
Abstract
Background
A low cerebrospinal fluid (CSF) white-blood cell count (WBC) has been identified as an independent risk factor for adverse outcome in adults with bacterial meningitis. Whereas a low CSF WBC indicates the presence of sepsis with early meningitis in patients with meningococcal infections, the relation between CSF WBC and outcome in patients with pneumococcal meningitis is not understood.
Methods
We examined the relation between CSF WBC, bacteraemia and sepsis in a prospective cohort study that included 352 episodes of pneumococcal meningitis, confirmed by CSF culture, occurring in patients aged >16 years.
Results
CSF WBC was recorded in 320 of 352 episodes (91%). Median CSF WBC was 2530 per mm3 (interquartile range 531–6983 per mm3) and 104 patients (33%) had a CSF WBC <1000/mm3. Patients with a CSF WBC <1000/mm3 were more likely to have an unfavourable outcome (defined as a Glasgow Outcome Scale score of 1–4) than those with a higher WBC (74 of 104 [71%] vs. 87 of 216 [43%]; P < 0.001). CSF WBC was significantly associated with blood WBC (Spearman's test 0.29), CSF protein level (0.20), thrombocyte count (0.21), erythrocyte sedimentation rate (-0.15), and C-reactive protein levels (-0.18). Patients with a CSF WBC <1000/mm3 more often had a positive blood culture (72 of 84 [86%] vs. 138 of 196 [70%]; P = 0.01) and more often developed systemic complications (cardiorespiratory failure, sepsis) than those with a higher WBC (53 of 104 [51%] vs. 69 of 216 [32%]; P = 0.001). In a multivariate analysis, advanced age (Odds ratio per 10-year increments 1.22, 95%CI 1.02–1.45), a positive blood culture (Odds ratio 2.46, 95%CI 1.17–5.14), and a low thrombocyte count on admission (Odds ratio per 100,000/mm3 increments 0.67, 95% CI 0.47–0.97) were associated with a CSF WBC <1000/mm3.
Conclusion
A low CSF WBC in adults with pneumococcal meningitis is related to the presence of signs of sepsis and systemic complications. Invasive pneumococcal infections should possibly be regarded as a continuum from meningitis to sepsis.
Similar content being viewed by others


Background
Bacterial meningitis is a life-threatening disease [1, 2]. Recently we evaluated clinical features and prognostic factors in a prospective cohort study of 696 episodes of community-acquired acute bacterial meningitis [3]. The most common pathogens were Streptococcus pneumoniae and Neisseria meningitidis. The mortality rate was 21 percent and was higher among patients with pneumococcal meningitis than among those with meningococcal meningitis (30% vs. 7%, P < 0.001). The outcome was unfavourable in 34 percent of episodes and the strongest risk factors for an unfavourable outcome were symptoms indicative of systemic compromise, a low level of consciousness, infection with S. pneumoniae, and a low cerebrospinal fluid (CSF) white-blood cell count (WBC). The relation between unfavourable outcome and a low CSF WBC has been described previously in both patients with N. meningitidis and S. pneumoniae meningitis [3–6]. In patients with meningococcal meningitis, a low CSF WBC indicates the presence of sepsis with early meningitis [3]. The relation between CSF WBC and outcome in patients with pneumococcal meningitis is not understood [2–4]. A recent study in experimental pneumococcal meningitis suggested that an attenuated CSF pleocytosis was likely the result of a decrease in blood WBC induced by bacteraemia [7]. This suggests that a low CSF WBC in patients with pneumococcal meningitis may indicate the presence of sepsis, analogous to meningococcal disease. The aim of the present study was to examine the relation between CSF pleocytosis, bacteraemia and sepsis in a prospective cohort study of adults with pneumococcal meningitis.
Methods
The Dutch Meningitis Cohort Study, a prospective nationwide observational cohort study in the Netherlands, includes 696 episodes of community-acquired bacterial meningitis [3]. Inclusion and exclusion criteria are described more extensively elsewhere [3]. In summary, eligible patients were aged >16 years and had CSF culture proven bacterial meningitis. CSF culture yielded S. pneumoniae in 352 episodes (51%), N. meningitidis in 257 episodes (37%), and other bacteria in 87 episodes (13%) [3]. The Dutch Meningitis Cohort Study was approved by our ethics committee and written informed consent was obtained from participating patients or their legally authorised representatives. Information was collected by means of a case record form. Patients using immunosuppressive drugs and patients with diabetes mellitus, alcoholism, asplenia or infection with the human immunodeficiency virus were considered immunocompromised. Fever was defined as a body temperature ≥38°C. A diastolic blood pressure <60 mm Hg was used as a surrogate marker for septic shock. Patients underwent a neurological examination at discharge and outcome was graded by means of the Glasgow Outcome Scale (GOS). This is a well validated measurement scale with scores varying from 1 (indicating death) to 5 (good recovery) [3, 8]. A favourable outcome was defined as a score of 5, and an unfavourable outcome as a score 1–4.
For nonparametric testing, χ2- or Fisher's exact statistics were used. Correlation between parameters was performed by non-parametric Spearman rank test. We used logistic regression analysis to calculate odds ratios and 95% confidence intervals (CI) to assess the strength of the association between potential factors and a low CSF WBC (defined as a CSF WBC <1000/mm3). Although the median percentage of missing values for potential factors was low (2%), data were complete for all factors in only 175 episodes (50%) [4]. Missing values were imputed by use of multivariate normal distributions, and the coefficients of ten rounds of imputation were combined to obtain the final estimates from the multivariate model [3, 4]. All statistical tests were two-tailed, and we considered a P value less than 0.05 as statistically significant. All analyses were undertaken with SAS software (version 9.11).
Results
A total of 352 episodes of pneumococcal meningitis occurred in 343 patients; 9 patients had a second episode during the study period. Characteristics of the study population, clinical course and outcome are described more extensively elsewhere [3, 4].
All patients underwent lumbar puncture. CSF WBC was determined in 320 episodes (91%); median CSF WBC was 2530 per mm3 (interquartile range 531 to 6983 per mm3) and in 104 of 320 episodes (33%) CSF WBC was <1000/mm3 (Table 1). Patients with a CSF WBC <1000/mm3 were significantly older than those with a higher CSF WBC (mean age 62 vs. 57 years; P = 0.01), were less likely to have complaints <24 hours before admission (39 of 97 [40%] vs. 110 of 200 [55%]; P = 0.02), more often had a positive blood culture (72 of 84 [86%] vs. 138 of 196 [70%]; P = 0.01) and an immunocompromised status (31 of 104 [30%] vs. 39 of 215 [18%]; P = 0.02). Patients with a CSF WBC below or above 1000 per mm3 had similar proportions of patients with fever, tachycardia (heart rate >120 beats/min) or diastolic blood pressure <60 mmHg on admission. Although several factors were significantly associated with a low CSF WBC in the univariate analysis, most factors were not significant in the multivariate analysis. In the multivariate model, advanced age (Odds ratio per 10-year increments 1.22, 95%CI 1.02–1.45), a positive blood culture (Odds ratio 2.46, 95%CI 1.17–5.14), and a low thrombocyte count on admission (Odds ratio per 100,000/mm3 increments 0.67, 95%CI 0.47–0.97) were significantly associated with a CSF WBC <1000/mm3.
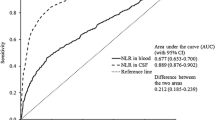
To further explore our data we performed an analysis of correlations between indexes of inflammations in CSF and blood (Table 2). There was a significant correlation between CSF and blood WBC (Spearman's test 0.29, P < 0.001). CSF WBC was also significantly associated with CSF protein level (Spearman's test 0.20, P = 0.001), thrombocyte count (0.21, P < 0.001) and indexes of inflammation in the blood: erythrocyte sedimentation rate (ESR, -0.15, P = 0.02), and C-reactive protein level (CRP, -0.18, P = 0.02). Blood WBC was significantly associated with thrombocyte count (Spearman's test 0.35, P < 0.001) and ESR (-0.12, P = 0.04), but not with CRP, CSF protein or CSF glucose level.
Episodes with a CSF WBC <1000/mm3 were more likely to develop systemic complications (cardiorespiratory failure and/or sepsis) during clinical course than those with higher CSF WBC (53 of 104 [51%] vs. 69 of 216 [32%]; P = 0.001). The proportion of episodes with neurological complications (seizures, impairment of consciousness, or focal neurological abnormalities) was similar in episodes with a CSF WBC below and above 1000 cells per mm3 (84 of 104 [81%] vs. 158 of 216 [73%], respectively, P = 0.14).
Discussion
Our findings indicate that a low CSF WBC in adults with pneumococcal meningitis is related to the presence of signs of sepsis and systemic complications. This is analogous to findings in patients with meningococcal meningitis [3]. Therefore, invasive pneumococcal infections should possibly also be regarded as a continuum from meningitis to sepsis, rather than of infections in isolated systemic and central nervous system compartments.
Leukocyte recruitment is a key aspect of the host response against invading micro-organisms [2]. In experimental pneumococcal meningitis blocking of leukocyte accumulation in the CSF augmented bacteraemia and increased mortality due to severe sepsis [9]. Another study in animals with pneumococcal meningitis showed a relation among a large CSF bacterial load, lack of response of CSF leukocytes and intracranial complications [10]. This suggests that low CSF WBC is related to excessive bacterial growth. In clinical studies, a low CSF WBC is a strong individual predictor of unfavourable outcome [3–5]. A recent study in experimental pneumococcal meningitis explored the role of systemic infection on meningeal inflammation [7]. In this study, meningitis was induced in rabbits by intracisternal injection of ~1 × 106 colony forming units S. pneumoniae type 3; WBC and bacterial concentrations were regularly determined in blood and CSF [7]. The animals were either provided with a similar dose of pneumococci intravenously at 0 hour (bacteraemic rabbits), pre-treated with paraformaldehyde-killed pneumococci (immunized rabbits) or not treated further (controls). Bacteraemic rabbits showed a decrease in blood WBC between 10–16 hours after inoculation and had an attenuated CSF pleocytosis as compared to the other groups between 12–16 hours from time of infection.
A weak leukocyte response in the CSF was significantly associated with advanced age. In a previous analysis of the Dutch Meningitis Cohort study, systemic complications have been noted as the leading causes of death in elderly patients with bacterial meningitis [11]. In the present study we lacked data for analyzing international accepted criteria of sepsis and septic shock [12]. We used a low diastolic blood pressure as a surrogate marker, which is a limitation of our study. Our results show a weak leukocyte response in the CSF was associated with bacteraemia and other factors related to systemic compromise; however, the association with a low blood WBC on admission did not reach statistical significance in our multivariate model. Therefore, a direct causal relationship between an attenuated CSF pleocytosis and a decrease in blood WBC induced by bacteraemia remains speculative.
A recent randomised, placebo-controlled trial involving 301 adults with suspected meningitis in combination with cloudy cerebrospinal fluid, bacteria in the CSF on Gram's staining, or a CSF WBC of more than 1000 per mm3, showed that adjunctive treatment with dexamethasone before or with the first dose of antimicrobial therapy reduced the risk of unfavourable outcome from 25 percent to 15 percent (number needed to treat, 10 patients) [13]. In this study, the effect of dexamethasone on outcome was most striking in patients with pneumococcal meningitis, in which mortality was decreased from 34 to 14 percent. A post hoc analysis of this study showed that the beneficial effect of dexamethasone on mortality in pneumococcal meningitis was attributable to a reduction in systemic complications, rather than neurological complications [14]. In a categorization of death of patients with pneumococcal meningitis who died within 14 days after admission, the percentage of patients who died due to neurological causes was similar between groups. The percentage of patients who died due to a systemic cause was significantly smaller in the dexamethasone group than in the placebo group (2 vs. 16%; Relative risk 0.11; 95%CI 0.04–0.25). The systemic complications that were potentially preventable by dexamethasone were pulmonary complications and septic shock [14]. As one of the inclusion criteria was a CSF WBC of more than 1000 per mm3, a subgroup analysis of patients included in this study with low CSF WBC on the effect of dexamethasone cannot be performed. In the current study, patients did not routinely receive corticosteroids [3]. This may well have influenced our results concerning the relation with development of complications during clinical course. However, this has not influenced our results on the correlation between CSF WBC, blood WBC and other indexes of inflammation in the blood since adjunctive dexamethasone is generally started after blood and CSF samples are obtained.
Conclusion
We found a significant correlation between CSF WBC, blood WBC and other indexes of inflammation in the blood. In addition, a CSF WBC below 1000 per mm3 was a risk factor for the development of systemic complications in patients with pneumococcal meningitis. These findings suggest that a low CSF WBC may be due the presence of bacteraemia and sepsis with early meningitis and invasive pneumococcal infections should possibly be regarded as a continuum from meningitis to sepsis.
References
van de Beek D, de Gans J, Tunkel AR, Wijdicks EF: Community-acquired bacterial meningitis in adults. N Engl J Med. 2006, 354: 44-53. 10.1056/NEJMra052116.
Weisfelt M, de Gans J, van der Poll T, van de Beek D: Pneumococcal meningitis in adults: new approaches to management and prevention. Lancet Neurol. 2006, 5: 332-342. 10.1016/S1474-4422(06)70409-4.
van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M: Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004, 351: 1849-1859. 10.1056/NEJMoa040845.
Weisfelt M, van de Beek D, Spanjaard L, Reitsma JB, de Gans J: Clinical features, complications, and outcome in adults with pneumococcal meningitis: a prospective case series. Lancet Neurol. 2006, 5: 123-129. 10.1016/S1474-4422(05)70288-X.
Kastenbauer S, Pfister HW: Pneumococcal meningitis in adults: spectrum of complications and prognostic factors in a series of 87 cases7. Brain. 2003, 126: 1015-1025. 10.1093/brain/awg113.
McMillan DA, Lin CY, Aronin SI, Quagliarello VJ: Community-acquired bacterial meningitis in adults: categorization of causes and timing of death1. Clin Infect Dis. 2001, 33: 969-975. 10.1086/322612.
Ostergaard C, O'reilly T, Brandt C, Frimodt-Moller N, Lundgren JD: The Influence of the blood bacterial load on the meningeal inflammatory response in Streptococcus pneumoniae meningitis. BMC Infect Dis. 2006, 6: 78-10.1186/1471-2334-6-78.
Jennet B, Teasdale G: Management of head injuries. Philadelphia: F A Davies. 1998
Brandt CT, Lundgren JD, Frimodt-Moller N, Christensen T, Benfield T, Espersen F, Hougaard DM, Ostergaard C: Blocking of leukocyte accumulation in the cerebrospinal fluid augments bacteremia and increases lethality in experimental pneumococcal meningitis. J Neuroimmunol. 2005, 166: 126-131. 10.1016/j.jneuroim.2005.05.014.
Tauber MG, Kennedy SL, Tureen JH, Lowenstein DH: Experimental pneumococcal meningitis causes central nervous system pathology without inducing the 72-kd heat shock protein4. Am J Pathol. 1992, 141: 53-60.
de Gans J, van de Beek D: Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002, 347: 1549-1556. 10.1056/NEJMoa021334.
Weisfelt M, van de Beek D, Spanjaard L, Reitsma JB, de Gans J: Community-acquired bacterial meningitis in older people. J Am Geriatr Soc. 2006, [E-pub ahead of print]
Abraham E, Matthay MA, Dinarello CA, Vincent JL, Cohen J, Opal SM, Glauser M, Parsons P, Fisher CJ, Repine JE: Consensus conference definitions for sepsis, septic shock, acute lung injury, and acute respiratory distress syndrome: time for a reevaluation. Crit Care Med. 2000, 28: 232-5. 10.1097/00003246-200001000-00039.
van de Beek D, de Gans J: Dexamethasone and pneumococcal meningitis. Ann Intern Med. 2004, 141: 327-
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/6/149/prepub
Acknowledgements
We are indebted to many physicians in the Netherlands who participated in the Dutch Meningitis Cohort Study.
Financial support: The Dutch Meningitis Cohort Study was in part supported by a research grant of Roche Pharmaceuticals, The Netherlands. The study was designed, conducted, and analysed independently of the sponsor.
Research grants received: J. de Gans received funding support from Baxter BV. D. van de Beek received funding support from the Meningitis Research Foundation, UK, and Meerwaldt Foundation, The Netherlands; and is supported by a personal grant of the Netherlands Organization for Health Research and Development (ZonMw), Netherlands; NWO-Rubicon grant 2006 (019.2006.1.310.001).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
MW and DvdB participated in the design and coordination of the study, performed the statistical analysis, and participated in the writing of the article. JdG and LS participated in the design and coordination of the study and in the writing of the article. JBR participated in the statistical analysis and in critical revisions of the manuscript for important intellectual content. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Weisfelt, M., van de Beek, D., Spanjaard, L. et al. Attenuated cerebrospinal fluid leukocyte count and sepsis in adults with pneumococcal meningitis: a prospective cohort study. BMC Infect Dis 6, 149 (2006). https://doi.org/10.1186/1471-2334-6-149
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-6-149