The planning of orthodontic treatment within a public health system requires information on the orthodontic treatment needs of the population [1]. This would permit selection of cases to be treated based on financial, political or administrative purposes [2]. These indexes quantify and summarize a set of clinical and/or radiological data to obtain a final quantitative score or qualitative categorization [3–5]. In essence, the primary purpose of an orthodontic treatment need index is to identify individuals who would benefit from orthodontic treatment and would be given treatment priority [5].
The assessment of orthodontic treatment need, based on the Index of Orthodontic Treatment Need (IOTN) [6], has gained international acceptance in recent years because it was found to be valid, reliable and easy to use [3, 4, 7–11].
Briefly, the IOTN has two parts: the Aesthetic (AC) and the Dental Health (DHC) components. The AC assesses the perception of an individual on the attractiveness of his/her dentition through a 10-point photographical scale showing different levels of dental attractiveness, with photo 1 representing the most attractive and photo 10 the least attractive [6, 12]. Photos 1 to 4 represent 'no need for treatment'; 5 to 7 'borderline need for treatment' and 8 to 10 'definite need for orthodontic treatment'. The DHC assesses 10 traits of malocclusion: overjet, reverse overjet, overbite, openbite, crossbite, crowding, impeded eruption, defects of cleft lip and palate as well as any craniofacial anomaly, Class II and Class II buccal occlusions, and hypodontia. The DHC identifies the worst occlusal trait that is potentially detrimental to dental health and each given grade is a reflection of the level of orthodontic treatment need for the basis of treatment prioritization [3, 6, 7, 13]. Grades 1 and 2 represent 'no need for treatment'; grade 3 'moderate/borderline need for treatment' and grades 4 and 5 'definite need for orthodontic treatment.
Since consciousness of body image increases during childhood and adolescence, young adults are considered to be a relevant age group for the study of personal dental appearance perception [14]. The determination of prevailing orthodontic treatment need in young adults is important because individuals with high treatment needs can be identified and advised accordingly [15]. In addition, information regarding orthodontic treatment need of young adults would be relevant for evaluating satisfaction with dental appearance in orthodontically treated and untreated individuals and for assessing treatment outcomes [14, 16].
Although studies on young adults have reported that up to 50% of study samples had definite orthodontic treatment needs [15, 17–28], there is little information regarding treatment need levels in developing countries such as Peru. Nevertheless, malocclusion is undoubtedly a public health concern in any country.
The aims of this study were to assess the normative and self-perceived need for orthodontic treatment in a sample of Peruvian young adults using the IOTN and to compare the treatment need levels according to sex, age and socio-economic status (SES) of the students. This should serve as a starting point for an adaptation or the creation of a new index for orthodontic need for the Peruvian population. The use of indexes validated elsewhere have to be considered carefully since the definition of a population's need is not universal. This is especially true for aesthetic perception of need.
Methods
The study sample compromised of 281 first-year university students who were randomly selected from a population of 780 students in a private university from Lima (Peru). The registration list of the students admitted to the 2003 academic year was used as a sampling frame for the sample selection. Students with a past history or active orthodontic treatment were excluded from the study. The sample size was calculated for estimating an orthodontic treatment need of 24% in the population (using the DHC of the IOTN), at the 5% level (α = 0.05) and with a maximum tolerable error of 5%.
A structured face-to-face interview was carried out before the respective clinical examination of each student. First, students were asked to give their personal data as well as state their university tuition fee scale as an indirect measure of SES. In this university, students pay different tuition fees according to a socio-economic evaluation corroborated by a university social worker. An ordinal scale of three categories was available (low, medium and high SES). No additional information about desire and self-perceived need was requested from the students.
Thereafter, students rated their own perceived dental attractiveness on the AC of IOTN [6, 12], and whereas the normative orthodontic treatment need was assessed according to the DHC of the IOTN [6]. During clinical examination, hypodontia was determined as the absence of at least one tooth in any quadrant with restorative implications and impacted tooth was determined as the impeded eruption of any tooth (disregarding third molars) due to occlusal or pathological causes [6].
Clinical examinations were carried out at the University Dental Clinic by one examiner with experience in epidemiological evaluation of orthodontic treatment need [28–31]. To minimize random and systematic errors, intra-examiner reliability was assessed through duplicated assessments for ten students on different days (0.89, weighted Kappa).
Statistical analyses were conducted using the statistical package Intercooled Stata 8.0 for Windows (Stata Corporation, Texas, USA). Both components of IOTN were determined in percentages separately. Chi-square test was used to determine if there were significant differences in the distribution of DHC and AC grades according to sex, SES and age of students. Median age was used to separate the students into two age groups, where one group was < 18 years and the second group was ≥ 18 years of age. The level of significance was set at 0.05.
Results
The sample study (n = 281) consisted of 157 males (55.9%) and 124 females (44.1%). The mean age of the evaluated students was 18.1 +/- 1.6 years, with 79.3% ranging from 17 to 19 years old. The percentage distribution of students according to SES was 51.2%, 40.6% and 8.2% corresponding to low, medium and high SES respectively.
The objectively determined DHC distributions showed that 29.9% of the students were in great need of treatment (grades 4 and 5), 34.9% in moderate need of treatment (grade 3), and 35.2% with slight or no need for treatment (grades 2 and 1). Dental crowding, increased overjet and hypodontia were, in that order, the most common occlusal traits contributing to DHC grades (Table 1), with 57.2%, 12.4% and 6.4% of the evaluated students, respectively, having these traits.
Table 2 shows the comparison of DHC grades according to the evaluated covariables. When DHC grades were compared by sex, age and SES of the students no statistically significant differences were found (P = 0.403, 0.543 and 0.247 respectively).
The frequency distribution of AC of IOTN is exhibited in Figure 1. Only 1.8% of the students perceived themselves in definite need of treatment (photos 8–10), 11.0% in borderline need for treatment (photos 5–7) and 87.2% in no need for orthodontic treatment (photos 1–4). Photo number 2 was the most selected (30.6%).

Distribution of AC grades in the sample of evaluated students.
Due to the limited number of cases which were self-perceived as definitely needing orthodontic treatment, categories of borderline need and definite need were collapsed to develop a more appropriate statistical analysis. (Table 3) No statistically significant differences for AC grades according to gender, age and SES of the students were found (P = 0.750, 0.750 and 0.054 respectively).
Discussion
Several reasons have been previously reported to support the assessment of orthodontic treatment need in young adults [14–16]. In the present study, these young adults were selected for two additional reasons: first, their higher capability for expressing opinions on dental appearance in comparison to younger age groups [32, 33], and second, for their accessibility since young adults consistently attend university, where they could be evaluated simultaneously.
The study sample included students from a private university located in Lima, Peru. This university was selected by convenience, and the students recruited represented a highly selective group of young adults. As such, the results from this study would not be truly representative of the young adult population of Lima. Policy makers and public health dentists should interpret these results with caution in light of this limitation. Further studies would be needed to verify or complement the outcomes of this study.
According to the DHC assessment, almost a third of the evaluated sample was placed in grades 4 and 5, indicating great and very great orthodontic treatment need, respectively. Previous studies in young adults indicated that normative orthodontic treatment need ranged from 1.4% to 71.6% [15, 17–28, 33]; however, different indexes were used in the studies (Table 4). Some of these studies have even included young adults with a history of previous orthodontic treatment [18, 20, 21, 25, 27].
When only those studies using the DHC were compared, the frequency of treatment need in the present population was higher than those reported for Finns [21, 23] and Kuwaiti citizens [25], but smaller than that reported for male Asians [15] and Saudi citizens [33]. (Table 4) Different selected sample sizes and age ranges within the evaluated young adults might have contributed to the reported differences in normative orthodontic treatment need.
In Peru, a previous study [28] carried out with the same population of first-year university students used the Dental Aesthetic Index (DAI). Despite the broadly discussed differences between both indexes in relation to the occlusal traits included in the assessment [3, 4, 11, 34, 35], the frequency of students needing orthodontic treatment was very similar in both studies (32.6% versus the 29.9% reported here).
Dental crowding, increased overjet and hypodontia were the most frequently scored occlusal traits. Although the overall frequency of students presenting with dental crowding was 57.2%, a displacement of teeth greater than 4 mm was only found in 11.7% of the sample, which indicates a need for orthodontic treatment (grade 4). Therefore, the remainder of the students only had slight dental crowding (≤ 4 mm), which was classified as not having a significant need for orthodontic treatment. Similarly, only 6.0% of the students- and not 12.4%-presented an increased overjet greater than 6 mm, which indicated a definite treatment need (grades 4 and 5). The remaining 6.4% presented with a mildly increased overjet (>3.5 mm but ≤ 6 mm). Compared with these adjusted results, the frequency of students with hypodontia requiring pre-restorative orthodontics was high (6.4%). This would mean that increased overjet is the third most common occlusal trait for definite treatment need.
The present findings agree with those previously reported by Hassan [33], who found that dental crowding was the predominant occlusal trait in Kuwaiti citizens. In addition, Bernabé and Flores-Mir [28], using the DAI index, found that in the same population of Peruvian students malocclusion was characterized by a relative high frequency of missing teeth, significant dental crowding and inadequate posterior occlusal relationships. On the contrary, Kerosuo et al [23] and Soh and Sandham [15] have reported that dental crossbite and crowding, in that order, were the most common occlusal traits scoring for definite treatment need in Finnish and Asian young adults respectively.
When self-perceived orthodontic treatment need was evaluated by means of the AC of IOTN, only a few of the first-year students (1.8%) self-scored as presenting a definite need for orthodontic treatment (photos 8–10). This corroborates the presence of a skewed distribution toward the attractive end of the scale as has been reported in previous studies [23, 25, 27, 33].
A marked difference between normative (29.9%) and self-perceived (1.8%) treatment need in this population was detected. A possible explanation for which normatively defined need for orthodontic care was not matched by the perceived need is that the IOTN is a normative measure of something that is subjectively defined (aesthetics). Such a difference is supported by the conceptual distinction between health and disease [36]; while clinical indicators measure disease, which is a purely a biological concept, subjective indicators concentrate on health, a concept inclined more towards sociology and psychology [37].
Disease does not always negatively affect subjective perceptions of well-being, and even when it does, its impact depends on expectations, preferences, material, social and psychological resources and, more importantly, socially and culturally derived values [36, 37]. What is considered aesthetically pleasing in one culture will often not match that which is thought of as aesthetically pleasing in another. Thus the lack of perceived need in the population evaluated might be due to the fact that Peruvian students probably do not have the same notions of beauty as their British peers, where the index was developed.
The level of education may also be a factor influencing treatment need and demand. The present results were based on highly educated individuals, which might not be truly representative of the general young adult population. Further studies should assess the perception of malocclusion and the level of orthodontic awareness in children, adolescents and young adults in addition to treatment need, to provide more precise information for manpower planning for the delivery of orthodontic care.
Another possible explanation could be the low frequency of orthodontic treatment requested by the Peruvian population. In Peru, the orthodontist to population ratio is very low, approximately 1/450,000 in Lima, and completely delivered by the fee-for-service modality [28]. The availability of orthodontic services has been shown to affect self-satisfaction of dental appearance and the desire of treatment in young adults [15, 38]. Furthermore, Espeland et al [18, 19] have reported that untreated young adults living in areas with low orthodontic treatment frequency were generally less aware of their anterior occlusal traits in comparison to young adults in areas with a higher treatment frequency. Presumably, different norms for acceptable dental arrangement operate in both areas [19].
In the present study sex, age and socio-economic status of the Peruvian first-year university students did not influence normative or self-perceived orthodontic treatment need. According to our literature review, the role of these factors in treatment need varies. Although sex seems to be the most studied covariable, findings still are contradictory. In a previous study, males were assessed by professionals as having need for treatment significantly more frequently than females [23], but others do not support this difference [21, 25]. Also, some studies have shown that females are more selective in their self-perception than males, generally valuing dental appearance higher than males [2, 39].
Stenvik et al [22] found that dissatisfaction with dental appearance and desire for orthodontic treatment decreased with increasing age, but more studies are required to assess age-related changes, which should be conducted longitudinally. The absence of differences in the distribution of normative and self-perceived need for orthodontic treatment according to socio-economic status is in agreement with some authors [25, 40]; however, several other studies have reported differences between different socio-economic statuses [41, 42]. It is possible that a standardization of the criteria used to define social class will be needed before a summary of the different findings could be made [11].
According to the present findings, a third of the Peruvian first-year university young adults should receive orthodontic treatment to avoid the associated health risks generated by malocclusions [40], unfortunately not many of them have access to orthodontic treatment. One possible explanation may be that orthodontic concern is still given low priority in the oral health care system in Peru. Although there is a public health system, the lack of resources makes the funds available for dentistry scarce. Thus, orthodontic services are not readily available and accessible to the general population.
In that context, the current findings could be useful to plan orthodontic services for this specific university population, where an oral health insurance program exists including basic restorative treatment. Nevertheless, cost-benefit and cost-effectiveness analyses should be carried out first to assess the suitability of such a service.
In summary, further studies are required to improve our understanding of normative and self-perceived need for orthodontic treatment, especially in developing countries where the low frequency of orthodontic care added to the almost 100% private delivery of orthodontics have a significant influence. Hence, different factors than those reported in North American and European countries could be influencing the demand and delivery of orthodontic care. It may even be necessary to use more than one index in an epidemiological study to gather all the required information.
Conclusion
-
Approximately one-third of the evaluated Peruvian first-year university students presented a normative definite need.
-
Only 1.8% self-perceived a need for orthodontic treatment need.
-
Dental crowding greater than 4 mm, hypodontia, and increased overjet greater than 6 mm were the main reasons for determining orthodontic treatment need.
-
Gender, age and socio-economic status of the students did not influence the frequency distribution of normative and self-perceived orthodontic treatment need.
References
Abu Alhaija ES, Al-Nimri KS, Al-Khateeb SN: Orthodontic treatment need and demand in 12-14-year-old north Jordanian school children. Eur J Orthod. 2004, 26: 261-263. 10.1093/ejo/26.3.261.
Shaw WC, O'Brien KD, Richmond S: Quality control in orthodontics: factors influencing the receipt of orthodontic treatment. Br Dent J. 1991, 170: 66-68. 10.1038/sj.bdj.4807399.
Shaw WC, Richmond S, O'Brien KD: The use of occlusal indices: a European perspective. Am J Orthod Dentofacial Orthop. 1995, 107: 1-10. 10.1016/S0889-5406(95)70151-6.
Beglin FM, Firestone AR, Vig KW, Beck FM, Kuthy RA, Wade D: A comparison of the reliability and validity of 3 occlusal indexes of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2001, 120: 240-246. 10.1067/mod.2001.116401.
Jarvinen S: Indexes for orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2001, 120: 237-239. 10.1067/mod.2001.114830.
Brook PH, Shaw WC: The development of an index of orthodontic treatment priority. Eur J Orthod. 1989, 11: 309-320.
So LL, Tang EL: A comparative study using the Occlusal Index and the Index of Orthodontic Treatment Need. Angle Orthod. 1993, 63: 57-64; discussion 65-6.
Younis JW, Vig KW, Rinchuse DJ, Weyant RJ: A validation study of three indexes of orthodontic treatment need in the United States. Community Dent Oral Epidemiol. 1997, 25: 358-362. 10.1111/j.1600-0528.1997.tb00955.x.
Cooper S, Mandall NA, DiBiase D, Shaw WC: The reliability of the Index of Orthodontic Treatment Need over time. J Orthod. 2000, 27: 47-53. 10.1093/ortho/27.1.47.
Bentele MJ, Vig KW, Shanker S, Beck FM: Efficacy of training dental students in the index of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2002, 122: 456-462. 10.1067/mod.2002.126895.
Kuijpers MA, Kiekens RM: [Research methods in dentistry 10. Assessment of orthodontic treatment need]. Ned Tijdschr Tandheelkd. 2005, 112: 206-210.
Evans R, Shaw W: Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod. 1987, 9: 314-318.
Tang EL, So LL: Correlation of orthodontic treatment demand with treatment need assessed using two indices. Angle Orthod. 1995, 65: 443-450.
Espeland LV, Stenvik A: Perception of personal dental appearance in young adults: relationship between occlusion, awareness, and satisfaction. Am J Orthod Dentofacial Orthop. 1991, 100: 234-241.
Soh J, Sandham A: Orthodontic treatment need in Asian adult males. Angle Orthod. 2004, 74: 769-773.
Albino JE, Tedesco LA, Phipps GT: Social and psychological problems of adolescence and their relevance to dental care. Int Dent J. 1982, 32: 184-193.
Salonen L, Mohlin B, Gotzlinger B, Hellden L: Need and demand for orthodontic treatment in an adult Swedish population. Eur J Orthod. 1992, 14: 359-368.
Espeland LV, Stenvik A, Medin L: Concern for dental appearance among young adults in a region with non-specialist orthodontic treatment. Eur J Orthod. 1993, 15: 17-25.
Espeland LV, Gronlund G, Stenvik A: Concern for dental appearance among Norwegian young adults in region with low uptake of orthodontic treatment. Community Dent Oral Epidemiol. 1993, 21: 151-157. 10.1111/j.1600-0528.1993.tb00741.x.
Searcy VL, Chisick MC: Perceived, desired, and normatively determined orthodontic treatment needs in male US Army recruits. Community Dent Oral Epidemiol. 1994, 22: 437-440. 10.1111/j.1600-0528.1994.tb00793.x.
Tuominen ML, Nystrom M, Tuominen RJ: Subjective and objective orthodontic treatment need among orthodontically treated and untreated Finnsih adolescents. Community Dent Oral Epidemiol. 1995, 23: 286-290. 10.1111/j.1600-0528.1995.tb00250.x.
Stenvik A, Espeland L, Berset GP, Eriksen HM: Attitudes to malocclusion among 18- and 35-year-old Norwegians. Community Dent Oral Epidemiol. 1996, 24: 390-393. 10.1111/j.1600-0528.1996.tb00885.x.
Kerosuo H, Kerosuo E, Niemi M, Simola H: The need for treatment and satisfaction with dental appearance among young Finnish adults with and without a history of orthodontic treatment. J Orofac Orthop. 2000, 61: 330-340. 10.1007/PL00001903.
Onyeaso CO, Arowojolu MO, Taiwo JO: Periodontal status of orthodontic patients and the relationship between dental aesthetic index and community periodontal index of treatment need. Am J Orthod Dentofacial Orthop. 2003, 124: 714-720. 10.1016/j.ajodo.2003.01.002.
Kerosuo H, Al Enezi S, Kerosuo E, Abdulkarim E: Association between normative and self-perceived orthodontic treatment need among Arab high school students. Am J Orthod Dentofacial Orthop. 2004, 125: 373-378. 10.1016/j.ajodo.2003.04.009.
Baca-Garcia A, Bravo M, Baca P, Baca A, Junco P: Malocclusions and orthodontic treatment needs in a group of Spanish adolescents using the Dental Aesthetic Index. Int Dent J. 2004, 54: 138-142.
Klages U, Bruckner A, Zentner A: Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J Orthod. 2004, 26: 507-514. 10.1093/ejo/26.5.507.
Bernabé E, Flores-Mir C: Orthodontic treatment need in Peruvian young adults evaluated through Dental Aesthetic Index. Angle Orthod. 2006, 76: 417-421.
Flores-Mir C, Major PW, Salazar FR: Self-perceived orthodontic treatment need evaluated through 3 scales in a university population. J Orthod. 2004, 31: 329-34; discussion 302. 10.1179/146531204225020644.
Bernabé E, Flores-Mir C: Estimating arch length discrepancy through Little's irregularity index for epidemiological use. Eur J Orthod. 2005, (in press):
Bernabé E, Kresevic VD, Cabrejos SC, Flores-Mir F, Flores-Mir C: Dental aesthetic self-perception in young adults with or without previous orthodontic treatment. Angle Orthod. 2006, 76: 412-416.
Grzywacz I: The value of the aesthetic component of the Index of Orthodontic Treatment Need in the assessment of subjective orthodontic treatment need. Eur J Orthod. 2003, 25: 57-63. 10.1093/ejo/25.1.57.
Hassan AH: Orthodontic treatment needs in the western region of Saudi Arabia: a research report. Head Face Med. 2006, 2: 2-10.1186/1746-160X-2-2.
Jenny J, Cons NC: Comparing and contrasting two orthodontic indices, the Index of Orthodontic Treatment need and the Dental Aesthetic Index. Am J Orthod Dentofacial Orthop. 1996, 110: 410-416. 10.1016/S0889-5406(96)70044-6.
Johnson M, Harkness M, Crowther P, Herbison P: A comparison of two methods of assessing orthodontic treatment need in the mixed dentition: DAI and IOTN. Aust Orthod J. 2000, 16: 82-87.
Locker D: The burden of oral disorders in a population of older adults. Community Dent Health. 1992, 9: 109-124.
Tsakos G, Marcenes W, Sheiham A: Evaluation of a modified version of the index of Oral Impacts On Daily Performances (OIDP) in elderly populations in two European countries. Gerodontology. 2001, 18: 121-130. 10.1111/j.1741-2358.2001.00121.x.
Espeland L, Stenvik A: Residual need in orthodontically untreated 16-to-20-years-olds from areas with different treatment rates. Eur J Orthod. 1999, 21: 523-531. 10.1093/ejo/21.5.523.
Tuominen ML, Tuominen RJ, Nystrom ME: Subjective orthodontic treatment need and perceived dental appearance among young Finnish adults with and without previous orthodontic treatment. Community Dent Health. 1994, 11: 29-33.
Otuyemi OD, Ogunyinka A, Dosumu O, Cons NC, Jenny J: Malocclusion and orthodontic treatment need of secondary school students in Nigeria according to the dental aesthetic index (DAI). Int Dent J. 1999, 49: 203-210.
Tickle M, Kay EJ, Beran D: Socio-economic status and orthodontic treatment need. Community Dent Oral Epidemiol. 1999, 27: 413-418.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
EB performed the statistical analysis and participated in the conception and draft of the manuscript.
CF conceived the study, participated in the study design, helped with the data collection, and coordinated and helped to draft the manuscript.
All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Bernabé, E., Flores-Mir, C. Normative and self-perceived orthodontic treatment need of a Peruvian university population. Head Face Med 2, 22 (2006). https://doi.org/10.1186/1746-160X-2-22
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1746-160X-2-22