Abstract
Purpose
The aim of this study was to quantify surface roughness of carious dentine using noncontact optical profilometry (NCOP) in vitro.
Methods
A total of 20 extracted teeth with root caries were examined according to clinical assessment criteria. NCOP (Proscan 2000, Scantron, Taunton, UK) was used to carry out the surface roughness measurements in vitro. Selection of sampling rate measurements were subsequently performed.
Results
Results showed that the surface roughness (Ra) values were most accurately obtained at a sampling rate of 30 Hz. All lesions had rough texture, with cavitation ranging from 0.5 to 4 mm. Most lesions were leathery, whilst remaining few were soft. There was a significant difference in surface roughness between the carious and sound dentine (p < 0.05). Pearson’s correlation coefficient tests failed to show any significant linear correlation between surface roughness measurements and cavitation (r 0.39; p > 0.05) whilst there was a significant correlation between the hardness and surface roughness (r 0.47, p = 0.04). There was an inverse relationship trend between surface roughness measurements and severity of root caries.
Conclusions
There are limitations due to the sophisticated layout of collage network within the root carious dentine especially cavitated lesions. The NCOP could be considered for the quantification of surface roughness on noncavitated carious dentine in a laboratory setting.
Clinical significance
The effect of different oral health care products on root caries using the NCOP without causing any potential damage to the noncavitated root surface could be assessed prior to the large-scale clinical studies.
Similar content being viewed by others


Introduction
Root caries is an increasing clinical problem in ageing population. Over the last 25 years, the percentage of the population aged 65 and over increased from 15% in 1983 to 16% in 2008, an increase of 1.5 million people in this age group [1]. Root caries remains a dental burden for older people in the twenty-first century and also a challenge to most clinicians. Despite these, there is relatively limited research available on root caries when compared to the enamel caries.
The clinical examination is based primarily on subjective interpretation of surface characteristics, such as integrity, texture, translucency/opacity, location and colour [2, 3]. Texture identification is extensively used by clinicians to aid in the determination of root caries and its activity [4]. Tactile sensation using a blunt probe is to feel the tug back as a sign of the presence of dental caries. Due to the structural differences in coronal and root caries, coronal caries is more likely to be confidently diagnosed at an earlier stage than root caries using visual/tactile methods [4].
Texture of the active lesion is perceived as rough, whilst inactive/arrested lesion presents a smoother surface. Further, the hardness of root carious lesions also depends on its stage of progression; active lesions tend to be soft/leathery whilst arrested lesions are hard [4]. It should also be noted that arrested lesions remain unchanged during several years of observation [5].
Visual examination has been shown to have high specificity with low sensitivity and reproducibility [6, 7]. Recently, ICDAS was proposed to provide defined descriptors of different severity stages of caries lesions [3, 6,7,8]. However, there are still shortcomings and limitations with the ICDAS criteria and root caries. Unfortunately, these clinical criteria are not sensitivity to detect the early root carious lesions and assess the severity of these lesions.
Early detection and noninvasive strategies are desirable with respect to root caries since restorative approach is still challenging with high chances of failures despite the recent advancement in restorative materials. Reversal of root caries is widely accepted to be associated with remineralisation [9] and a corresponding reduction in acidogenic and aciduric micro-organisms [10,11,12].
Noncontact optical profilometry (NCOP) measurements of roughness of dental hard tissues was first introduced in 1972 [13]. Many studies have been reported using the NCOP for quantification of mineral loss in dental hard tissues, however mainly in tooth wear/dental caries/erosion studies of enamel [14,15,16]. To date, there have been no similar studies for assessing the ability of NCOP to measure the surface roughness of carious dentine.
The aim of the study was to use NCOP at the correct settings to quantify the surface roughness of natural root carious lesions.
Materials and methods
Noncontact optical profilometry scanning
The NCOP (Proscan 2000, Scantron, UK) for laboratory use consists of a white light source that transmits white light through a lens and then splits the light beam into a full spectral field (Fig. 1) [17]. The NCOP is capable of rapid surface profiling at rates of up to 1000 measurements per second and can achieve precise measurements both on polished and transparent surfaces with a resolution of 5 nm. There are different sensors with various working ranges and stand-off heights to optimise the measurement for a variety of surfaces, from medical and dental materials with ceramics to a rough paper. The NCOP software package comprises a variety of ISO analytical tools for surface form, finish and feature geometry, as well as area and volume-based measurements.

A schematic diagram of the measurement principles of noncontact optical profilometer
This precise technology is noninvasive and utilises the different refractive indices of the components of white light to measure height differences in sample topography. Surface analysis achieves through splitting the emitted beam inside the profiler into two rays, one is directed to a standardised reference mirror whilst the other ray is directed outside the lens to the surface of the tested sample.
The surface roughness average (Ra) is the arithmetic average height of roughness irregularities measured from a mean line within the measurement length and is the most commonly reported surface roughness parameter. Noncontact optical sensors can be used to analyse the shape, microtopography and roughness of a wide range of surfaces.
Visual-tactile examination for root caries
A total of 20 extracted teeth with root caries was obtained from the Dental Emergency Clinics at Barts and the London School of Medicine and Dentistry, London, UK. Ethical approval was obtained from the Office for Research Ethics Committees Northern Ireland (ORECNI, 16/NI/0101). Each patient signed an informed consent for their extracted teeth to be included in the study.
Each tooth was polished using a slow handpiece and a polishing cup. Texture of each lesion was evaluated by gentle probing (100 g) using an Ash No.6 blunt probe and graded as either smooth or rough. The depth of the cavity was also measured using a periodontal probe with 1-mm intervals.
The mesio-distal and occluso-gingival dimensions of each lesion were measured using a William’s periodontal probe. The hardness of each lesion was assessed using an Ash No.6 blunt probe with a pressure of around 100 g and classified as either soft, leathery or hard. Soft lesions were easily penetrated by the probe whilst leathery lesions had some resistance to withdrawal and hard lesions failed to have any penetration [9,10,11].
The purpose of the severity index (SI) for root caries is to categorise the severity of carious lesions [9,10,11]. This index was based on a score from 0 to 4 (Table 1) taking into account the proximity of each lesion to the dental pulp, size and hardness of the lesions.
Sample preparation
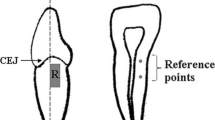
Each tooth was cut to the full depth from the labial/buccal to palatal/lingual surfaces using a diamond cutter saw ensuring that the surfaces contained both root carious lesion and sound dentine. The diamond saw (Struers, Germany) thickness was 0.3 mm and operated at 3000 rpm speed under water lubrication. The samples had the full thickness of the tooth from labial/buccal to palatal/lingual (Fig. 2).

Preparation of the root surfaces with carious lesions
Samples were then embedded onto a customised NCOP tray using a regular set putty (Elite HD+, Zhermack) to ensure the repositioning during repeated scanning process (Fig. 2). Following this procedure, each sample was dried for a period of 5 min at 37 °C before NCOP scanning. During the study period, these samples were stored in deionised water and kept in an incubator at 37 °C.
Scanning method
The NCOP (Proscan 2000, Scantron, Taunton, UK) was used to quantify the surface roughness of root caries and also sound dentine. The sensor used for the measurements was S13/1.2 chromatic sensor (Stil-Sa) presenting a 1.2-mm measuring range with 25-nm vertical resolution. A dark reference background check was performed each time prior to scanning to achieve optimum sensitivity during measurements.
An initial area scan of 1.5 × 1.5-mm dimension was carried out to ensure suitability of the selected area with root caries and without root caries (sound dentine) (Fig. 3). Subsequently, three lines in the X direction were randomly chosen within this scanning area to eliminate any potential missing points for carious lesion and sound dentine. The optimal step size for the area scan (x axis 0.1 mm, y axis 0.1 mm) for root caries and sound dentine was selected. Subsequently, a single line was selected within the lesion in which there were no missing points. A line scan with a length of 1 mm was obtained within 1000 steps at 0.001-mm step size for each lesion and for sound dentine. The NCOP software was used to quantify the surface roughness for each sample (Fig. 4).

The area scan on the root carious lesion

Typical profilometer scan for root carious lesion
Selection of the data collection rate
This study was designed to determine the optimum sampling rate refers to the number of measurements taken per second at each data measurement point. The profilometer used in this study was operated at four different frequencies: 30, 100, 300 and 1000 Hz to select the optimised spectral response of the instrument. Each sample rate combined with seven different averages (1, 2, 4, 8, 16, 32 and 64) respectively.
Reproducibility scans
Reproducibility scans were carried out on same points for the same line using one sample. The sample was scanned 20 times in x-direction from the same line scan whilst the sample was repositioned onto the same starting point with 1000 steps and 0.001 step size after each scan. The data collection frequency was 30 Hz.
Power calculation
Sample size calculation was based on the data from a previous study, where the mean difference between baseline and final scans were 0.32, and the standard deviation of the differences was 0.02 [17]. The statistical power was set to 80% at a level of significance of 0.05 (two sided).
Statistical analysis
Descriptive analysis for each measurement was carried out using SPPSS Version 22 with a confidence level of 95% at p < 0.05. Independent Student’s t test was carried out to analyse any potential differences in surface roughness between carious and sound dentine. Pearson’s correlation coefficient test was chosen to assess the degree of a possible linear relationship between roughness measurements and severity index and hardness of root carious lesions (p < 0.05).
Results
Effect of sampling rate
The Ra values at different rates and averages are shown in Table 2. At the data collection rate of 30 Hz, Ra had the consistent surface roughness values for the root carious dentine when the surface roughness for one sample was carried out at different rates and averages.
Reproducibility scans
Reproducibility scans were carried out on the same points using the same line with one sample. Results of the reproducibility scans are presented in Table 3.
Visual-tactile assessment and roughness measurements for root caries
All natural lesions with root caries had rough texture with cavitation between 0.5 and 4 mm. Majority of these lesions were light to dark brown. A total of 15 lesions were leathery, whilst the remaining 5 were soft (Table 4). Mean of Ra measurements for carious and sound dentine at the sample rate of 30 for each lesion demonstrated wide range of values. Independent Student’s t test showed a significant difference between root carious lesions and sound dentine in surface roughness (p = 0.0001) (Table 5; Table 6).
Pearson’s correlation coefficient test showed that there was an inverse relationship trend between surface roughness measurements and severity of root caries. Soft root carious lesions with SI 4 demonstrated smoother surface characteristics when compared to the less severe lesions (SI 1–3). Interestingly, there was a significant correlation between the hardness and surface roughness of these lesions (r 0.47, p = 0.04) (Fig. 5).

Box plot of surface roughness measurements according to the hardness of root carious lesions (leathery to soft)
Discussion
In this study, quantification of the surface texture changes in root caries was measured using the NCOP method with different data collection rates in a laboratory setting. The repeatability efficiency of this system was also assessed. The surface of carious dentine is irregular with peaks and valleys due to the nature of demineralisation process [14]. Irregular texture of root caries can make surface roughness measurements challenging with various artefacts. Therefore, it is important to use the NCOP method at the correct setting for dentinal lesions.
Data collection rate selection was also crucial for the acquisition of accurate measurements. The results showed that the slower frequency, (30 Hz) provided scans with least missing data when compared to other sample rates (100, 300 and 1000 Hz) for root caries and sound dentine. Since the sample rate refers to the number of measurements taken per second at each data measurement point, slow sampling rate will take more time for measurements and ultimately, more accurate measurements will be achieved. If the reflectivity of the sample is high, there is a little scope in decreasing the sampling rate, since the detector is then “saturated” and there is no advantage to have longer measurements.
At the data collection rate of 30 Hz, Ra had the consistent surface roughness values for the root carious dentine when the surface roughness for one sample was carried out at different rates and averages. Reproducibility scans presented consistent and reliable results. All natural lesions had a rough texture with cavitation between 0.5 and 4 mm. Majority of these lesions were dark and light brown. A total of 15 lesions were leathery, whilst the remaining 5 were soft. Soft root carious lesions with SI 4 demonstrated smoother surface characteristics when compared to the less severe lesions. Interestingly, there was a significant correlation between the hardness and surface roughness of these lesions.
With this respect, it was previously noted that demineralisation of dental hard tissue resulted in loss of its autofluorescence affecting the light scattering ability of the surface [3]. Noncontact optical profilometer operates via a light beam reflection to the sensor. Difficulties encountered in this study were that the irregular dentine lesions had their surfaces with low reflectivity and affected the light beam causing scattering effect. The light beam then failed to reflect back to the sensor completely due to the scattering effect. Therefore, slower sample frequency was found to be more appropriate for measuring root carious surfaces to eliminate data loss.
The sensor used for the measurements in the study was S13/1.2 chromatic sensor (Stil-Sa) presenting a 1.2-mm measuring range with 25-nm vertical resolution. The absorption of light by a surface is a property influenced by the colour of the surface. Shades of surfaces would change the energy absorption properties which would be recognised by the NCOP detector. The outline roughness of the target surface would impact the reflection which would help detector to recognise the degree of the surface texture. Having these two factors give the ability to spectrophotometer to assess the surface. In this study, colour failed to correlate with the surface roughness measurements of these lesions. Bearing in mind that, the reason for this could be related to the similar reflective indices of light brown, brown and dark brown colour.
The structure of dentine is formed by about 45–50 vol% mineral in the form of a carbonated hydroxyapatite with 30–35 vol% of organic matter, which is type I collagen with associated noncollagenous proteins and remaining is the oral fluid whilst enamel is the hardest calcified tissue of the body. Dentinal tubules are usually between 10 nm and 3 μm in diameter. The changes in collagen network of dentine and subsequently effect on surface roughness for natural carious dentine are still not well reported. There was an inverse relationship trend between severity index and surface roughness measurements in this study. It should be noted that the extracted teeth with natural root carious samples had varied range of severity and they were mostly cavitated lesions. The results clearly demonstrated that severe lesions presented low Ra values when compared to noncavitated, leathery and small lesions. It could be speculated that the white light from the NCOP was reflected efficiently without any scattering effect from the flat surfaces of noncavitated lesions and also sound dentine. This resulted in high Ra values for noncavitated lesions and sound dentine in comparison to the cavitated and severe lesions. It can be speculated that NCOP could be considered to measure the surface roughness for early noncavitated lesions without destoring the samples. Another important factor for this outcome is that early root carious lesions exhibited irregular surfaces due to apatite demineralisation where soft lesions had completely loss of collagen network which may have effect the reflection of light to the sensor. There are clearly limitations due to the sophisticated layout of collagen network within root carious dentine especially in severe and cavitated lesions. Therefore, future laboratory-based studies with only noncavitated and less severe type of root carious lesions could be considered to assess if there is any difference with the correlation of clinical assessments and quantification of surface roughness using the NCOP.
There are number of methods to quantify surface roughness in the literature [16, 18, 19]. Few in vitro studies only focus on mineral loss of enamel due to tooth wear (erosion and abrasion). Paepegaey et al. [16] compared contact, noncontact and confocal laser scanning microscopes and surface profilometry measurements for the quantification of wear in restorative materials. Their findings indicated a good agreement between all three methods; however, contact profilometry potentially might damage the surface of study samples. Whereas, surface roughness measurements with noncontact optical profilometry could possibly provide results on carious dentine without touching the surface structure. It should be noted that suitable settings for root caries need to be assessed to eliminate the methodological errors such as loss of data and measuring the artefacts.
Bearing in mind that remineralisation is the optimum management option for early leathery noncavitated lesions [9]. Future laboratory-based studies would be beneficial to investigate the remineralisation effect of oral health care products, dentifrices, mouthwashes, dental varnishes and tooth mouse, on natural lesions in vitro and/or in situ periodically without causing any surface damage.
Conclusions
With the limitations of this laboratory-based study, it is important to use this system with the correct instrument settings. Future laboratory-based studies potentially need to focus on surface roughness of leathery noncavitated root caries using the NCOP without causing any potential damage to the root surface.
References
National Institute on Aging, https://www.nia.nih.gov/2010
Ekstrand KR, Ricketts DN, Kidd EA (1997) Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res 31:224–231
Nyvad B, Fejerskov O (1997) Assessing the stage of caries lesion activity on the basis of clinical and microbiological examination. Community Dent Oral Epidemiol 25:69–75
Fejerskov O (2015) Pathology of dental caries. In: Fejerskov O, Nyvad B, Kidd EA (eds) Dental caries: the disease and its clinical management, 3rd edn. Whiley Blackwell, Oxford, pp 40–81
Banting DW (1993) Diagnosis and prediction of root caries. Adv Dent Res 7:80–86
Bader JD, Shugars DA, Bonito AJ (2001) Systematic reviews of selected dental caries diagnosis and management methods. J Dent Educ 65(10):960–968 ISSN 0022-0337
Ismail AI (2004) Visual and visuo-tactile detection of dental caries. J Dent Res 83(Spec Iss C):C56–C66
Nyvad B, Machiulskiene V, Baelum V (1999) Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 33:252–260
Baysan A, Lynch E, Ellwood R, Davies R, Petersson L, Borsboom P (2001) Reversal of primary root caries using dentifrices containing 5,000 and 1,100 ppm fluoride. Caries Res 35:41–46
Brailsford SR, Shah B, Simons D, Gilbert S, Clark D, Ines I, Adams SE, Allison C, Beighton D (2001) The predominant aciduric microflora of root-caries lesions. J Dent Res 80:1828–1833
Lynch E, Beighton D (1993) Relationships between mutans streptococci and perceived treatment need of primary root-caries lesions. Gerodontol 10:98–104
Schüpbach P, Osterwalder V, Guggenheim B (1995) Human root caries: microbiota in plaque covering sound, carious and arrested carious root surfaces. Caries Res 29:382–395
Marshall GW Jr, Marshall SJ, Kinney JH, Balooch M (1997) The dentin substrate: structure and properties related to bonding. J Dent 25:441–458
Ashmore H, Van Abbe NY, Wilson SY (1972) Measurement in vitro of dentin abrasion by toothpaste. Brit Dent J 133:60–66
Jones RS, Darling CL, Featherstone JD, Fried D (2006) Imaging artificial caries on the occlusal surfaces with polarization-sensitive optical coherence tomography. Caries Res 40:81–89
Paepegaey A-M, Barker ML, Bartlett DW, Mistry M, West NX, Hellin N, Brown LJ, Bellamy PG (2013) Measuring enamel erosion: a comparative study of contact profilometry, non-contact profilometry and confocal laser scanning microscopy. Dent Mat 29:1265–1272
Sleibi A, Tappuni AR, Davis GR, Anderson P, Baysan A (2018) Comparison of efficacy of dental varnish containing fluoride either with CPP-ACP or bioglass on root caries: ex vivo study. J Dent 73:2018–2096. https://doi.org/10.1016/j.jdent.2018.04.009
Schlueter N, Jung K, Ganss C (2016) Profilometric quantification of erosive tissue loss in dentine: a systematic evaluation of the method. Caries Res 50:443–454
Zhang XZ, Anderson P, Dowker SE, Elliott JC (2000) Optical profilometric study of changes in surface roughness of enamel during in vitro demineralisation. Caries Res 34:164–174
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Ethical approval was obtained from the Office for Research Ethics Committees Northern Ireland (ORECNI, 16/NI/0101).
Informed consent
Every patient signed an informed consent for their extracted teeth to be included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Baysan, A., Sleibi, A., Ozel, B. et al. The quantification of surface roughness on root caries using Noncontact Optical Profilometry—An in vitro study. Laser Dent Sci 2, 229–237 (2018). https://doi.org/10.1007/s41547-018-0041-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41547-018-0041-4