
Abstract
Background
Urachal carcinoma is an uncommon neoplasm associated with poor prognosis.
Case presentation
A 45-year-old man was admitted with complaints of abdominal pain and pollakisuria. A soft mass was palpable under his navel. TC-scan revealed a 11 × 6 cm tumor, which was composed of a cystic lesion arising from the urachus and a solid mass component at the urinary bladder dome. The tumor was removed surgically. Histological examination detected poor-differentiated adenocarcinoma, which had invaded the urinary bladder. The patient has been followed up without recurrence for 6 months.
Conclusion
The urachus is the embryological remnant of urogenital sinus and allantois. Involution usually happens before birth and urachus is present as a median umbilical ligament. The pathogenesis of urachal tumours is not fully understood. Surgery is the treatment of choice and role of adjuvant treatment is not clearly understood.
Similar content being viewed by others


Background
Urachal carcinoma is an uncommon neoplasm associated with poor prognosis. The estimated annual incidence of urachal carcinoma in the general population is one in 5 million, or 0.01% of all cancers in adults. Urachal carcinoma has been estimated to comprise 0.17-0.34% of all bladder cancers [1]. Adenocarcinoma is common among urachal carcinomas, whereas squamous cell carcinoma (SCC) is very rare. We report a case of primary adenocarcinoma of the urachus.
Case presentation
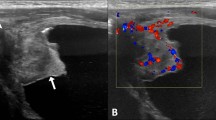
A 45-year-old man was referred to our hospital with complaints of micturition pain of 5 months' duration, and lower abdominal pain and pollakisuria of 1 month's duration. A physical examination revealed a soft tender mass under his navel. Periumbilical discharge was not recognized. Laboratory data: hemoglobin, 15.9 g/dL; erythrocyte count, 4865000/mL; leukocyte count, 11600/mL; platelet count, 259000/mL. CEA: 5.1 ng/ml. Urinalysis: hemoglobin (++). Urine cytology: negative. Cystoscopy detected mucosal edema and erosion at the bladder dome. TC-scan showed a soft-tissue mass along the umbilicus, which extended from the bladder dome to the posterior wall of the bladder and the peritoneum. The size of the tumor was 11 × 6 cm (Fig. 1).

TC-scan: a soft-tissue mass along the umbilicus, which extended from the bladder dome to the posterior wall of the bladder and the peritoneum. The size of the tumor was 11 × 6 cm
It was noted that the tumor extended from the bladder dome to the umbilicus. Open laparotomy revealed bladder edema and intraoperative cytological examination was negative. The tumor was removed en bloc together with the umbilicus, lateral umbilical ligaments, adjacent peritoneum and bladder dome (Fig. 2).

Tumor removed en bloc together with the umbilicus, lateral umbilical ligaments, adjacent peritoneum and bladder dome
On gross inspection, the suprapubic mass consisted of slid and cystic lesions. Microscopically, poor-differentiated adenocarcinoma of the solid lesion was observed (Fig. 3). According to CT scan and pathologist report the tumor can be staged as Sheldon II, confined only to urachus. The grading of this tumor was impossible.

Macroscopic aspect of tumor: the suprapubic mass consisted of slid and cystic lesions
Tumor cells not invaded the bladder. Follow-up abdominal computerized tomography at 6 months showed no tumor recurrence.
Discussion
The urachus is the embryological remnant of urogenital sinus and allantois. Involution usually happens before birth and urachus is present as a median umbilical ligament. The pathogenesis of urachal tumours is not fully understood. It is believed that urachal carcinomas arise from malignant transformation of columnar or glandular metaplastic epithelium. They lie in the space of Retzius, between transversalis fascia anteriorly and peritoneum posteriorly, extending from the dome of the bladder to the umbilicus.
Urachal cancer was first described in 1863 by Hue and Jacquin in a report translated and summarized by Sheldon [1]. Although this tumour has now become a recognisable 'neoplastic entity', its origin and pathophysiology remain unknown [2]. The estimated annual incidence of urachal carcinoma is 0.01% of all cancers in adults. The incidence of the disease ranges from 0.55 to 1.20% of bladder tumors in Japan and 0.07-0.70% of bladder tumors in Western countries. Histopathologically, adenocarcinoma accounts for 80-90% of the tumors. The 5-year cancer-specific survival rate, depending of pathologic stage [3], is 6% in Japan [4] but Ashley [5] in a 50 years of experience at Mayo Clinic reported a 5-year cancer-specific survival rate of 49%. The poor prognosis of this cancer is due to: (a) late presentation of symptoms leading to advanced stage at diagnosis; (b) a propensity for early local invasion; and (c) distal metastasis.
The new Mayo staging system was less complicated than the Sheldon system, although both systems predicted cancer-specific mortality equally well. Positive surgical margins (hazard ratio [HR], 4.7), high tumor grade (HR, 3.6), positive local lymph nodes (HR, 5.1), metastases at diagnosis (HR, 3.3), advanced tumor stage (HR, 4.8), failure to perform umbilectomy (HR, 3.0), and primary radiation therapy (HR, 2.9) were all univariately associated with death (P < .05). Only grade and margins were significant in the multivariate analysis. Modern therapeutic regimens have offered minimal benefit, especially when unresectable. No survival benefit was noted for lymphadenectomy or adjuvant therapy. Salvage surgery resulted in a long-term cure for 50% of patients who had local recurrences. No effective treatment was identified for patients with metastatic UrC. The question as to whether partial or radical cystectomy is suitable for localised disease is difficult to answer since urachal tumours are rare. Furthermore, within this group, urachal adenocarcinoma is uncommon in those under 40 years. However, in order to evaluate which surgical approach is correct or whether new chemotherapeutic agents will induce objective responses and improve long-term survival requires co-operation between physicians and centres internationally so that larger studies can be conducted. This approach can only benefit patients [6–8].
Conclusion
The urachus is the embryological remnant of urogenital sinus and allantois. Involution usually happens before birth and urachus is present as a median umbilical ligament. The pathogenesis of urachal tumours is not fully understood. Surgery is the treatment of choice and role of adjuvant treatment is not clearly understood.
Consent
Written informed consent was obtained from the patient for publication of this case report. A copy of the consent is available with editorial office
Change history
29 June 2021
A Correction to this paper has been published: https://doi.org/10.1186/s12957-021-02294-3
References
Sheldon CA, Clayman RV, Gonzalez R, Williams RD, Fraley EE: Malignant urachal lesions. J Urol. 1984, 131: 1-8.
Mostfi FK, Thomson RV, Dean AL: Mucinous Adenocarcinoma of the urinary bladder. Cancer. 1955, 8: 741-58. 10.1002/1097-0142(1955)8:4<741::AID-CNCR2820080417>3.0.CO;2-C.
Gopalan A, Sharp DS, Fine SW, Tickoo SK, Herr HW, Reuter VE, Olgac S: Urachal carcinoma: a clinicopathologic analysis of 24 cases with outcome correlation. Am J Surg Pathol. 2009, 33 (5): 659-68. 10.1097/PAS.0b013e31819aa4ae.
Ghazizadeh M, Yamamoto S, Kurokawa K: Clinical features of urachal carcinoma in Japan: review of 157 patients. Urol Res. 1983, 11: 235-8. 10.1007/BF00272286.
Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, Zincke H: Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer. 2006, 107: 712-20. 10.1002/cncr.22060.
Tian J, Ma JH, Li CL, Xiao ZD: Urachal mass in adults: clinical analysis of 33 cases. Zhonghua Yi Xue Za Zhi. 2008, 88 (12): 820-2.
Paras FA, Maclennan GT: Urachal adenocarcinoma. J Urol. 2008, 180 (2): 720-10.1016/j.juro.2008.05.039.
Sugarbaker PH, Verghese M, Yan TD, Brun E: Managment of mucinous urachal neoplasm presenting as pseudomyxoma peritonei. Tumori. 2008, 94 (5): 732-6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
SS, ER, ER, RS and VF are surgeons of the Unit of Surgical Oncology (Chief: VF) and have performed the operation. LV is General Psysician of the patient. VG and CF are radiologists of the Department of Radiology. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Scabini, S., Rimini, E., Romairone, E. et al. RETRACTED ARTICLE: Urachal tumour: case report of a poorly understood carcinoma. World J Surg Onc 7, 82 (2009). https://doi.org/10.1186/1477-7819-7-82
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7819-7-82