
Abstract
Background
Asymptomatic subjects at intermediate coronary risk may need diagnostic testing for risk stratification. Both measurement of coronary calcium scores and exercise testing are well established tests for this purpose. However, it is not clear which test should be preferred as initial diagnostic test. We evaluated the prevalence of documented coronary artery disease (CAD) according to calcium scores and exercise test results.
Methods
Asymptomatic subjects with ST-T changes on a rest ECG were selected from the population based PREVEND cohort study and underwent measurement of calcium scores by electron beam tomography and exercise testing. With calcium scores ≥10 or a positive exercise test, myocardial perfusion imaging (MPS) or coronary angiography (CAG) was recommended. The primary endpoint was documented obstructive CAD (≥50% stenosis).
Results
Of 153 subjects included, 149 subjects completed the study protocol. Calcium scores ≥400, 100–399, 10–99 and <10 were found in 16, 29, 18 and 86 subjects and the primary endpoint was present in 11 (69%), 12 (41%), 0 (0%) and 1 (1%) subjects, respectively. A positive, nondiagnostic and negative exercise test was present in 33, 27 and 89 subjects and the primary endpoint was present in 13 (39%), 5 (19%) and 6 (7%) subjects, respectively. Receiver operator characteristics analysis showed that the area under the curve, as measure of diagnostic yield, of 0.91 (95% CI 0.84–0.97) for calcium scores was superior to 0.74 (95% CI 0.64–0.83) for exercise testing (p = 0.004).
Conclusion
Measurement of coronary calcium scores is an appropriate initial non-invasive test in asymptomatic subjects at increased coronary risk.
Similar content being viewed by others


Background
In selected asymptomatic subjects with an intermediate coronary risk profile, non-invasive testing may be required for coronary risk stratification [1–5]. Guidelines recommend the use of exercise testing [2, 6, 7] and measurement of coronary calcium scores [8], since the predictive values of both non-invasive tests for future coronary events have been well established in asymptomatic subjects at intermediate risk [7, 9–11]. However, guidelines do not recommend one of these tests as initial screening tool in these subjects. Although an abnormal exercise test result is widely accepted as indication for coronary angiography (CAG)[12], the indications for an invasive diagnostic or therapeutic procedure have not yet been defined for subjects with high calcium scores. This may be of particular importance for subjects with calcium scores ≥400, since these subjects are at a high annual risk of cardiac events of 4.8% [9]. So far, no head to head studies have compared exercise testing with measurement of calcium scores as initial tool in the evaluation of coronary artery disease (CAD).
Our aim was to investigate the diagnostic yield of coronary calcium scores and exercise testing in asymptomatic subjects with an intermediate coronary risk profile. Therefore, in a population based cohort study, all 12-lead rest ECGs with ST depression (defined as Minnesota codes 4.1-2 (>0.5 mm ST-junctional depression)), T-wave inversion (codes 5.1-2 (T wave inversion ≥1.0 mm)) or with an abnormal frontal T-axis (-180° to -15° and 105° to 180°) [13–17] were selected, after exclusion of the ECGs with non-interpretable ST segments during the exercise test by a clinical cardiologist [7]. These subjects are representative for a study population at intermediate coronary risk, due to the selection from a low risk population and in the presence of ≥1 high risk characteristic [13–18]. First, we investigated the prevalence of documented CAD. Second, we investigated the invasive therapeutic implications according to coronary calcium scores and exercise test results.
Methods
Subjects
Asymptomatic male and female subjects with ST-T changes on a 12-lead resting ECG were selected from the prospective population based Prevention of REnal and Vascular ENdstage Disease (PREVEND) cohort study in Groningen, the Netherlands. The primary aim of this cohort study is to assess the value of urinary albumin excretion in relation to cardiovascular and renal risk. In addition to the ECG, collected data include medical history, demographics, biometric data, urine- and blood collections and laboratory measurements. The first visit has taken place between 1997–1998. Subjects for the current study were selected after the second visit (2001–2003). Exclusion criteria were previous manifestations of coronary heart disease (myocardial infarction, revascularization procedure, or Q waves on the ECG) or coronary angiography (CAG); age >70 years; and subjects in whom the ST-T segment was not interpretable during the exercise test due to atrial fibrillation or left bundle branch block (LBBB) or ST depression >1 mm at 80 msec after the J point [7]. For details on the PREVEND study design we refer to earlier publications [19]. All participants underwent measurement of calcium scores by EBT and exercise testing. This PREVEND substudy was approved by the medical ethics committee and conducted in accordance with the guidelines of the declaration of Helsinki. All participants have given written informed consent.
Electrocardiography
Standard 12-lead ECGs were recorded with Cardio Perfect equipment (Cardio Control, Delft, The Netherlands), stored digitally, and classified according to the Minnesota code, using the computer program MEANS (Modular ECG Analysis System) [20]. Signal analysis and classification of MEANS have been extensively evaluated [21, 22]. ST-T segment changes were defined by Minnesota codes 4.1-2 (ST-junctional depression = 0.5 mm) and 5.1-2 (negative T-wave ≥1 mm) or abnormal mean frontal T-axis (-180° to -15° and 105° to 180°) [13–18]. T axes were computed from vectorcardiographic X, Y and Z leads, which can, in good approximation, be reconstructed from the standard ECG leads [23]. The mean spatial axis was obtained by vectorially adding the instantaneous heart vectors during the T wave. The mean frontal T axis is the angle between the X axis and the projection of the mean spatial T axis on the frontal XY plane. Q waves were defined by Minnesota codes 1.1–1.3 [17]. All ECGs were reviewed by a senior clinical cardiologist in order to exclude the ECGs of which the ST-T segment was not interpretable during the exercise test.
Measurement of coronary calcium scores
Coronary calcium was measured using electron beam tomography (EBT) (e-Speed, GE Medical Systems, South San Francisco, USA). According to subjects' weight and size the beam speed was set to 50 ms (for small or slender patients) or 100 ms (for larger patients). Prospective ECG triggering was used and set at 42% of the R-R interval. Scans were made without the use of a contrast agent with 130 kV and 895 mAs. A single collimation of 3.0 mm and an increment of 3.0 mm was applied. Total radiation exposure was <1 mSv for each patient. The coronary calcium score was obtained by multiplying each area of interest with a factor indicating peak density within the individual area, as was proposed by Agatston [24].
Exercise testing
As is common practice in the Netherlands, all exercise tests were performed on a bicycle. Exercise tests were performed in accordance with the guidelines for exercise testing [6, 7]. All exercise tests were independently reviewed by a cardiologist (RT) and a research physician (CG), who reached consensus in all cases. Exercise test end points were defined as follows: positive, in case of ECG evidence of myocardial ischemia (≥1.0 mm horizontal shift of the ST segment at 80 msec after the J point compared to the baseline ECG) and/or in case of 30 mmHg decrease in systolic blood pressure and/or ventricular arrhythmia and/or typical angina; intermediate, in case of <1.0 mm ST depression as compared to baseline and/or aspecific anginal complaints in the absence of ECG evidence of ischemia; negative, in the absence of any of the above mentioned criteria; and non-interpretable, if <85% of the age- and sex- predicted heart rate or a rate pressure product <18,000 was achieved. Intermediate and non-interpretable results are considered as "nondiagnostic test results".
Protocol
All patients underwent measurement of coronary calcium scores by EBT and exercise testing. Test performance was evaluated according to the decision protocol as given in figure 1. In case of calcium scores ≥10, or positive exercise test result, CAG or MPS was recommended to evaluate the presence of obstructive CAD (figure 1). In subjects with calcium scores <10 and a negative or nondiagnostic exercise test result, a test to document obstructive CAD was not recommended. In this population the presence of obstructive CAD is almost fully excluded due to the high negative predictive value of low calcium scores on CAD [9, 10, 25]. In subjects with calcium scores <10 and a positive exercise test and in subjects with calcium scores 10–99, the first choice recommended test was myocardial perfusion scintigraphy (MPS), followed by CAG in case of abnormal results. In subjects with calcium scores 100–399 and in subjects with calcium scores ≥400, the first choice recommended test was CAG.

Decision protocol*. *see text for explanation. Abbreviations: CAG, coronary angiography; MPS, myocardial perfusion scintigraphy.
Endpoints
The primary endpoint was defined as documented CAD, i.e. presence of obstructive significant CAD (≥50% luminal obstruction), based on CAG, or MPS, in case CAG was not available. Myocardial perfusion scintigraphy was performed as previously described [26]. All CAGs were re-analysed by a senior cardiologist (FZ), without knowledge of the clinical data. By qualitative analysis the coronary arteries were graded as follows: normal coronary arteries, defined as the absence of any coronary lesion; non-obstructive CAD, if maximal luminal obstructions were <50%; and obstructive CAD, if lesions obstructed the lumen ≥50% (i.e. documented CAD). The secondary endpoint was a class I or IIa indication for a revascularization procedure (percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery (CABG)) according to the ESC and ACC/AHA guidelines for PCI and CABG [27–29]. Decisions to perform a revascularization procedure were taken by the Thoraxcenter multidisciplinary heart team. In case of obstructive CAD (= 50% luminal stenosis), either MPS, or fractional flow reserve (FFR) measurement [30, 31] was performed to guide the decision for a revascularization procedure. An FFR <0.75 was an indication for a revascularization procedure. All subjects were followed for the occurrence of cardiac events, i.e. myocardial infarction or coronary death. Cardiac events were collected by review of the subject's medical record, questionnaire or telephone interview.
Statistical analysis
Continuous data are expressed as mean ± standard deviation. Hypertension was defined as a systolic blood pressure >140 mmHg and/or diastolic >90 mmHg or use of antihypertensive medication. Left ventricular hypertrophy (LVH) on the ECG was defined according to the Cornell voltage-duration product [19]. Framingham risk estimations were calculated according to Wilson et al [32]. Since HDL cholesterol was not measured during the second visit, HDL cholesterol data of the first visit were used for the Framingham risk estimations. Significance was reached when p < 0.05. To compare the diagnostic yield of calcium scores with exercise test results, receiver operating characteristic (ROC) curve analysis was performed. We compared the area under the curves of both tests for the primary and the secondary endpoints. For the ROC analysis, subjects with calcium scores <10 and a negative or nondiagnostic exercise test and in whom MPS or CAG was not performed, were assumed to have no endpoints. Calculations were performed using the statistical package SPSS version 12.0 (SPSS, Chicago, USA) and STATA 9.0 (College Station, Texas, USA).
Results
Baseline characteristics
In 6,804 (99%) of 6,894 subjects participating in PREVEND between 2001–2003, a 12-lead resting ECGs was recorded. Of 481 (7%) subjects with ST-T changes on the ECG, 291 subjects had any of the following characteristics, namely previous manifestation of coronary heart disease; age >70 years; atrial fibrillation; LBBB or ST depression >1.0 mm at 80 msec after the J point. Of 190 subjects invited, 153 responded (81%) and were included. Baseline characteristics of the participants are shown in table 1. Of the 11 subjects with ECG criteria for LVH, 5 had calcium scores of 0 and 6 between 16 and 1313. The 10-year estimated Framingham risk was <10% in 49%, 10–20% in 22% and >20% in 29% of subjects.
Test results
Eighty-six (58%) participants had low calcium scores (<10), 18 (12%) had calcium scores 10–99, 29 (19%) participants had calcium scores 100–399 and 16 (11%) participants had high calcium scores (= 400). Exercise test characteristics are shown in table 2. Significant ST depression occurred in 19% of subjects and angina was present in 2%. Eighty-nine (60%) participants had a negative exercise test result, while 27 (18%) had a nondiagnostic and 33 (22%) had a positive exercise test result.
Endpoints
Four patients refused to undergo CAG or MPS as recommended by the decision protocol, namely one patient with calcium scores <10 and a positive exercise test; one patient with calcium scores 10–99 and a positive exercise test; one patient with calcium scores 10–99 and a negative exercise test; and one patient with calcium scores ≥400 and positive exercise test result. Therefore, outcome was obtained in 149 participants (100%) during 14 ± 3 months of follow up. No cardiac events occurred during follow up. The primary endpoint (documented CAD) was present in 24 (16%) participants. In 16 (11%) participants, the secondary endpoint, a Class I or IIa indication for revascularization procedure, was present according to the ESC and ACC/AHA guidelines for PCI and CABG in asymptomatic patients [27–29].
The diagnostic yield of coronary calcium scores compared to the exercise test
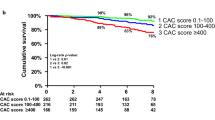
Results are shown in table 3 and figure 2. The primary and secondary endpoints were present in, respectively, 69% and 63% of 16 subjects with calcium scores = 400 and in, respectively, 39% and 27% of 33 subjects with a positive exercise test. In 37% of the 33 subjects with a positive exercise test, the absence of CAD was confirmed by a low calcium score and/or normal coronary arteries at CAG. A false negative test result was observed in 1% of 86 subjects with calcium scores <10 and in 7% of 89 subjects with a negative exercise test result. The subject with calcium scores <10, a positive exercise test and obstructive CAD was a non-diabetic, male 56-year old subject, a past smoker, who underwent a revascularization procedure for a left main stenosis. With regard to the primary endpoint, ROC statistics show an increased diagnostic yield of calcium scores above exercise testing: the area under the curve is 0.91 (95% CI 0.84–0.97) for calcium scores versus 0.74 (95% CI 0.64–0.83) for exercise testing (p = 0.004; figure 3). With regard to the secondary endpoint, ROC statistics show a similar pattern, albeit not statistically significant: the area under the curve is 0.90 (95% CI 0.78–1.00) for calcium scores versus 0.73 (95% CI 0.52–0.93) for exercise testing (p = 0.170; figure 3).

Endpoints according to coronary calcium scores and exercise test results. (a) primary endpoint (documented significant obstructive coronary artery disease) (b) secondary endpoint (Class I or IIa indication for revascularization procedure). Abbreviations: neg., negative; nond., nondiagnostic; pos., positive

Receiver operator characteristic curves. (a) primary endpoint (documented significant obstructive coronary artery disease) Area under the curve for coronary calcium scores 0.91 (95% CI 0.84–0.97); Area under the curve for exercise test 0.74 (95% CI 0.64–0.83). (b) secondary endpoint (Class I or IIa indication for revascularization procedure) Area under the curve for coronary calcium scores 0.90 (95% CI 0.78–1.00); Area under the curve for exercise test 0.73 (95% CI 0.52–0.93)
Discussion
Principal findings
Our results show that the diagnostic yield of measurement of coronary calcium scores for documented obstructive CAD is clearly superior to exercise testing in asymptomatic subjects at increased coronary risk. Furthermore, compared to exercise testing, high calcium scores identified a higher number of subjects with a class I or IIa indication for a revascularization procedure according to the ESC and ACC/AHA guidelines for PCI and CABG.
General comments
Non-invasive testing, such as measurement of coronary calcium scores and exercise testing, have become well established tests for risk stratification in selected asymptomatic subjects encountered in clinical practice. [1, 2, 6–8] Both tests provide fundamentally different diagnostic information. Coronary calcifications are highly specific for atherosclerosis and a strong correlation with total plaque burden has been demonstrated [33, 34]. Coronary calcifications parallel the development of atherosclerosis, with higher values present in men and in the elderly [35]. Higher amounts of coronary calcium have been associated with more severe CAD [33, 34, 36, 37]. Coronary calcifications have been associated with hard as well as with soft plaques [38]. In ultrasound studies the sensitivity for the detection of soft plaques is lower than for hard plaques [38]. However, since the absence of coronary calcium has been associated with a negative predictive value of >95% for future coronary events [39, 40], (soft) plaques maybe missed by EBCT have a limited clinical importance [5]. Absolute coronary calcium scores, as well as age- sex- specific percentiles, have been associated with the occurrence of future coronary events [35, 39–41]. Measurement of coronary calcium scores therefore focuses on the detection of CAD, while the exercise test focuses on the detection of myocardial ischemia. The "anatomic approach" has the advantage that certainty on the absence of clinically important CAD is obtained when calcium scores equals zero. This is of clinical importance since many subjects at intermediate risk (a probability of a coronary event between 1–2% per year due to the presence of at least one high risk characteristic or based on Framingham scores [4, 5]) do not have CAD [42–44].
In asymptomatic populations, guidelines traditionally focus on long-term risk assessment and prevention of future manifestations of coronary disease, while the role of invasive diagnostic and therapeutic procedures is hardly discussed [8, 45]. Although high risk criteria on stress testing in asymptomatic subjects are accepted as indications for CAG [12], direct referral to CAG based on high calcium scores is generally believed to be inappropriate [12, 46]. However, several arguments favor an invasive strategy in subjects with high calcium scores. A clear association has been demonstrated between calcium scores and the amount of myocardial ischemia [47–49] as well as the severity of CAD [33, 34, 36], which are the principle components of guideline recommendations for a revascularization procedure [27–29]. In addition, event free survival was decreased in asymptomatic subjects with high calcium scores and an abnormal myocardial perfusion test [49]. Clearly, all subjects with high calcium scores require aggressive secondary prevention, including treatment with cholesterol lowering, antihypertensive medications and aspirin. Our research protocol recommended performance of CAG in case of calcium scores = 400 or positive exercise test result. The decision to perform a revascularization procedure when a non-invasive stress test had not been performed prior to CAG, was guided by fractional flow reserve measurement during CAG [12, 30, 31]. Alternative diagnostic strategies may be the performance of CAG only after documentation of myocardial ischemia by non-invasive stress testing [46], or in combination with current generation CT-angiography. We agree that an invasive strategy is associated with a risk of complications and inappropriate revascularizations. The recent COURAGE trial has shown that some patients with stable CAD can be managed conservatively [50], and future guidelines may therefore be adapted. Our multidisciplinary study was based on the former ESC and ACC/AHA guidelines for PCI and CABG [27–29], and identified a substantial number of subjects with a class I or IIa indication for a revascularization procedure.
Twenty-nine subjects had a calcium score between 100–399. When compared to subjects with calcium scores = 400, less subjects had a primary endpoint (41% vs 68%) or an indication for a revascularization procedure (17% vs 63%). This finding is in line with previous findings on the increasing number of abnormal stress tests in case of higher calcium scores, namely in 18–60% of subjects with calcium scores = 400, compared to 7–23% of subjects with calcium cores of 100–399 [47–49]. Since the finding of myocardial ischemia in asymptomatic subjects with calcium scores >100 affects clinical outcome [49], non-invasive stress testing is warranted. This may be followed by an invasive strategy in case of abnormal test results, in addition to appropriate medical treatment. Further studies with larger numbers of patients are needed to evaluate these issues.
Remarks and limitations
Thirthy-two patients (21.5%) used betablockers or calcium antagonists at the time of exercise testing. These medications may affect the maximal exercise heart rate [51]. This may have contributed to a non-interpretable result found in one case (0.7%). With regard to the exercise test, information on the Duke score and ST-T hysteresis were not measured. Unfortunately, individual FFR values were not registered. We used EBT to measure calcium scores. Due to recent improvements in ECG gating software, shorter scan times and higher resolutions, current generation multi detector CT also provides accurate calcium scores measurements with a radiation dose of 1.0 mSv [52]. Since multidetector CT scanners are more widely available than EBT, our results, when extended to multidetector CT scanners, may therefore influence clinical practice. The sensitivity of the exercise test was somewhat lower than expected from large symptomatic populations undergoing exercise testing and coronary angiography [53]. However, the test characteristics of our study were very comparable to the studies including only asymptomatic subjects [7, 54–56]. The specificity for high calcium scores to detect significant CAD in our study population is similar to studies comparing calcium scoring and CAG in symptomatic patients [36, 37]. This observation implies that the association between calcium scores and severity of CAD at CAG may be extendable to asymptomatic populations. The current study population was derived from the PREVEND population of subjects without previous documented coronary heart disease, which can be regarded as a low risk population since 3.3% experienced a first coronary event during 5.5 years of follow up [57]. The presence of ST-T changes on the resting ECG is a clear additional high risk characteristic, and therefore our population can be classified as intermediate risk [13–18]. The prevalence of coronary calcium scores, in particular with regard to the 30–50% of subjects having calcium scores <10, was comparable to other asymptomatic populations with at least one risk factor [42, 43]. Our results are therefore applicable in asymptomatic populations, who are candidates for risk stratification, based on the presence of ≥1 high risk characteristic.
Conclusion
Measurement of coronary calcium scores is an appropriate initial non-invasive test in asymptomatic subjects at increased coronary risk. Furthermore, invasive diagnostic and therapeutic procedures are indicated in a high number of subjects with coronary calcium scores ≥400.
Abbreviations
- CAD:
-
coronary artery disease
- CABG:
-
coronary artery bypass graft surgery
- CAG:
-
coronary angiography
- CT:
-
computed tomography
- EBT:
-
electron beam tomography
- MPS:
-
myocardial perfusion imaging
- PCI:
-
percutaneous coronary intervention
- PREVEND:
-
Prevention of REnal and Vascular ENdstage Disease
- ROC:
-
receiver operating characteristics
References
Greenland P, Gaziano JM: Clinical practice. Selecting asymptomatic patients for coronary computed tomography or electrocardiographic exercise testing. N Engl J Med. 2003, 349: 465-473. 10.1056/NEJMcp023197.
Smith SC, Greenland P, Grundy SM: AHA Conference Proceedings. Prevention conference V: Beyond secondary prevention: Identifying the high-risk patient for primary prevention: executive summary. American Heart Association. Circulation. 2000, 101: 111-116.
Hendel RC, Patel MR, Kramer CM, Poon M, Hendel RC, Carr JC, Gerstad NA, Gillam LD, Hodgson JM, Kim RJ, Kramer CM, Lesser JR, Martin ET, Messer JV, Redberg RF, Rubin GD, Rumsfeld JS, Taylor AJ, Weigold WG, Woodard PK, Brindis RG, Hendel RC, Douglas PS, Peterson ED, Wolk MJ, Allen JM, Patel MR: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006, 48: 1475-1497. 10.1016/j.jacc.2006.07.003.
Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, Lauer MS, Post WS, Raggi P, Redberg RF, Rodgers GP, Shaw LJ, Taylor AJ, Weintraub WS: ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2007, 49: 378-402. 10.1016/j.jacc.2006.10.001.
Budoff MJ, Achenbach S, Blumenthal RS, Carr JJ, Goldin JG, Greenland P, Guerci AD, Lima JA, Rader DJ, Rubin GD, Shaw LJ, Wiegers SE: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation. 2006, 114: 1761-1791. 10.1161/CIRCULATIONAHA.106.178458.
Guidelines for cardiac exercise testing. ESC Working Group on Exercise Physiology, Physiopathology and Electrocardiography. Eur Heart J. 1993, 14: 969-988.
Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, Mark DB, McCallister BD, Mooss AN, O'Reilly MG, Winters WL, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Russell RO, Smith SC: ACC/AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation. 2002, 106: 1883-1892. 10.1161/01.CIR.0000034670.06526.15.
De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dallongeville J, Ebrahim S, Faergeman O, Graham I, Mancia G, Cats VM, Orth-Gomer K, Perk J, Pyorala K, Rodicio JL, Sans S, Sansoy V, Sechtem U, Silber S, Thomsen T, Wood D: European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts). Eur J Cardiovasc Prev Rehabil. 2003, 10: S1-S10. 10.1097/00149831-200308000-00004.
Raggi P, Callister TQ, Cooil B, He ZX, Lippolis NJ, Russo DJ, Zelinger A, Mahmarian JJ: Identification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomography. Circulation. 2000, 101: 850-855.
Kondos GT, Hoff JA, Sevrukov A, Daviglus ML, Garside DB, Devries SS, Chomka EV, Liu K: Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adults. Circulation. 2003, 107: 2571-2576. 10.1161/01.CIR.0000068341.61180.55.
Gordon DJ, Ekelund LG, Karon JM, Probstfield JL, Rubenstein C, Sheffield LT, Weissfeld L: Predictive value of the exercise tolerance test for mortality in North American men: the Lipid Research Clinics Mortality Follow-up Study. Circulation. 1986, 74: 252-261.
Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, Legako RD, Leon DF, Murray JA, Nissen SE, Pepine CJ, Watson RM, Ritchie JL, Gibbons RJ, Cheitlin MD, Gardner TJ, Garson A, Russell RO, Ryan TJ, Smith SC: ACC/AHA guidelines for coronary angiography: executive summary and recommendations. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Coronary Angiography) developed in collaboration with the Society for Cardiac Angiography and Interventions. Circulation. 1999, 99: 2345-2357.
Kardys I, Kors JA, van M, Hofman A, van der Kuip DA, Witteman JC: Spatial QRS-T angle predicts cardiac death in a general population. Eur Heart J. 2003, 24: 1357-1364. 10.1016/S0195-668X(03)00203-3.
Kors JA, de Bruyne MC, Hoes AW, van Herpen G, Hofman A, van Bemmel JH, Grobbee DE: T axis as an indicator of risk of cardiac events in elderly people. Lancet. 1998, 352: 601-605. 10.1016/S0140-6736(97)10190-8.
Diercks GF, Hillege HL, van Boven AJ, Kors JA, Crijns HJ, Grobbee DE, De Jong PE, Van Gilst WH: Microalbuminuria modifies the mortality risk associated with electrocardiographic ST-T segment changes. J Am Coll Cardiol. 2002, 40: 1401-10.1016/S0735-1097(02)02165-4.
Sutherland SE, Gazes PC, Keil JE, Gilbert GE, Knapp RG: Electrocardiographic abnormalities and 30-year mortality among white and black men of the Charleston Heart Study. Circulation. 1993, 88: 2685-2692.
Sigurdsson E, Sigfusson N, Sigvaldason H, Thorgeirsson G: Silent ST-T changes in an epidemiologic cohort study--a marker of hypertension or coronary heart disease, or both: the Reykjavik study. J Am Coll Cardiol. 1996, 27: 1140-1147. 10.1016/0735-1097(95)00614-1.
Ashley EA, Raxwal VK, Froelicher VF: The prevalence and prognostic significance of electrocardiographic abnormalities. Curr Probl Cardiol. 2000, 25: 1-72. 10.1016/S0146-2806(00)70020-X.
Smilde TD, Asselbergs FW, Hillege HL, Voors AA, Kors JA, Gansevoort RT, Van Gilst WH, De Jong PE, Van Veldhuisen DJ: Mild renal dysfunction is associated with electrocardiographic left ventricular hypertrophy. Am J Hypertens. 2005, 18: 342-347. 10.1016/j.amjhyper.2004.09.015.
Kors JA, van HG, Wu J, Zhang Z, Prineas RJ, van Bemmel JH: Validation of a new computer program for Minnesota coding. J Electrocardiol. 1996, 29 Suppl: 83-88. 10.1016/S0022-0736(96)80025-2.
Willems JL, Abreu-Lima C, Arnaud P, van Bemmel JH, Brohet C, Degani R, Denis B, Gehring J, Graham I, van Herpen G, .: The diagnostic performance of computer programs for the interpretation of electrocardiograms. N Engl J Med. 1991, 325: 1767-1773.
van Bemmel JH, Kors JA, van Herpen G: Methodology of the modular ECG analysis system MEANS. Methods Inf Med. 1990, 29: 346-353.
Kors JA, van Herpen G, Sittig AC, van Bemmel JH: Reconstruction of the Frank vectorcardiogram from standard electrocardiographic leads: diagnostic comparison of different methods. Eur Heart J. 1990, 11: 1083-1092.
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990, 15: 827-832.
Budoff MJ, Shokooh S, Shavelle RM, Kim HT, French WJ: Electron beam tomography and angiography: sex differences. Am Heart J. 2002, 143: 877-882. 10.1067/mhj.2002.121737.
Slart RH, Bax JJ, Sluiter WJ, Van Veldhuisen DJ, Jager PL: Added value of attenuation-corrected Tc-99m tetrofosmin SPECT for the detection of myocardial viability: comparison with FDG SPECT. J Nucl Cardiol. 2004, 11: 689-696. 10.1016/j.nuclcard.2004.06.131.
Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ, Hart JC, Herrmann HC, Hillis LD, Hutter AM, Lytle BW, Marlow RA, Nugent WC, Orszulak TA: ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation. 2004, 110: e340-e437. 10.1161/01.CIR.0000138790.14877.7D.
Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C, Jorgensen E, Marco J, Nordrehaug JE, Ruzyllo W, Urban P, Stone GW, Wijns W: Guidelines for percutaneous coronary interventions: the task force for percutaneous coronary interventions of the European society of cardiology. Eur Heart J. 2005, 26: 804-847. 10.1093/eurheartj/ehi564.
Smith SC, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, Kuntz RE, Popma JJ, Schaff HV, Williams DO, Gibbons RJ, Alpert JP, Eagle KA, Faxon DP, Fuster V, Gardner TJ, Gregoratos G, Russell RO, Smith SC: ACC/AHA guidelines of percutaneous coronary interventions (revision of the 1993 PTCA guidelines)--executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty). J Am Coll Cardiol. 2001, 37: 2215-2239. 10.1016/S0735-1097(01)01344-4.
Berger A, Botman KJ, MacCarthy PA, Wijns W, Bartunek J, Heyndrickx GR, Pijls NH, De Bruyne B: Long-term clinical outcome after fractional flow reserve-guided percutaneous coronary intervention in patients with multivessel disease. J Am Coll Cardiol. 2005, 46: 438-442. 10.1016/j.jacc.2005.04.041.
Bech GJ, De Bruyne B, Pijls NH, de Muinck ED, Hoorntje JC, Escaned J, Stella PR, Boersma E, Bartunek J, Koolen JJ, Wijns W: Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation. 2001, 103: 2928-2934.
Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB: Prediction of coronary heart disease using risk factor categories. Circulation. 1998, 97: 1837-1847.
Simons DB, Schwartz RS, Edwards WD, Sheedy PF, Breen JF, Rumberger JA: Noninvasive definition of anatomic coronary artery disease by ultrafast computed tomographic scanning: a quantitative pathologic comparison study. J Am Coll Cardiol. 1992, 20: 1118-1126.
Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS: Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation. 1995, 92: 2157-2162.
Wong ND, Budoff MJ, Pio J, Detrano RC: Coronary calcium and cardiovascular event risk: evaluation by age- and sex-specific quartiles. Am Heart J. 2002, 143: 456-459. 10.1067/mhj.2002.120409.
Budoff MJ, Diamond GA, Raggi P, Arad Y, Guerci AD, Callister TQ, Berman D: Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation. 2002, 105: 1791-1796. 10.1161/01.CIR.0000014483.43921.8C.
Nallamothu BK, Saint S, Bielak LF, Sonnad SS, Peyser PA, Rubenfire M, Fendrick AM: Electron-beam computed tomography in the diagnosis of coronary artery disease: a meta-analysis. Arch Intern Med. 2001, 161: 833-838. 10.1001/archinte.161.6.833.
Baumgart D, Schmermund A, Goerge G, Haude M, Ge J, Adamzik M, Sehnert C, Altmaier K, Groenemeyer D, Seibel R, Erbel R: Comparison of electron beam computed tomography with intracoronary ultrasound and coronary angiography for detection of coronary atherosclerosis. J Am Coll Cardiol. 1997, 30: 57-64. 10.1016/S0735-1097(97)00147-2.
Arad Y, Spadaro LA, Goodman K, Lledo-Perez A, Sherman S, Lerner G, Guerci AD: Predictive value of electron beam computed tomography of the coronary arteries. 19-month follow-up of 1173 asymptomatic subjects. Circulation. 1996, 93: 1951-1953.
Shaw LJ, Raggi P, Schisterman E, Berman DS, Callister TQ: Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology. 2003, 228: 826-833. 10.1148/radiol.2283021006.
Raggi P, Cooil B, Callister TQ: Use of electron beam tomography data to develop models for prediction of hard coronary events. Am Heart J. 2001, 141: 375-382. 10.1067/mhj.2001.113220.
Church TS, Levine BD, McGuire DK, Lamonte MJ, Fitzgerald SJ, Cheng YJ, Kimball TE, Blair SN, Gibbons LW, Nichaman MZ: Coronary artery calcium score, risk factors, and incident coronary heart disease events. Atherosclerosis. 2007, 190: 224-231. 10.1016/j.atherosclerosis.2006.02.005.
Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC: Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004, 291: 210-215. 10.1001/jama.291.2.210.
Taylor AJ, Bindeman J, Feuerstein I, Cao F, Brazaitis M, O'Malley PG: Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors: mean three-year outcomes in the Prospective Army Coronary Calcium (PACC) project. J Am Coll Cardiol. 2005, 46: 807-814. 10.1016/j.jacc.2005.05.049.
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002, 106: 3143-3421.
Hecht HS, Budoff MJ, Berman DS, Ehrlich J, Rumberger JA: Coronary artery calcium scanning: Clinical paradigms for cardiac risk assessment and treatment. Am Heart J. 2006, 151: 1139-1146. 10.1016/j.ahj.2005.07.018.
Berman DS, Wong ND, Gransar H, Miranda-Peats R, Dahlbeck J, Hayes SW, Friedman JD, Kang X, Polk D, Hachamovitch R, Shaw L, Rozanski A: Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography. J Am Coll Cardiol. 2004, 44: 923-930. 10.1016/j.jacc.2004.06.042.
He ZX, Hedrick TD, Pratt CM, Verani MS, Aquino V, Roberts R, Mahmarian JJ: Severity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemia. Circulation. 2000, 101: 244-251.
Anand DV, Lim E, Hopkins D, Corder R, Shaw LJ, Sharp P, Lipkin D, Lahiri A: Risk stratification in uncomplicated type 2 diabetes: prospective evaluation of the combined use of coronary artery calcium imaging and selective myocardial perfusion scintigraphy. Eur Heart J. 2006, 27: 713-721. 10.1093/eurheartj/ehi808.
Boden WE, O'Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, Chaitman BR, Shaw L, Gosselin G, Nawaz S, Title LM, Gau G, Blaustein AS, Booth DC, Bates ER, Spertus JA, Berman DS, Mancini GB, Weintraub WS: Optimal Medical Therapy with or without PCI for Stable Coronary Disease. N Engl J Med. 2007
Herbert WG, Dubach P, Lehmann KG, Froelicher VF: Effect of beta-blockade on the interpretation of the exercise ECG: ST level versus delta ST/HR index. Am Heart J. 1991, 122: 993-1000. 10.1016/0002-8703(91)90463-R.
Daniell AL, Wong ND, Friedman JD, Ben-Yosef N, Miranda-Peats R, Hayes SW, Kang X, Sciammarella MG, de YL, Germano G, Berman DS: Concordance of coronary artery calcium estimates between MDCT and electron beam tomography. AJR Am J Roentgenol. 2005, 185: 1542-1545. 10.2214/AJR.04.0333.
Ashley EA, Myers J, Froelicher V: Exercise testing in clinical medicine. Lancet. 2000, 356: 1592-1597. 10.1016/S0140-6736(00)03138-X.
Borer JS, Brensike JF, Redwood DR, Itscoitz SB, Passamani ER, Stone NJ, Richardson JM, Levy RI, Epstein SE: Limitations of the electrocardiographic response to exercise in predicting coronary-artery disease. N Engl J Med. 1975, 293: 367-371.
Uhl GS, Hopkirk AC, Hickman JR, Fisher J, Medina A: Predictive implications of clinical and exercise variables in detecting significant coronary artery disease in asymptomatic men. J Cardiac Rehab. 1984, 4: 245-252.
Barnard RJ, Gardner GW, Diaco NV, Kattus AA: Near-maximal ECG stress testing and coronary artery disease risk factor analysis in Los Angeles City fire fighters. J Occup Med. 1975, 17: 693-695.
Geluk CA, Tio RA, Tijssen JGP, van Dijk RB, Dijk WA, Hillege HL, De Jong PE, Van Gilst WH, Zijlstra F: Clinical characteristics, cardiac events and coronary angiographic findings in the prospective PREVEND cohort: an observational study. Netherlands Heart Journal. 2007, 15: 133-141.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/7/19/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
CAG, RD, JAK, RAT, RHJAS, HLH, RV, TPW, PEJ, WHG, MO, FZ were involved in the conception and design, the analysis and interpretation of the data; drafting of the manuscript and revising it critically for important intellectual content. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Geluk, C.A., Dikkers, R., Kors, J.A. et al. Measurement of coronary calcium scores or exercise testing as initial screening tool in asymptomatic subjects with ST-T changes on the resting ECG: an evaluation study. BMC Cardiovasc Disord 7, 19 (2007). https://doi.org/10.1186/1471-2261-7-19
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2261-7-19