
Abstract
Increasing recognition of interdependencies of the health of humans, other organisms and ecosystems, and of their importance to socio-ecological systems, necessitates application of integrative concepts such as One Health and EcoHealth. These concepts open new perspectives for research and practice but also generate confusion and divergent opinion, prompting new theories, and call for empirical clarification and evaluation. Through a semi-systematic evaluation of knowledge generation in scientific publications (comprised of literature reviews, conceptual models and analyses of communities of practice), we show how integrative concepts and approaches to health evolve and are adopted. Our findings indicate that while their contexts, goals and rationales vary, integrative concepts of health essentially arise from shared interests in living systems. Despite recent increased attention to ecological and societal aspects of health including broader sustainability issues, the focus remains anthropocentric and oriented towards biomedicine. Practices reflect and in turn transform these concepts, which together with practices also influence ways of integration. Overarching narratives vary between optimism and pessimism towards integrated health and knowledge. We conclude that there is an urgent need for better, coherent and more deeply integrative health concepts, approaches and practices to foster the well-being of humans, other animals and ecosystems. Consideration of these concepts and practices has methodological and political importance, as it will transform thinking and action on both society and nature and specifically can enrich science and practice, expanding their scope and linking them better. Transdisciplinary efforts are crucial to developing such concepts and practices to properly address the multiple facets of health and to achieve their appropriate integration for the socio-ecological systems at stake. We propose the term “transdisciplinary health” to denote the new approaches needed.
Similar content being viewed by others


1 Introduction
Integrative concepts of health arise to contend with linkages between the subjects, attributes, determinants and fields of health in humans and other species and their shared ecological systems. These concepts notably include: “One Health”, mentioned by Zinsstag et al. (2005, 2124) and strongly pursued since (Gibbs 2014; Zinsstag et al. 2015; Woods et al. 2018); “comparative medicine” (Lerner and Berg 2015, 1–3); “one medicine” (Jones 2019); “ecosystem health” (Schaeffer and Novak 1988); “EcoHealth”, pioneered by Wilcox (2004); and “global health” and “planetary health”, introduced by Cannon (2002, 480) and visibly articulated by Johnston et al. (2005). The concept of “Health in Socio-Ecological Systems” has also been proposed (Zinsstag et al. 2011, 148). While some concepts have a long history (for reviews see, for example, Battelli and Mantovani 2011; Lerner and Berg 2015), new frameworks encompassing human, animal and ecosystem health have been developed (e.g. Coker et al. 2011; Rock and Degeling 2016, 68) which transform the human-centred definition of health by WHO (2006, 1).
These integrative concepts of health are diverse and ambiguous—overlapping yet operationally detached (Lerner and Berg 2017, 5). The concepts are also in flux, reflecting ongoing changes in knowledge and practices. A lack of consensus around definitions and outright contradictions between them are to be expected, especially in new, broad and heterogeneous areas of research and practice. Yet consensus can be improved and contradictions resolved through better appreciation of both the uniting and distinguishing factors across the concepts. Seeking points of conceptual correspondence and interdisciplinary agreement can help to remedy the disadvantages of narrow views. Importantly, in many integrative concepts of health, the understandings and values of health are largely anthropocentric in orientation, even when measures and evaluations of health are extended to integrate other organisms (Lerner and Berg 2017, op.cit.). Such biases can have profound consequences on how responses to our dependency on other organisms and living systems are conceptualized and implemented. Negative environmental trends or collapses of ecosystems indicate that regarding nature as merely a provider for human needs is insufficient; humans impact other life, which in turn impacts humans (Kumar 2010; Pascual et al. 2017).
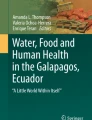
We posit that the links between the health of humans and that of other organisms and living systems, especially wildlife and ecosystems, are not yet widely appreciated and well researched. We further postulate that sustainable development is only possible if the dynamic processes affecting, and affected by, the health of ecosystems and of human societies are treated together more fully. In a globalizing world with extensive socio-ecological systems (Zinsstag et al. 2011, 152), with multiple drivers of the health of humans, animals and plants (Richardson et al. 2016; Haahtela et al. 2019, 3) and with interacting processes at many organizational levels (Fig. 1) and time scales, our era involves new threats and challenges yet also opportunities. In these systems and processes of health, socio-ecological structures must be recognized during both acute and foundational crises (Wallace et al. 2015, 70–11), but also in promoting sustainability in the longer term (Rock and Degeling 2016). There are thus important new challenges and opportunities for integrative concepts and practices of health.

Dimensions and types of integrative concepts of health. The typical central areas of a few common concepts have been indicated by hatched ovals. Note that: humans and animals overlap (denoted by dashed line), as do plants and animals with microbes which is not a taxonomic but a pragmatic concept (denoted by overlapping shapes), and that distinctions between synergism and antagonism are fuzzy as they coexist and coevolve and those between diversity and unity are value-laden
The evolution of integrative health concepts has been studied primarily with regard to One Health, as in the entire papers of Gibbs (2014), Degeling et al. (2017), Falzon et al. (2018) and Lerner and Berg (2017), and to environmental public health (e.g. Lovell et al. 2014; Chen et al. 2019). Evaluations of One Health as a field of activity have also been undertaken (Baum et al. 2016; Hitziger et al. 2018). However, extensive and systematic surveys of knowledge in the boundary field of human, non-human and ecosystem health have not been published except for some areas such as zoonoses (Anholt et al. 2012) and infectious disease control (Manlove et al. 2016). In their meta-analysis of sources on One Health, Manlove et al. (2016, 1) stressed that the benefits of the concept “remain unclear because its effects have not been quantitatively described”. Among extant descriptions, the environmental component in One Health has been found to be underrepresented (Barrett and Bouley 2015, 4). The societal dimensions in the relationships between humans and nature with regard to health have been gauged even more coarsely (Lapinski et al. 2015). Manlove et al. (2016, 5, 10) addressed this dimension mainly by specifying studies on management of health systems, whereas Falzon et al. (2018, 217) focused on economic studies. The frameworks used to assess the impact of One Health have focused on change and evaluation (Hitziger et al. 2018, 216), rather than networks, agency, paradigms and narratives. The criticisms by Hinchliffe (2015, 28, 34) which note a lack of consideration for contexts and processes in knowledge integration, and the proposals of Wallace et al. (2015) for structural One Health, have revealed the need for fuller analyses of—and comparisons between—the paradigms, modes of application and political economy of different integrative concepts of health.
The purpose of this paper is to analyse integrative concepts of health by systematically examining what has been integrated and how, and what are the implications for the co-generation and co-use of knowledge. For the purposes of our analysis, we defined integrative concepts of health as follows: concepts that address, or are applicable in a holistic manner to, the health of multiple living systems. These concepts include, but are not limited to, One Health, EcoHealth, ecosystem health and planetary health. Based on this, and on the above initial evaluations of gaps of knowledge, we address the following research questions: (1) How have these integrative concepts of health appeared in scientific literature, and what methodologies have been employed to study them; (2) How have such concepts been adopted and shaped in practice, and how has conceptual integration of health been perceived by communities practicing it; (3) What underlying narratives of health, knowledge and agency can be discerned in relevant literatures and practices; and (4) What is needed to further develop transdisciplinary co-creation of knowledge? We thus focus on knowledge production, but include initial analysis of its transfer, uptake and impacts, to be followed by in-depth studies of knowledge evaluation, application, implementation and co-creation.
2 Methods
2.1 General approach
We studied the evolution of integrative concepts of and practices on the health of humans, other animals, plants, microbiota and ecosystems, with particular reference to social ecology and the relationship between people, their shared environments, and mediating institutions and organizational systems. We therefore analysed semi-systematically, semi-quantitatively and comparatively the framing and use of such concepts within research and practice, with an emphasis on their ontology and meaning (Buttigieg et al. 2016), and on the extent of their transdisciplinarity, which is defined in multiple dimensions, involving science–society interactions (Stokols et al. 2013, 3–5; Allen-Scott et al. 2015, 867).
To characterize the development of concepts and their uses, we employed conceptual models, drew on the previous literature, and evaluated the development of knowledge empirically by coupled bibliometric and bibliographical analyses (task corresponding to research question 1; see Fig. 2 on the general layout of the methodological components in relation to all research questions). We further studied the framing of such concepts by professional networks—including those of authors within the literature (cf. Manlove et al. 2016, 3–4)—and by communities of practice (see Electronic Supplementary Material [ESM] Section 1, Wenger 1998) where knowledge is generated, shared, processed, translated, negotiated and used, and how these communities of practice have conceived the challenges and opportunities of integration (question 2). Based on these analyses, we explored the overarching narratives deployed by experts working with these concepts (on definitions see ESM and Degeling et al. 2017, 783) (question 3). These tasks jointly allowed us to identify further needs and opportunities for transdisciplinary co-creation and co-use of knowledge with integrative concepts of health (question 4).

Simplified diagram of the research and evaluation methodologies in relation to the research questions (Q1–4). The dotted arrows signify weaker or more sporadic involvement of the methodology in addressing the corresponding research questions. R&D research and development, WoS Web of Science database, CoP communities of practice
2.2 Data collection and analyses
The information search and evaluation procedures are described in detail in the electronic supplementary material (ESM—especially Fig. S1). We primarily performed searches in Web of Science (WoS) of papers published during its period of full coverage 1977-2016. Searches combined key descriptors for integrative concepts of health with (1) generic terms denoting Social Sciences and Humanities (SSH) studies (e.g. soci*, econ*, poli*, behave*, ethic*, phil*); and (2) specific SSH or interdisciplinary terms (e.g. sustainab*, altruis*, strateg*, actor*, “ecosystem service*, paradigm*). Search strategy decisions included: keywords or phrases (in English); data sources (primarily WoS, also for analytics); publication types (journal articles); time spans (1977–2016, 2014–2017, for historical searches longer); research orientations (categories of integrated concepts of health, SSH and other disciplinary fields); actors (authors, funders, organizers); scientific impacts (citations); and scopes of practice related to integrative concepts of health (e.g. clinical, policy-making, planning, advisory).
Excluding articles on global health (a field almost entirely concerned with human health) halved the number of articles retrieved (to 14,000, of which 6000 were in SSH); focusing among the 6000 on “One Health”, “EcoHealth” and “planetary health” gave ca. 1500 hits. Papers in all languages were included though English keywords or search phrases were used; English papers were dominant. We evaluated the relevance of sources using titles and abstracts, impacts (of citations and journals) supplemented by author, publication year, paper type and full-text availability. Based on this assessment, we derived a final subset from WoS of 697 recent SSH papers on integrative health concepts (see details in ESM, esp. Tables S2a–c).
We then analysed closely ca. 300 highly cited and otherwise seminal papers of the 697 papers. These papers were identified by the objective criterion of total number of citations (focusing on those cited > 3 times) and by our own judgments of their foundational and broad theoretical, methodological and applied importance from the point of view of social ecology (i.e. combining natural and social aspects), and from the point of view of transdisciplinarity (i.e. involving in addition to broad interdisciplinarity also science–practice interactions). It is acknowledged that such generic criteria of seminal impact are narrow and potentially biased, in part since publications with fewer citations (especially during early years of reception) may be influential, and vice versa: those often cited may not have lasting influence in science, let alone in policy and practice.
We then made “upstream” and “downstream” searches (of sources cited in and of sources citing the retrieved papers, respectively), to improve representativeness and to retrieve important complementary sources. We also retrieved sources by PubMed and Google Scholar searches (using the same search criteria as appropriate) and by non-systematic searches by the authors. These complementary searches included monographs, compilation publications, books (including textbooks), grey literature and databases, constituting important additional publication categories and routes through which to identify the relevant historical literature.
The analyses of communities of practice were based partly on the retrieved literature (including data on organizations and countries hosting and funding research as well as published evaluations that have been made of One Health, EcoHealth and other relevant communities) and partly on searches in information systems of key actors, specifically in the European Union’s (EU’s) CORDIS (Community Research & Development Information System) and EUR-LEX (EU Law) databases and, to a lesser degree, in documents of FAO and WHO (cf. ESM. Professional opinions and information about activities in communities of practice were elicited specifically in a series of 10 meetings on One Health, EcoHealth and other integrative aspects of health (see ESM Table S1, and Keune et al. 2017). We also used informal expert judgement by the authors in workshops and write shops and in the identification and collective evaluation of publications and of other information sources and activities.
The communities of practice were characterized by qualitative and semi-quantitative methods by: key areas of research and development (R&D) input (funding), conduct (projects and networks) and output (publications), and with respect to linkages to policy and practice. The scientific and professional narratives were characterized on the basis of emergent typologies in seminal publications, with particular reference to framings and beliefs regarding health and knowledge (ESM Table S2d).
3 Results
3.1 Development of integrative concepts of health and their application in research and practice
Integrative concepts of and approaches to health have become more common in scientific literature relative to the overall increase in publications, and also to literature on health or ecosystems in general (Fig. 3a1–2; Table 1; cf. ESM Tables S2a–d). The period of strongest increase in integrative health literature varies within and between topic areas. Environmental health was commonly addressed already in the 1970s and experienced its steepest increase around 1990, especially regarding SSH papers, which has then levelled out in comparison with some other topics such as global health. Studies on ecosystem health boomed in the late 1990s (Fig. 3, Table 1) and then levelled out, but still constitute a greater body of research than that on EcoHealth (Table 1). Studies on forest and plant health exhibit relatively stable trends (Table 1), but also their focus shifted to global change (e.g. Ramsfield et al. 2016). Studies on One Health underwent a rapid increase first in 1992–1996 with “one medicine” and again in 2012–2016 encompassing human–animal interactions; both phases included traditional and emerging diseases. However, there was a notable dominance of infectious diseases within One Health. Partly therefore, the steepest increase in all papers explicitly addressing the key integrative concepts of health (Columns 1–11 in Table 1) was during 1992–1996.

Trends in the position of integrative concepts of health in the scientific papers identified in the searches, as measured by four key criteria. Long-term trends are shown for all Web of Science papers (a1) and for social sciences/humanities (SSH) papers (a2) as proportions of total amounts of papers (log scale y e−4) for some categories but excluding the dominant human health focused “global health”. The data for “EcoHealth or Eco-health” as a more recent and uncommonly mentioned category have not been shown (cf. Table 1). More recent trends are shown for some categories and their combinations for highly cited papers (b1, as proportions of all papers) and in author affiliations for papers on “One Health”, “EcoHealth” or “planetary health” (b2, as proportions of all authors). H or H2 = health (depending on dataset or stage of bibliometrical analysis); Env = environmental; Ecos = ecosystem; US/CAN = USA and Canada; UK = United Kingdom; Etc Eur = Europe except UK; ANZ = Australia and New Zealand; Afr = Africa; ME = Middle East; S/M Am = South and Central America
Many retrieved papers were of low relevance, as the integrative concepts were used narrowly, typically in single focused human health or ecological research, or as buzzwords. Among highly cited papers (Fig. 3b1), the relative share of the papers in all 11 categories of integrative health concepts—ranging from 0.5–4% depending on the category (Table 1)—was higher than when comparing all papers in these categories (also the papers less cited) to the total number of papers (0.16% during 2012–2016, see column “Combined (1–11)”. This suggests the high impact and importance of broadly integrative studies as compared to more specific research. The relative shares of also the highly cited papers and their trends varied between areas, from high levels within human-focused (more narrowly framed) integrated health to lower levels within environmental health and One Health. All these categories indicated stable levels of relative impact (or researcher activity) over time, whereas the share of highly cited papers on ecosystem, forest and especially ocean health increased strongly from ca. 2010 (Fig. 3b1).
As to qualitative traits of research, anthropocentric, economic and pragmatic topics have dominated even in the expanded framing of health which has increasingly addressed global, environmental and societal aspects. The relative share of SSH papers was higher in topic areas such as global health, EcoHealth and holistic health. Regarding the methodological approaches used in literature, “integrative health” commonly encompassed both traditional and modern Western (mainly human) medicines. An English-centred perspective is present in published research notwithstanding inclusion of publications in other languages and from other regions and increasing research efforts and funding in non-English-speaking regions.
3.2 Communities of practice and their knowledge uptake and co-creation: from anthropocentric to socio-ecological
By evaluating the data on professional activities, we identified key strengths, gaps and trends in communities of practice including researchers, other experts and stakeholders. The content and scope of these professional activities directly reflect the uptake and use of integrated concepts and scientific and professional discourses (Table 2). The knowledge co-creation by the disciplinary communities and between researchers and practitioners was more difficult to establish and was traced more indirectly. The variations and trends within knowledge uptake and co-creation activities are for instance affected by the educational backgrounds, and affiliations of the practitioners (communities of human and veterinary medicine, plant health and ecology are thus identifiable, cf. ESM Fig. S4).
We found shifts in the levels of activities of research teams and networks in different geographical contexts, as investigated by author affiliations (Fig. 3b2; cf. ESM Fig. S2 and Table S3). USA and Canada have sustained high levels of activity. The relative level of research in the UK has declined, but in the rest of the EU it has increased to match that of North America. Research activity is increasing also in Australia, Africa and Asia, reflecting knowledge needs and efforts in these regions. The shifts were in part linked with diversified funding (ESM Fig. S2). Funding for studies involving integrative concepts, notably One Health, has increased especially in China, and practical applications are likely to follow. Their level of transdisciplinary knowledge co-creation is yet unclear.
Holistic initiatives and practices of health are dynamically developing, despite the inertia also observed. These have emerged along with interdisciplinary collaboration and new partnerships through shared challenges, some of which existed prior to the emergence of integrative concepts of health terms (e.g. King et al. 2004; Parkes et al. 2005). Examination of relevant EU Research and Innovation (R&I) projects (ESM Table S3) revealed that activities on One Health have increased more rapidly than those on ecosystem health when proceeding from the EU’s Framework Program 6–7 funding mechanism. Moreover, those on ecosystem health often addressed health as a topic peripheral to ecological studies, or defined ecosystem health unclearly. In both categories, we noted duplication of activities and deficits of broader approaches including social sciences. These suggest weak transdisciplinarity in R&I policy. Specifically, this involves a lack of studies of science–society interactions, e.g. instead including stakeholder communication and knowledge brokering in R&D projects only as an add-on and not as a topic of analysis in its own right.
Using the literature on integrative concepts of health (cf. Sect. 3.1) and the information on topics of activity, we synthesized their contents along the dimensions of “traditional” or “novel” scope and of their objects of concern (Fig. 4). The scope has broadened to include topics such as benefits along with risks, societal factors and interventions, nature-based health and planetary health. The concerns also increasingly include non-human organisms. In all these respects, there are overlaps between approaches to integration, and convergence and divergence between them. The consideration of interdependencies differs both between the communities of practice and between the respective areas of conceptual and functional integration. In terms of the systems addressed, the approach to health varies from close-range integration (microbiome–macrobiome interactions) over intermediate range (human–non-human interactions) to far range (ecosystem–society interactions). Furthermore, we found temporal developments in the consideration of interactions and interdependencies: while interest in integrative concepts and approaches has increased overall, in some cases it has subsided or lagged behind, such as in the socio-economic dimension (Table 2).

Development of important discernible fields of integrative concepts of health with regard to overall scope and goals, with examples in medical, veterinary and ecological research as identified through our review. The relationships and successions of fields (suggested by thick arrows) are indicative as they overlap, recur, converge and diverge. Note the emergence of nature-based interests, and potentially of holistic health
We further examined communities of practice based on their structure and organization, on topics of interest (Fig. 5a) and on activities according to the types of actors and the cycles in knowledge generation and intervention (Fig. 5b; ESM Table S4). We find important application areas of integrative concepts of health (see grey boxes). Many of these areas can be seen as “boundary objects” (on this concept in relation to ecosystems, see Abson et al. 2014) that promote the interaction and, potentially, integration between communities of practice that have been isolated in established disciplines and sectors. Influences of broader social networks (Manlove et al. 2016, 1) are identifiable, and also “Latourian” actor networks can be postulated, as with avian influenza (cf. Tirado et al. 2015, 116, 120). However, it is evident that the uptake and co-creation of holistic knowledge of health are hampered by many organizational and cultural factors.

Integrated approaches to health in key areas. The structure of key relations of communities of practice (CoP), defined by topics (a) and actors and activities (b). Important topical (a) and functional (b) areas of integration are highlighted in the rectangular boxes with rounded corners, and the overall significance of health (explained in boldface) is encapsulated in the part (b)
Among policy instruments and actors in the EU, the use of integrative concepts of health has increased and expanded from traditional environmental health studies and practices, but is still dominated by certain high-profile topics such as antibiotic resistance and food safety (ESM Table S4). A broader and more fundamental socio-ecological perspective seems to be less developed, as was found in knowledge co-creation and R&I policy (see the 3rd paragraph in this sub-section). This also mirrors the status of integrative concepts of health by global communities of practice, e.g. in FAO (One Health is usually placed under animal health activities), and WHO (“integrative medicine” is often linked with traditional and complementary medicine, i.e. integrative with regard to approach, not to organisms, see WHO 2013). Sustainability challenges have facilitated deeper integration of health that includes social dimensions, but this remains to be achieved for non-human and ecosystem health.
3.3 Discourses and narratives of integrative concepts of health: optimistic and pessimistic views
Various overarching narratives of health were discerned in scientific and professional discourse. The narratives are embedded in interpretations of scientific information and thus in cultural conceptions and traditions, both disciplinary and general, reflecting fundamental assumptions and valuations regarding health and health promotion (Table 3). We identify multiple roles for these narratives: (1) conveying ideas, or ideals, about the unity of health and of knowledge; (2) helping to formulate linkages between aspects of health and sectors or fields of activity (a direct role in R&I processes); (3) functioning in communication about health and in interaction between communities of practice; and (4) acting in scientific, professional and social learning. Some of these overlapping functions involve contested framings, value conflicts and even tactical uses of integrative concepts, e.g. to defend or expand positions of established fields (cf. Hinchliffe 2015, 29–30).
Notwithstanding the limits of broadly integrative narratives and corresponding actions, we note a broadening scope of and increasing impetus towards the unification of narratives within human, veterinary and ecosystem health (Figs. 4, 5). We also find shifts towards consideration for the values of nature in itself, i.e. de-centring humans in a more altruistic and communitarian meta-narrative. In veterinary medicine, the wildlife perspective is often still subsumed under domestic interests, but more ecological orientation is emerging. Environmental health has moved from anthropocentric risk to broader themes, notably nature’s benefits to health and ecosystem health (Table 2).
In some regards, the narratives that underpin integrative concepts of health retain traditional tropes and features, or have even evolved towards less holism, e.g. when an allegedly interdisciplinary community of practice is dominated by narrow technical concepts (cf. Sect. 3.2). Notably, we find that scientific and applied narratives often do not fully account for economic, political and structural aspects of integrative health and may become reactive instead of proactive. There are drivers or enablers as well as obstacles and limits for unified narratives (Table 3), additionally; therefore, such narratives vary. The outcomes depend on the area of research or practice and on the circumstances, e.g. balance between specificity and generality and between new and traditional knowledge.
We further distilled meta-narratives of health (including that of non-human entities) and of knowledge, reflecting varying expectations (Fig. 6). These narratives are strongly related to world views, notably regarding the value of integrative health and knowledge, and their underlying capacity to be integrated. Narratives range from the extremes of ideologically conditioned optimism to fearmongering, and from the exaggerated certainty of experts, for example as demonstrated by Tversky and Kahneman (1974), to “manufactured uncertainty” (cf. Michaels and Monforton 2005, 43–44). Defence narratives using metaphors of immunity or natural enemies are encountered with zoonosis outbreaks (e.g. Mutsaers 2015, highlights) and can be coupled with abatement strategies that omit socio-ecological root causes and interventions (Fig. 6 lower right). Counter-narratives emphasize the benign in nature, with either pessimism (Fig. 6 upper left) or optimism (Fig. 6 upper right) towards the limits of knowledge and then towards control of the processes involved. There are intermediate discourses between these types of narratives. Importantly, narratives of adaptive nature, health, care and governance emerge (Fig. 6 central area). For example, nature as a negative influence on health can also be coupled with positive views of resilience and of human control.

A typology of narratives of health and knowledge with regard to integration under complexity. The typology is based on expectations regarding the potential or factual improvements in health and the improvement in knowledge, indicating prevailing and alternate narratives discerned in the literature and expert opinion. Note intermediates and interactions between categories. R&D research and development
4 Discussion
4.1 The importance of integrated concepts of health as reflected in the development of the associated literatures
Integrative concepts of health are important for the development of science and for other forms of knowledge generation such as monitoring and surveillance. They elucidate the interdependencies between humans, other organisms and ecosystems; can provide shared methods of diagnosis, prognosis and therapy; and promote improved and more nuanced understanding of aspects of health. The very emergence of integrative concepts of health, varied as they are, underlines their importance in bridging gaps between fields of knowledge (scientific and applied, also and experiential) and practices. One of the key common attributes of such concepts is the perceived need for sustaining health through a more comprehensive understanding of the relative importance and impacts of interacting mechanisms and systems, including interventions (Zinsstag et al. 2011, 154–155; Boriani et al. 2017, 2). The scope of inquiry includes biological and social systems and potentially biogeochemical systems too, as organisms not only adapt to but also construct their environment (Lewontin 1992; cf. Fig. 1). However, we observed the rapid increases in research on integrative concepts of health (Fig. 3) to be accompanied by continued compartmentalization in silos, a central finding also by Manlove et al. (2016, 1). We also found uneven development in the various dimensions of integration, with particular gaps in integration across humans and other organisms; across biomedical and SSH studies, as did Friese and Nuyts (2017); across soft and hard methods; across different geographical regions; and across research and practice (Table 1). These variations reflect continued ambiguity in the meaning of the integrative concepts and highlight key development needs.
As our analysis suggests, integrative concepts of health can transform thought and practice on multiple levels and in many directions, thus enriching transdisciplinarity (Allen-Scott et al. 2015, 869; Schelling and Zinsstag 2015). This can in principle be developed to new overarching concepts such as holistic health accounting for interdependencies among beneficiaries or agents (Fig. 4), and within practice to more responsive relationships between knowledge, motivation and action. Accounting for linkages between nature and humans is crucial for improvements in health of all living systems, and vice versa: health provides a potent way to explicate and develop those linkages. Therefore, the potential importance of integrative concepts is great. However, improved understanding and promotion of such holistic knowledge generation and uptake on more pragmatic level, across spatial and time scales, will require further study, experimentation, evaluation and implementation. The demonstrated deficits in transdisciplinary health concepts and applications point to considerable challenges before their full potential can be realized.
4.2 Scientific and professional discourses on integrated health: diagnosis, aetiology and emerging cures for myopia
The low relevance of many scientific papers to progressing the development, application or both of integrated concepts of health was often due to limited consideration of biological or socio-ecological entities, mainly in the following respects: (1) studies with outcome measures limited to human health dominated; (2) within environmental health, studies commonly treat the environment as an external influence; (3) in studies of ecosystem health and One Health, natural scientific research dominated; (4) veterinary studies focused on the health or transmission role of domestic animals; (5) many sources allegedly on novel integrative aspects of health were in fact derivative. Among top-cited papers, health was addressed in a narrow manner; few of the papers on broadly integrative concepts of health including societal aspects were rarely among the most cited.
On the other hand, many sources that did not explicitly address integrative concepts of health were relevant for their development and application of interdisciplinary and transdisciplinary knowledge and practice. For instance, evolutionary studies can unite the health of various host and pathogen organisms (James et al. 2015b, 4083–4087). Such interactions between otherwise distinct areas of research may first be conceptual and weak but can develop to strong functional ties simultaneously transforming fields, as seen with “omics” (Marco-Ramell et al. 2016). Likewise, many areas in human health research have broader relevance, for instance through insights in the shared foundations of health such as the role of microbiome (Ruokolainen et al. 2017, 43; Haahtela et al. 2019, 4), in integrated surveillance (Whitmee et al. 2015, 2018), and in bioethics (Lee 2017, 5). New ways to account for linkages in health are also observable in the exposome concept (Wild 2012), and in allostasis, the process of achieving stability after load (Logan et al. 2018) or, equally, through beneficial stimuli (Lovell et al. 2014; James et al. 2015a).
Most integrative accounts of health were concerned with the dependence of humans on other organisms and ecosystems (e.g. Lovell et al. 2014, 13–14; Whitmee et al. 2015, 1987), but alternative ontologies are emerging which include reciprocal and multi-directional linkages, e.g. of humans as stressors and beneficiaries of ecosystems (Haahtela et al. 2019, 2) and as parts of ecological economy (Whitmee et al. 2015, 2011), of humans as guardians and stewards of socio-ecological systems or as sentinels of sustainability (Loring et al. 2016), of animal-assisted health interventions (Hediger et al. 2019), of a “meshwork” encompassing humans and others (Rock and Degeling 2016, 71), and of extended solidarity between these entities and agents (Rock and Degeling 2015). While there is a dominance of attention to infectious diseases from the point of view of humans and domestic animals (e.g. Jones et al. 2008, 990–992; Wiethoelter et al. 2015), due largely to pandemic threats (Desjardins et al. 2018), there is considerable scope for this area to address the health of ecosystems and socio-ecological systems as a whole. More balanced consideration of ‘good’, ‘bad’ and intermediate nature (Antoine-Moussiaux et al. 2019, 3–5) and of risks and rewards are steps in this direction.
The discourse on ecosystem health has been transformed by broad themes of sustainability and resilience (McAlpine et al. 2015, 56–57) and interspecies justice (Lysaght et al. 2017, 5–9). As lay perspectives on zoonotic risks become more prominent, new types of less anthropocentric narratives also emerge (Rabinowitz et al. 2008). This development parallels that in public health where links with sustainable development, salutogenic notions of health, planetary health and human agency are increasingly emphasized (Tilman and Clark 2014, 518; Kurth 2017). Past narratives also recur: the “Earth ethics” underlying much of the interest in such concepts in part involves a re-emergence of “land ethics” (Callicott 2013), and the idea of eradication of health risks resurfaces in epidemics which promoted One Health. A narrative focused on threats, e.g. from vector-borne diseases and zoonoses (Wald 2008; Karesh et al. 2012, 1941–1943), remains strong. This is problematic as the important risks and costs of non-communicable diseases and long-term factors of health can be easily overlooked. Interestingly, global organizations such as FAO, WHO and OiE adopted a One Health concept, despite its vagueness, in response to the avian flu in part to reduce conflicts and defend their legitimacy (Chien 2012, 222–224). It is important to scrutinize such motives behind narratives and their implications for policies and practices. For instance, rallying for One Health without consideration of political realities in its integration with trade and development misses key social and political contexts, which is both naïve and misguided (Mwakalimba and Green 2015).
4.3 Challenges to integration from complexity and specialization, and potential responses
The clarification, further development and better application of integrated concepts of health require sensitivity to the dimensions of integration (Fig. 1), to its contexts (Assmuth and Hildén 2008) and to the resultant complexity (Keune 2008; Keune and Assmuth 2018). The interrelationships of environmental and social aspects of health need to be specifically appreciated (Barrett and Bouley 2015; Zinsstag 2012), extending beyond narrow biomedical paradigms to more general views of knowledge. This will be particularly important when applications and impacts are considered, e.g. through medical or environmental practice and through science and innovation policy (Sect. 3.2, Fig. 4). While ways to incorporate the societal dimension in One Health have been outlined (Lapinski et al. 2015), these are dominated by positivist paradigms (Phoenix et al. 2013, 219–223). These methodological obstacles are compounded by the confirmed dominance of anthropocentric studies and practices (Figs. 5, 6). Similarly, Europe-centric and English language dominance could shape the concepts and approaches used, the narratives upheld, and the policies and practices adopted on integrated health. A more global—and more culturally inclusive—outlook is needed and offers great potential for concepts and practices of health.
The content and scope of integrated concepts of health are in flux, as illustrated by the literature evaluated in our study (Table 1, Figs. 3 and 4). Concepts of ecosystem health range from metaphors to operational models which can accommodate ex ante and ex post assessment along with participatory governance (Fock and Kraus 2016, 7–8), and those of ecosystem services can (despite a utilitarian lens) renew thinking around the relationship between human health and the intrinsic value of nature (Ford et al. 2015). Definitions of the integrative concepts of health also vary in scope, and this instability is reflected in their content and underlying values (Lerner and Berg 2017, 5). The shift towards unification can also represent a renewal of the fundamental relationship between science and culture, as found in sustainability science (Lang et al. 2012) also in relation to health (White and Brown 2010), and it can reinforce the return of eco-centric concerns to the forefront of the discipline of bioethics (Lee 2017, 5, 9).
The complexity inherent in broadening the scope of health presents multiple and considerable challenges across scientific disciplines and communities of practice. These challenges are conceptual as well as organizational, cultural, pragmatic and even political. Yet this complexity needs to be tackled in order to address present and future problems and to give a “voice” to those impacted, including non-human organisms in a socio-ecological entity. It is precisely because of these that a transdisciplinary, collaborative and participatory approach sensitive to the perspectives and values of the actors is worth exploration and experimentation (Schelling and Zinsstag 2015). Reconfigurations of integrative concepts of health are thus called for. Such reconfigurations should be developed and applied through additional studies and collaborative action, in order to allow efficient evaluation of concepts such as One Health (Rüegg et al. 2017, 4) and to achieve (tentative) “proof” of concepts (Rabinowitz et al. 2013).
Specialization poses a second key challenge to integration and holism. Persistent “silos” were noted between communities of practice, as found by Manlove et al. (2016, 3–7) between ecological, veterinary and “third” (mainly human medical) communities. Silos are due especially to path dependencies in conduct and funding of practices and to the multiplicity of goals and processes embedded within related institutions. This involves continued dominance of communities of practice whose disciplinary background is located within human and domestic animal health, i.e. anthropocentric, and through which often also narrow technical paradigms and understandings are sustained and defended. External factors such as disasters or greater awareness of ecological crises and interdependencies may be needed to change these paradigms.
4.4 Social and political dimensions of integrative health in the context of sustainability
The impoverishment of the living environment, increasingly through anthropogenic factors, undermines both human health and ecosystem resilience, as found with abrupt climate change (McMichael 2017). The health of other animals and plants also depends on ecosystem quality. Integrative concepts and practices of health emerge to respond to this multifaceted challenge. Yet, the dependency of human, animal and plant well-being on ecosystems is widely ignored in political and economic spheres. The impoverishment of health through repression and other political and societal factors is additionally too often ignored. The complexity, uncertainty, ambiguity and dynamics of actor involvement in tackling these multiple dimensions of health (Table 3) pose “wicked problems” that have increasingly been addressed in policy studies, based on the work of Rittel and Webber (1973), also with regard to health (Walls 2018). New concepts, approaches, narratives and activities are needed also for maintaining the health of multiple systems as adaptive capacity emerging from and sustaining ecological and social functions (Charron 2012). The observed developments in communities of practice adopting integrative concepts of health (Fig. 6) reflect these pressing needs.
Even the increased use of concepts such as One Health may have limited penetration due to weak or unclear political commitments (Chatham House 2017). Problems also include the conception—notably in the human health sector—that One Health is a veterinary initiative of lower priority to the health of humans (Stärk et al. 2015, 124). Therefore, as well as deciding what kind of integrative health knowledge is needed and how to co-create it, communities of practice must also convince policy and decision makers, funders and others of its relevance and guide its use, demonstrating how it can be more valuable than narrow views and practices. This co-creation of actionable holistic knowledge has been studied, e.g. in synergistic Ebola biobanking (Capps and Lederman 2015, 1024–1027), and has been outlined in surveillance in terms of economic assessment (Babo Martins et al. 2016; 386), but less often used regarding the underlying societal goals and processes. For instance, the “proof of concept” of One Health surveillance by Kelly et al. (2017, 114–115) focused on technical and organizational aspects. The recent work on outbreak response sensitive to public preferences by Johnson et al. (2019, 164) is an important step, demonstrating there is no single generalizable best way to implement One Health (or other integrative concepts of health) and emphasizing the need for adaptive governance depending on the case and on collective priorities.
Better accounts of the social and political dimensions in integrative concepts of health, including value judgments, will thus be crucial to further development (Degeling et al. 2015, 2016; Johnson et al. 2019). The definition of human health (WHO 2006) (1) already accounts for societal factors, e.g. the distribution of burdens and benefits and the links between health and economic development (Beaglehole et al. 2011, 449; Lange and Vollmer 2017, 53–57). These accounts are natural also within extensions of health, e.g. nutrition (Cannon 2002). The challenge is to extend such societal considerations to the health of other organisms and living systems and to the corresponding fields of practice. The notion of health as dynamic adaptation rather than a state, stressed in salutogenetic models of health promotion (Antonovsky 1996; see also Huber et al. 2011), is applicable to other systems and can potentially enrich integrative concepts and practices of health, but will require consideration of political agency.
Integrative concepts and practices of health provide additional depth to notions and policies of sustainability, by combining ecological and social meanings and values, and thus promoting sustainable communities (Ostrom 2009). The conclusion holds regardless of anthropocentrism: humans will be concerned with non-human organisms and ecosystems when they sufficiently understand the interdependencies of their health and that of other biological entities, and, as biophilic creatures, value them (Wilson 1984). From such understanding and ethical valuation, balanced policies and actions can develop, as proposed, for instance for Ebola vaccination (Capps and Lederman 2015, 1014–1016, 1028).
5 Summary and conclusions
We summarize our key findings and discussion points with regard to the research questions posed at the outset:
- 1.
Integrative concepts of health have emerged in the scientific literature in various forms and during different periods, ranging from narrow to broad perspectives and from traditional to novel research. The concepts have expanded to address broader questions and ontological entities, some of them approaching genuinely holistic views of health in social ecology, but are yet dominated by narrowly anthropocentric and biomedical concerns, and by research paradigms that are predicated on positivist views.
- 2.
Communities and conducts of practice have evolved in response to these expanding and transforming scientific interests, to practical concerns and to societal structures and cultures which surround science and practice. Communities of practice have in turn influenced research, in interactive relationships of knowledge co-creation. Specifically, communities in One Health and EcoHealth have grown in response to the connectedness of health, ecological and social problems and have converged although there still is considerable separation and rigidity.
- 3.
Corresponding to the various integrative concepts of health among researchers and practitioners, different narratives and mixtures of narratives of health and of knowledge can be discerned, ranging from optimistic to pessimistic and from definite to inclusive notions. The narratives underlying integrative concepts and practices of health are linked to motivations and goals of research and applications as well as to world views, and thus to concrete political contents and contexts in these integrative fields of thought and activity.
- 4.
By open and innovative participatory transdisciplinary processes, fruitful and even surprising new ways can be found to navigate the dilemmas and tensions between increased breadth and complexity and between different views and values, as shown by developments in science and practice. Agreement can focus on achieving integration, instead of prescribing a certain kind and degree of integration, thus more fully realizing the potential of integrative concepts. This potential in responding to challenges in human and ecosystem health is great, especially when the multidimensionality and context dependency of the challenges and solutions are better appreciated.
We conclude that there are movements towards broader integration of different disciplinary conceptualizations of health, but the associated complexity—biological, geophysical and social—remains a challenge. Progress seems possible, especially by: more fully considering the contingencies and dynamics in the health of living systems; better utilizing the understanding of societal factors in these systems as a means to focus action; using the concept of health as a deliberative device to clarify its meanings within and across disciplines; identifying related values, goals and means. To reach the potential of integrative concepts of health, we thus generally advocate investing in a transdisciplinary approach that connects disciplines and communities engaged in co-production, co-interpretation and co-utilization of knowledge. Continuous reflection on the interplay between the concept of health, with its applications, will help resolve what might be meaningful and useful modes of integration of related concepts and practices. The means of engagement for the actors and communities involved, the appropriate scales, and the acceptable approaches should be subject to further studies. We tentatively propose the term “transdisciplinary health” to signify both the needed broad integration across fields and the dynamic interaction across research, practice and society as a whole, on all scales from local to global.
References
Abson DJ, von Wehrden H, Baumgärtner S, Fischer J, Hanspach J, Härdtle W, Heinrichs H, Klein AM, Lang DJ, Martens P, Walmsley D (2014) Ecosystem services as a boundary object for sustainability. Ecol Econ 103:29–37
Allen-Scott LK, Buntain B, Hatfield JM, Meisser A, Thomas CJ (2015) Academic institutions and one health: building capacity for transdisciplinary research approaches to address complex health issues at the animal-human-ecosystem Interface. Acad Med 90(7):866–871
Anholt RM, Stephen C, Copes R (2012) Strategies for collaboration in the interdisciplinary field of emerging zoonotic diseases. Zoonoses Public Health 59(4):229–240
Antoine-Moussiaux N, Janssens de Bisthoven L, Leyens S, Assmuth T, Keune H, Zinsstag J, Hugé J, Vanhove MPM (2019) The good, the bad and the ugly: framing debates on Nature in a One Health community. Sustain Sci 14:1729–1738
Antonovsky A (1996) The salutogenic model as a theory to guide health promotion. Health Promot Int 11:11–18
Assmuth T, Hildén M (2008) The significance of information frameworks in integrated risk assessment and management. Environ Sci Pol 11:71–86
Assmuth T, Lyytimäki L (2015) Co-constructing inclusive knowledge in converging fields: environmental and health care. Environ Sci Pol 51:338–351
Babo Martins S, Rushton J, Stärk KD (2016) Economic assessment of zoonoses surveillance in a ‘One Health’ context: a conceptual framework. Zoonoses Public Health 63:386–395
Barrett MA, Bouley TA (2015) Need for enhanced environmental representation in the implementation of One Health. EcoHealth 12(2):212–219. https://doi.org/10.1007/s10393-014-0964-5
Battelli G, Mantovani A (2011) The veterinary profession and one medicine: some considerations, with particular reference to Italy. Vet Ital 47:389–395
Baum SE, Machalaba C, Daszak P, Salerno RH, Karesh WB (2016) Evaluating one health: are we demonstrating effectiveness? One Health 3:5–10. https://doi.org/10.1016/j.onehlt.2016.10.004
Beaglehole R, Bonita R, Alleyne G, Horton R, Li L, Lincoln P, Mbanya JC, McKee M, Moodie R, Nishtar S, Piot P, Reddy KS, Stuckler D, Lancet NCD Action Group (2011) UN high-level meeting on non-communicable diseases: addressing four questions. Lancet 378:449–455
Boriani E, Esposito R, Frazzoli C, Fantke P, Hald T, Rüegg SR (2017) Framework to define structure and boundaries of complex health intervention systems: the ALERT project. Frontiers Public Health. https://doi.org/10.3389/fpubh.2017.00182
Bowen KJ, Ebi KL (2015) Governing the health risks of climate change: towards multi-sector responses. Curr Opin Environ Sustain 12:80–85
Buttigieg PL, Morrison N, Smith B, Mungall CJ, Lewis SE and the ENVO Consortium (2016) The environment ontology in 2016: bridging domains with increased scope, semantic density, and interoperation. J Biomed Semant 7:art. 57
Callicott JB (2013) Thinking like a planet: land ethic and earth ethic. Oxford Univeristy Press, Oxford
Cannon G (2002) Nutrition: the new world map. Asia Pac J Clin Nutr 11(Suppl 3):S480–S497
Capps B, Lederman Z (2015) One Health and paradigms of public biobanking. J Med Ethics 41:258–262
Charron DFE (2012) Ecohealth research in practice. Innovative applications of an ecosystem approach to health. Springer, New York. ISBN 978-1-4614-0517-7
Chatham House (2017) Monitoring progress toward implementation of a one health approach. Centre on Global Health Security Draft Meeting Summary, 16 Nov 2017. Chatham House—The Royal Institute of Global Studies, London
Chen X, de Vries S, Assmuth T, Dick J, Hermans T, Hertel O, Jensen A, Jones L, Kabisch S, Lanki T, Lehmann I, Maskell L, Norton L, Reis S (2019) Research challenges for cultural ecosystem services and public health in (peri-)urban environments. Sci Total Environ 651:2118–2129. https://doi.org/10.1016/j.scitotenv.2018.09.030
Chien Y-J (2012) How did international agencies perceive the avian influenza problem? The adoption and manufacture of the ‘One World, One Health’ framework. Sociol Health Illness 35:213–226
Coker R, Rushton J, Mounier-Jack S, Karimuribo E, Lutumba P, Kambarage D, Pfeiffer DU, Stärk K, Rweyemamu M (2011) Towards a conceptual framework to support one-health research for policy on emerging zoonoses. Lancet Infect Dis 11:326–333
Dahlgren G, Whitehead M (2007) European strategies for tackling social inequities in health: levelling up part 2. WHO Europe, Geneva. Originally printed 2006. Studies of social determinants of population health, 3. WHOLIS E89384
Degeling C, Johnson J, Kerridge I, Wilson A, Ward M, Stewart C, Gilbert G (2015) Implementing a One Health approach to emerging infectious disease: reflections on the socio-political, ethical and legal dimensions. BMC Public Health 15:art 1307
Degeling C, Lederman Z, Rock M (2016) Culling and the common good: re-evaluating harms and benefits under the One Health paradigm. Public Health Ethics 9:244–254
Degeling C, Johnson J, Ward M, Wilson A, Gilbert G (2017) A Delphi survey and analysis of expert perspectives on One Health in Australia. EcoHealth 14:783–792
Desjardins MR, Whiteman A, Casas I, Delmelle E (2018) Space-time clusters and co-occurrence of chikungunya and dengue fever in Colombia from 2015 to 2016. Acta Trop 185:77–85
Dora C, Pfeiffer M, Racioppi F (2013) Lessons from environment and health for HiAP. In: Leppo K et al (eds) Health in all policies. Seizing opportunities, implementing policies. Ministry of Social Affairs and Health of Finland, Helsinki, pp 255–285
Falzon L, Lechner I, Chantziaras I, Collineau L, Courcoul A, Filippitzi M, Laukkanen-Ninios R, Peroz C, Pinto Ferreira J, Postma M, Prestmo PG, Phythian CJ, Sarno E, Vanantwerpen G, Vergne T, Grindlay DJC, Brennan ML (2018) The quantitative outcomes of a “One Health” approach to study global health issues: a systematic review. Eco Health 15:209–227. https://doi.org/10.1007/s10393-017-1310-5
Fletcher J, Franz D, Leclerc JD (2009) Healthy plants—necessary for a balanced ‘One Health’ concept. Vet Ital 45:79–95
Fock HO, Kraus G (2016). From metaphors to formalism: a heuristic approach to holistic assessments of ecosystem health. PLOS ONE 11:art e0159481
Ford AES, Graham H, White PCL (2015) Integrating human and ecosystem health through ecosystem services frameworks. EcoHealth 12:660–671
Friese C, Nuyts N (2017) Posthumanist critique and human health: how nonhumans (could) figure in public health research. Crit Public Health 27(3):303–313
Gibbs EP (2014) The evolution of One Health: a decade of progress and challenges for the future. Vet Rec 174(4):85–91
Haahtela T, Holgate S, Pawankar R, Akdis CA, Benjaponpitak S, Caraballo L, Demain J, Portnoy J, von Hertzen L, WAO Special Committee on Climate Change and Biodiversity (2013) The biodiversity hypothesis and allergic disease: world allergy organization position statement. World Allergy Organ J 6(1):3
Haahtela T, von Hertzen L, Anto JM, Bai C, Baigenzhin A, Bateman ED, Behera D, Bennoor K, Camargos P, Chavannes N, Correia de Sousa J, Cruz A, Do Céu Teixeira M, Erhola M, Furman E, Gemicioğlu B, Gonzalez Diaz S, Hellings PW, Jousilahti P, Khaltaev N, Kolek V, Kuna P, La Grutta S, Thi Tuyet Lan L, Maglakelidze T, Masjedi MR, Mihaltan F, Mohammad Y, Nunes E, Nyberg A, Quel J, Rosado-Pinto J, Sagara H, Samolinski B, Schraufnagel D, Sooronbaev T, Tag Eldin M, To T, Valiulis A, Varghese C, Vasankari T, Viegi G, Winders T, Yañez A, Yorgancioğlu A, Yusuf O, Bousquet J, Billo NE (2019) Helsinki by nature: the nature step to respiratory health. Clin Transl Allergy 9(57):1–12. https://doi.org/10.1186/s13601-019-0295-2
Haines A (2016) Addressing challenges to human health in the Anthropocene epoch—an overview of the findings of the rockefeller/lancet commission on planetary health. Public Health Rev 37(14):1–5. https://doi.org/10.1186/s40985-016-0029-0
Halpern BS, Longo C, Hardy D, McLeod KL, Samhouri JF et al (2012) An index to assess the health and benefits of the global ocean. Nature 488:615–622
Hediger K, Meisser A, Zinsstag J (2019) A one health research framework for animal-assisted interventions. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph16040640
Hinchliffe S (2015) More than one world, more than one health: re-configuring interspecies health. Soc Sci Med 129:28–35
Hitziger M, Esposito R, Canali M, Aragrande M, Häsler B, Rüegg SR (2018) Knowledge integration in One Health policy formulation, implementation and evaluation. Bull WHO 98:211–218
Huber M, Knottnerus JA, Green L, van der Horst H, Jadad AR, Kromhout D, Leonard B, Lorig K, Loureiro MI, van der Meer JWM, Schnabel P, Smith R, van Weel C, Smid H (2011) How should we define health? Br Med J 343:d4163
James P, Banay RF, Hart JE, Laden F (2015a) A review of the health benefits of greenness. Curr Epidemiol Rep 2:131–142
James TY, Toledo LF, Rödder D, Leite da Silva D, Belasen AM, Betancourt-Román CM, Jenkinson TS, Soto-Azat C, Lambertini C, Longo AV, Ruggeri J, Collins JP, Burrowes PA, Lips KR, Zamudio KR, Longcore JE (2015b) Disentangling host, pathogen, and environmental determinants of a recently emerged wildlife disease: lessons from the first 15 years of amphibian chytridiomycis research. Ecol Evol 5:4079–4097
Johnson J, Howard K, Wilson A, Ward M, Gilbert GL, Degeling C (2019) Public preferences for One Health approaches to emerging infectious diseases: a discrete choice experiment. Soc Sci Med 228:164–171. https://doi.org/10.1016/j.socscimed.2019.03.013
Johnston N, Rogers M, Cross N, Schona A (2005) Global and planetary health: teaching as if future matters. Nurs Educ Perspect 26(3):152–156
Jones BV (2019) The origins of one medicine. Vet Rec 184(15):481. https://doi.org/10.1136/vr.l1723
Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL et al (2008) Global trends in emerging infectious diseases. Nature 451:990–994. https://doi.org/10.1038/nature06536
Karesh WB, Andy Dobson A, Lloyd-Smith JO, Lubroth J, Dixon MA, Bennett M, Aldrich S, Harrington T, Formenty P, Loh EH, Machalaba CC, Thomas MJ, Heymann DL (2012) Ecology of zoonoses: natural and unnatural histories. Lancet 380:1936–1945
Kau AL, Ahern PP, Griffin NW, Goodman AL, Gordon JI (2011) Human nutrition, the gut microbiome and the immune system. Nature 474:327–336
Keesing F, Belden LK, Daszak P, Dobson A, Harvell CD, Holt RD, Hudson P, Jolles A, Jones KE, Mitchell CE, Muers SS, Bogich T, Ostfeld RS (2010) Impacts of biodiversity on the emergence and transmission of infectious diseases. Nature 468:647–652
Kelly TR, Karesh WB, Johnson CK, Gilardi KV, Anthony SJ, Goldstein T, Olson SH, Machalaba C, PREDICT Consortium, Mazet JA (2017) One Health proof of concept: bringing a transdisciplinary approach to surveillance for zoonotic viruses at the human-wild animal interface. Prev Vet Med 137:112–118
Keune H (2008) Critical complexity in environmental health practice: simplify and complexify. Environ Health 11:S19
Keune H, Assmuth T (2018) Framing complexity in human health and the environment. Oxford research encyclopedia of environmental science (July 2018). Oxford University Press, Oxford. https://doi.org/10.1093/acrefore/9780199389414.013.350
Keune H, Flandroy L, Thys S, De Regge N, Mori M, Antoine-Moussiaux N, Vanhove MPM, Rebolledo J, Van Gucht S, Deblauwe I, Hiemstra W, Häsler B, Binot A, Savic S, Rüegg SR, De Vries S, Garnier J, van den Berg T (2017) The need for European OneHealth/EcoHealth networks. Arch Public Health 75:64. https://doi.org/10.1186/s13690-017-0232-6
King LJ, Marano N, Hughes JM (2004) New partnerships between animal health services and public health agencies. Rev Sci Tech (Int Office Epizootics) 23(2):717–725
Kumar P (ed) (2010) The economics of ecosystems and biodiversity—ecological and economic foundations. The Economics of Ecosystems & Biodiversity (TEEB) Study Report. Earthscan, Washington
Kurth AE (2017) Planetary health and the role of nursing: a call to action. J Nurs Scholarsh 49(6):598–605. https://doi.org/10.1111/jnu.12343
Lang DJ, Wiek A, Bergmann M, Stauffacher M, Martens P, Moll P et al (2012) Transdisciplinary research in sustainability science: practice, principles, and challenges. Sustain Sci 7:25–43. https://doi.org/10.1007/s11625-011-0149-x
Lange S, Vollmer S (2017) The effect of economic development on population health: a review of the empirical evidence. Br Med Bull 121:1
Lapinski MK, Funk JA, Moccia LT (2015) Recommendations for the role of social science research in One Health. Soc Sci Med 129:51–60
Lee L (2017) A bridge back to the future: public health ethics, bioethics, and environmental ethics. Am J Bioethics 17:5–12
Lerner H, Berg C (2015) The concept of health in One Health and some practical implications for research and education: what is One Health? Infect Ecol Epidemiol. https://doi.org/10.3402/iee.v5.25300
Lerner H, Berg C (2017) A comparison of three holistic approaches to health: one health, eco health, and planetary health. Frontiers Vet Sci 4:163. https://doi.org/10.3389/fvets.2017.00163
Lewontin RC (1992) Biology as ideology. The doctrine of DNA. HarperCollins, New York
Logan AC, Prescott SL, Haahtela T, Katz DL (2018) The importance of the exposome and the allostatic load in the planetary health paradigm. J Physiol Anthropol 37(1):15. https://doi.org/10.1186/s40101-018-0176-8
Loring PA, Hinzman MS, Neufeld H (2016) Can people be sentinels of sustainability? Identifying the linkages among ecosystem health and human well-being. Facets 1:148–162
Lovell R, Wheeler BW, Higgins SL, Irvine KN, Depledge MH (2014) A systematic review of the health and well-being benefits of biodiverse environments. J Toxicol Environ Health B 17:1–20
Lysaght T, Capps B, Bailey M, Bickford D, Coker R, Lederman Z, Watson S, Tambyah PA (2017) Justice is the missing link in One Health: results of a mixed methods study in an urban city state. PLoS ONE 12(1):e0170967. https://doi.org/10.1371/journal.pone.0170967
Manlove KR, Walker JG, Craft ME, Huyvaert KP, Joseph MB, Miller RS et al (2016) “One Health” or Three? Publication Silos among the One Health disciplines. PLoS Biol 14(4):e1002448
Marco-Ramell A, de Almeida AM, Cristobal S, Rodrigues P, Roncada P, Bassols A (2016) Proteomics and the search for welfare and stress biomarkers in animal production in the one-health context. Mol BioSyst 12(7):2024–2035. https://doi.org/10.1039/c5mb00788g
McAlpine CA, Seabrook LM, Ryan JG, Feeney BJ, Ripple WJ, Ehrlich AH, Ehrlich PR (2015) Transformational change: creating a safe operating space for humanity. Ecol Soc 20(1):56. https://doi.org/10.5751/ES-07181-200156
McMichael A (2017) Climate change and the health of nations: famines, fevers, and the fate of populations. Oxford University Press, Oxford
Michaels D, Monforton C (2005) Manufacturing uncertainty: contested science and the protection of the public’s health and environment. Am J Public Health 95(Suppl 1):S39–S48
Mutsaers I (2015) One-health approach as counter-measure against “autoimmune” responses in biosecurity. Soc Sci Med 129:123–130
Mwakalimba KK, Green J (2015) ‘One Health’ and development priorities in resource-constrained countries: policy lessons from avian and pandemic influenza preparedness in Zambia. Health Pol Plan 30:215–222
Ostrom E (2009) A general framework for analyzing sustainability of social-ecological systems. Science 325:419–422. https://doi.org/10.1126/science.1172133
Parkes WM, Bienen L, Breilh J, Hsu L-N, McDonald M, Patz AJ et al (2005) All hands on deck: transdisciplinary approaches to emerging infectious disease. EcoHealth 2(4):258–272
Pascual U, Balvanera P, Diaz S, Pataki G, Roth E, Stenseke M et al (2017) Valuing nature’s contributions to people: the IPBES approach. Curr Opin Environ Sustain 26:7–16
Pautasso M, Schlegel M, Holdenriedel O (2015) Forest health in a changing world. Microbial Ecol 69:826–842
Phoenix C, Osborne NJ, Redshaw C, Moran R, Stahl-Timmins W, Depledge MH, Fleming LE, Wheeler BW (2013) Paradigmatic approaches to studying environment and human health: (forgotten) implications for interdisciplinary research. Environ Sci Pol 25:218–228
Rabinowitz PM, Odofin L, Dein FJ (2008) From “us vs. them” to “shared risk”: can animals help link environmental factors to human health? EcoHealth 5:224–229
Rabinowitz PM, Kock R, Kachani M, Kunkel R, Thomas J, Gilbert J et al (2013) Toward proof of concept of a one health approach to disease prediction and control. Emerg Infect Dis 19:e130265. https://doi.org/10.3201/eid1912.130265
Ramsfield TD, Bentz BJ, Faccoli M, Jactel H, Brockerhoff EG (2016) Forest health in a changing world: effects of globalization and climate change on forest insect and pathogen impacts. Forestry 89:245–252
Richardson J, Lockhart C, Pongolini S, Karesh WB, Baylis M, Golgberg T, Slingenbergh J, Gale P, Venturini T, Catchpole M, de Balogh K, Pautasso M, Broglia A, Berthe F, Scans J, Poppy G (2016) Drivers for emerging issues in animal and plant Health. Efsa J 14:Art Unsp S0512
Rittel HWJ, Webber MM (1973) Dilemmas in a general theory of planning. Policy Sci 4:155–169
Rock MJ, Degeling C (2015) Public health ethics and more-than-human solidarity. Soc Sci Med 129:61–67
Rock M, Degeling C (2016) Towards “One Health” promotion. In: Singer M (ed) A companion to the anthropology of environmental health. Wiley, New York, pp 68–82
Rüegg SR, McMahon BJ, Häsler B, Esposito R, Rosenbaum Nielsen L, Ifejika Speranza C et al (2017) A blueprint to evaluate one health. Frontiers Public Health 5:20. https://doi.org/10.3389/fpubh.2017.00020
Ruokolainen L, Lehtimäki J, Karkman A, Haahtela T, von Hertzen L, Fyhrquist N (2017) Holistic view on health: two protective layers of biodiversity. Ann Zool Fennici 54:39–49
Schaeffer DJ, Novak EW (1988) Integrating epidemiology and epizootiology information in ecotoxicology studies. III. Ecosystem health. Ecotoxicol Environ Saf 16(3):232–241
Schelling E, Zinsstag J (2015) Transdisciplinary research and one health. In: Zinsstag J et al (eds) One health: the theory and practice of integrated health approaches. CABI, Oxfordshire, pp 366–373
Shreve C, Davis B, Fordham M (2016) Integrating animal disease epidemics into disaster risk management. Disaster Prev Manag 25:506–519
Stärk KD, Kuribreňa M, Dauphin G, Vokaty S, Ward MP, Wieland B, Lindberg A (2015) One Health surveillance—more than a buzz word? Prev Vet Med 120:124–130
Stengers I (2010) Including nonhumans in political theory: opening Pandora’s Box? In: Braun Whatmore (ed) Political matter: technoscience, democracy, and public life. University of Minnesota Press, Duluth, pp 3–33
Stokols D, Hall KL, Vogel AL (2013) Transdisciplinary public health: definitions, core characteristics and strategies for success. In: Haire-Joshu McBride (ed) Transdisciplinary public health: research, methods and practice. Jossey-Bass, San Francisco, pp 3–30
Tilman D, Clark M (2014) Global diets link environmental sustainability and human health. Nature 515(7528):518–522. https://doi.org/10.1038/nature13959
Tirado F, Gomez A, Rocamora V (2015) The global condition of epidemics: panoramas in A (H1N1) influenza and their consequences for One World One Health programme. Soc Sci Med 129:113–122
Tversky A, Kahneman D (1974) Judgment under uncertainty: heuristics and biases. Science 185:1124–1131
Wald P (2008) Contagious: cultures, carriers, and the outbreak narrative. Duke University Press, Durham
Wallace RG, Bergmann L, Kock R, Gilbert M, Hogerwerf L, Wallace R, Holmberg M (2015) The dawn of structural one health: a new science tracking disease emergence along circuits of capital. Soc Sci Med 129:68–77
Walls HL (2018) Wicked problems and a ‘wicked’ solution. Glob Health 14:34. https://doi.org/10.1186/s12992-018-0353-x
Wenger E (1998) Communities of practice: learning, meaning, and identity. Cambridge University Press, Cambridge
White PJ, Brown PH (2010) Plant nutrition for sustainable development and global health. Ann Bot 105:1073–1080
Whitmee S, Haines A, Breyer C, Boltz F, Capon AG, de Souza Ferreira, Diaz B et al (2015) Safeguarding human health in the Anthropocene epoch: report of the Rockefeller Foundation-Lancet Commission on planetary health. Lancet 386:1973–2028
WHO (2006) Constitution of World Health Organization - Basic Documents. Forty-fifth edition, Supplement, October 2006. First published 1948. World Health Organization: Geneva
WHO (2013) WHO traditional medicine strategy: 2014–2023. World Health Organization, Geneva, p 78
Wiethoelter AK, Beltran-Alcrudo D, Kock R, Mor SM (2015) Global trends in infectious diseases at the wildlife–livestock interface. Proc Natl Acad Sci USA 112:9662–9667
Wilcox BA (2004) Integrating ecohealth in the school of medicine. Hawaii Med J 63(10):316–317
Wild CP (2012) The exposome: from concept to utility. Int J Epidemiol 41:24–32
Wilson EO (1984) Biophilia. Harvard University Press, Cambridge
Woods A, Bresalier M, Cassidy A, Mason Dentinger R (2018) Animals and the shaping of modern medicine: One Health and its histories. Palgrave Macmillan, London. https://doi.org/10.1007/978-3-319-64337-3
Zinsstag J (2012) Convergence of Ecohealth and One Health. EcoHealth 9:371–373
Zinsstag J, Schelling E, Wyss K, Bechir M (2005) Potential of cooperation between human and animal health to strengthen health systems. Lancet 366:2142–2145. https://doi.org/10.1016/S0140-6736(05)67731-8
Zinsstag J, Schelling E, Waltner-Toews D, Tanner M (2011) From “one medicine” to “one health” and systemic approaches to health and well-being. Prev Vet Med 101:148–156
Zinsstag J, Schelling E, Waltner-Toews D, Whittaker M, Tanner M (2015) One Health: the theory and practice of integrated health approaches. CABI and CABI-Europe, Wallingford
Acknowledgements
Open access funding provided by Finnish Environment Institute (SYKE). The lead author produced the initial and refined concepts of the study, performed most of the literature searches and evaluations, wrote the first version of the paper and was responsible for its elaboration. The other authors, listed alphabetically, contributed in various ways through participation in the workshops, collection of additional sources and information, and texts for and commentary on manuscripts. This work was supported by ALTER-Net, Europe’s Ecosystem Research Network, in its High-Impact Action on One Health and EcoHealth, to the employer of the lead author. The work was also supported by funding from the Swiss Federal Research Foundation for a workshop in Magglingen, Switzerland, under Grant No. IZSEZO 177533/1. Dr. Degeling was supported through funding from the National Health and Medical Research Council of Australia [#1083079]. Dr. Irvine’s involvement was supported through funding from the Rural & Environment Science & Analytical Services (RESAS) Division of the Scottish Government. The authors acknowledge the valuable comments and suggestions received by the anonymous reviewers as well as from editors.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Assmuth, T., Chen, X., Degeling, C. et al. Integrative concepts and practices of health in transdisciplinary social ecology. Socio Ecol Pract Res 2, 71–90 (2020). https://doi.org/10.1007/s42532-019-00038-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42532-019-00038-y