
Abstract
This paper proposes a new risk function for lower limb fractures from high rate axial loading, such as that expected in under vehicle explosions. The aim is to improve the prediction of such fractures based on the loads measured by an Anthropomorphic Test Device (ATD) during blast testing. This function has been created by combining data from six different peer-reviewed post mortem human subjects (PMHS) studies. The work, which led to the risk function, considered proximal tibia force as the primary indicator of fracture, with age, sex and body mass considered as covariates. Previous studies considered age as a linear covariate to allow the elderly PMHS population results to be mapped onto a younger population. The literature review as part of this study found, however, that bone strength varies non-linearly with age. Extrapolating bone strength linearly may therefore overestimate the strength of younger populations’ lower limbs. This study uses a non-linear variation of bone strength with age and optimised parameters within this function to produce a Weibull risk curve with a minimum spread. The function described is for loads on the human; for it to be applicable in vehicle testing, there is a need to account for the response of the ATD.
Similar content being viewed by others

Introduction
The aim of this study is to generate a fracture injury risk function for the human leg applicable to high rate axial loads. While the risk function is applicable to high rate loads produced by other means, this work was conducted to inform the development of criteria for assessing the likelihood of injury to personnel in military vehicles exposed to underbelly explosion threats. These assessments are based on the loads measured by an Anthropomorphic Test Device (ATD) during blast testing; criteria development is necessary to produce more appropriate risk functions for loads in the human leg and to account for the differences in the response of the human and ATD legs. The risk functions were produced using existing published data but in doing so have two new aspects. First, this work draws together the widest practical set of data on which to base a criterion by compiling the results of many separate studies. Second, this paper removes some of the variation within lower limb injury data, caused by factors such as age, sex and body mass.
Due to natural variation within a population, there is variation on the risk of fracture of the lower limb. Peak force in the tibia has been shown to correlate best with probability of a disabling lower extremity injury [1, 2] and so is widely used as the main explanatory variable when considering the probability of fracture. Bone fracture is associated with bone strength, which in turn is linearly related to bone mineral density (BMD) [3]. Parameters such as age, sex and body mass are known to influence BMD within an individual [1, 4,5,6,7,8,9].
There are a few sources of published test data where the legs of post mortem human subjects (PMHS) have been subjected to axial loads in a variety of conditions. Different studies treat data in different ways. Yoganandan et al. [4] fitted a two-parameter Weibull distribution to the data by considering non-fracture events as right censored and fracture events as left censored. Other studies, including Funk et al. [1], McKay [2] and Gallenberger [10], use a Weibull distribution but assume fracture events as uncensored.
Funk et al. [1] carried out 43 tests on legs disarticulated at the knee. The foot was set at a neutral posture against a flat plate and impacted axially. Loads were recorded by two load cells, one implanted mid-shaft in the tibia and one between the impactor and foot. The leg was restrained at the proximal tibia. Twenty-two of the test subjects had external tension applied to the Achilles tendon to simulate muscle tension. Acoustic sensors were applied to the bone, and it was found that peak acoustic emission occurred simultaneously with the peak force. This demonstrated that following a fracture, the bone could not continue to carry load, and as such, the peak force reported corresponds to an un-censored data point. Funk et al. [1] considered force, sex, age, body mass, and Achilles tension in fitting a Weibull distribution to the data.
McKay [2] reported tibia force data for 17 tests using a load cell implanted mid-shaft in the tibia. The test specimens included an intact knee joint, with the femur connected to a Hybrid III Anthropomorphic Test Device (ATD). The foot was struck axially to the horizontally positioned tibia, with the femur orientated vertically and the torso of the ATD horizontal. A deformable honeycomb layer between the impactor and footplate was used to manipulate the time history of the force applied to the foot. Weibull, logistic, normal and lognormal distributions were all fitted to the data, with the Weibull distribution being shown to be the best match to the data. Barbir [11] details results from ten impact tests carried out using a similar experimental set up to McKay [2].
Gallenberger [10] describes 54 impact tests conducted on legs disarticulated at the knee, 41 of which had a neutral ankle position, and 13 of which had the ankle dorsi-flexed by 20°. The leg was suspended in order to be horizontal at the time of impact and free to translate horizontally post impact. A proximal tibia load cell was used to record load. For the eight clinically significant injuries reported in the neutral ankle specimens, an acoustic sensor confirmed that the peak axial force recorded was the fracture force for three. In the remaining five, the recorded force at fracture was between 2 and 16% smaller than the peak force. For the logistic regression analysis reported, the un-censored force at fracture was used.
Yoganandan et al. [12] have carried out a meta-analysis of a number of published lower limb impact studies but did not consider Gallenberger [10] or Barbir [11]. Furthermore, data from McKay [2] and Funk et al. [1] were discounted as analysis of the injury force indicated that they were too different (P < 0.05). The authors of the current paper believe that this difference is due to the method of recording the tibia force between the different studies as both McKay [2] and Funk et al. [1] opted for an embedded load cell in the mid-shaft of the tibia. Any load carried by the fibula will not have been captured by this method, in contrast to studies using proximal load cells.
Yoganandan et al. [12] applied a censoring scheme whereby non-fracture data was right censored; if multiple tests were carried out on a single leg, the result was considered to be interval censored between the highest non-injury and the peak injury force, and all other injury tests were considered as left censored. No discussion was presented on the acoustic emission findings in Funk et al. [1] or Gallenberger [10]. A survival analysis considering age as a covariate was carried out for the Weibull, log-normal, normal, and log-logistic distributions. The best fit was reported to be the Weibull distribution and hence was chosen to derive the survival-based risk curve.
Bailey et al. [13] also carried out a meta-analysis of multiple lower limb injury studies. Plantar force was used throughout, due to it being closer to the location of most fractures. Censoring status was applied as follows: right censored for non-injury data points, un-censored for data points where there is evidence that the fracture force is known and left censored for fracture data points where there is no evidence that the force recorded occurred at the fracture force. Force rate was not included as a covariate because of its small contribution to the yield strength of bone under the range of loading rates in the data set. Bailey et al. [13] postulated that by removing samples with evidence of osteoporosis, as was done in the PMHS tests, it can be assumed that bone strength will vary in the same way for both men and women. Bailey et al. [13] considered bone strength to vary linearly with age. As the population used in the survival analysis does not have many samples aged between 20 and 30 years, there is a risk that the extrapolated strength to this age group will overestimate strength.
Methods
Data Set
Data from the following PMHS studies were considered for inclusion in a combined data set: Yoganandan et al. [4] which contained data from earlier work at Wayne State University which does not include the impact velocity [14] (the latter was separated out here), Barbir [11], Funk et al. [1], McKay [2] and Gallenberger [10]. PHMS tests carried out by Owen et al. [15] and Henderson et al. [16] were also reviewed by the authors; however, as they did not report the PMHS sex, those data were not included in this study.
Tests where the ankle was not in a neutral position were excluded from the analysis as Gallenberger [10] reports differences in how the dorsiflexed limb responds. The six remaining studies include 154 individual impact tests on lower limbs with a neutral ankle where a tibia force has been reported. These are detailed in Table 1.
Statistical Analysis and Development of the Risk Function
McKay [2] and Yoganandan et al. [4] both compare a number of statistical distributions and conclude that the Weibull distribution is the best fit for lower limb injury data. This distribution has been used by other workers [1, 12, 16] and has been adopted in this study.
In this study, the authors used the following definitions when interpreting the published data: uncensored, if the load recorded is interpreted as the exact load to cause fracture; left censored, if the load is interpreted as being higher than the minimum load required to cause fracture; and right censored, if the load recorded resulted in no fracture or it was assumed that fracture occurred at a force above that recorded. Following the findings from Funk et al. [1], in which acoustic emission from fracture occurred concurrently with the peak force measured, non-fracture data were considered as right censored and fracture force as uncensored.
MATLAB’s (R2014a, version 8.3, Mathworks, USA) inbuilt Weibull fitting and 95% confidence interval (CI) functions were used to process the data. As the aim of the study was to remove variability from the data by considering population data, a measure of the range of fracture forces in the data was required. In order to capture both the quality of fit (determined by the separation of the 95% CIs) and the range of loads between a low probability of fracture and a high probability of fracture, the measure of spread used was
where
- F 90 % CI_Upper :
-
The force with a 90% probability of fracture on the upper CI
- F 10 % CI_Lower :
-
The force with a 10% probability of fracture on the lower CI
Analysis of the data cited in Table 1 together with data from Owen et al. [15] and Henderson et al. [16], to add statistical power to the observations (as sex was not considered as a factor), found that mid-shaft tibia load cell data under predicted the force of fracture by 14.3% when compared with proximal load cell data. Therefore, the mid-shaft tibia load cell data were included in the combined data set but scaled by 1.167 to account for the load transferred by the fibula and the further distal location of the load cell. The loading rate was not considered as a covariate in this study, as it was not a strong indicator of fracture within the data set, in agreement with Bailey et al. [13].
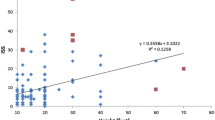
In adulthood, bone strength is widely reported to decrease with age. Ding et al. [5] report that trabecular bone strength decreases significantly with age and data reported by them were used to define a non-linear function with its maximum at 40 years of age. This non-linear trend can be attributed to the post 40 years of age BMD data presented by Funk et al. [1] (Fig. 1). Currey [18] reports that bone strength increases with age up to the age of 15 years, before plateauing between 15 and 40 years. The following function (Eq. 1) is proposed for the variation of fracture risk with age based on fitting a non-linear curve to the data presented by Funk et al. [1] and assuming constant bone strength between 15 and 40 years of age.

Plot of bone mineral density data from PMHS reported in Funk et al. [1], with a second-order polynomial trend line fitted
Age dependent risk function, where
- R a :
-
Risk function linking force and age to the risk of fracture.
- F :
-
Proximal tibia force (kN)
- A :
-
Age (years)
- α :
-
Age weighting parameter (years)
Women tend to have a lower BMD than men, and this gap increases with age [7]. This trend can be seen by plotting the BMD data for the specimens tested in Funk et al. [1] (Fig. 1). A parabola has been fitted to the data, and while there is scatter in the data, it can be seen that the underlying trend, with a maximum at 40, does represent the data once it is considered for each sex independently. For the PMHS data reported in Funk et al. [1], Bailey et al.’s [13] assumption that bone strength variation with age is the same for both sexes does not seem to hold.
Bone mineral content increases with weight-bearing exercise [8]. That increase can be expressed as an increase in BMD, as in the study by Duncan et al. [9]. However, if the measurement of BMD is areal rather than volumetric, the mineral content may be due to changes in geometry. Haapasalo et al. [19] demonstrated the effect of exercise on geometry of the humerus and radius within the dominant arm of tennis players. They concluded that the playing arm’s extra bone mineral, and thus increased bone strength, was mainly due to increased bone size and not due to a change in volumetric bone density. As loading can increase both mineral content and bone bulk, it is expected that heavier people will develop stronger bones. A weak positive correlation between body mass and BMD is found in Funk et al.’s BMD data. [1] Therefore, the risk of fracture is assumed to be inversely proportional to the mass. Consequently, the postulated risk function is updated to include body mass and a body mass weighting parameter (Eq. 2).
Age and mass dependent risk function, where
- R am :
-
Risk function linking force, age and mass to the risk of fracture
- F :
-
Proximal tibia force (kN)
- A :
-
Age (years)
- α :
-
Age weighting parameter (years)
- m :
-
Body mass (kg)
- ω :
-
Body mass weighting parameter (kg)
The values of the body mass weighting parameter and age weighting parameter were simultaneously sampled, and the combination that produced the minimum spread was identified, independently for men and women.
A total of 12 of the 154 data points from these studies do not report a body mass but do report age and sex. As age and sex were expected to have more of an influence on fracture risk than mass, these 12 data points were included in the analysis. Data points where a body mass was not reported were assigned the average mass from the remaining 142 tests in order to minimise their impact on the derivation of the mass weighting parameter.
Using the combined data set in Table 1 and optimising by iteratively searching sample parameters to minimise spread, the risk function in Eq. 3 was derived. The parameters for male were normalised such that the risk function equals the proximal tibia force measured in kN for an 85 kg person aged 40 years or under. To enable the same Weibull distribution to be used for both sexes, the parameters for female function were scaled such that the probability of fracture when the function is applied to the female data set is equal to the probability of fracture for the male data set processed by the male function.
Optimised age, body mass and sex dependent risk function, where
- R amg :
-
Risk function linking force, age, mass and sex to the risk of fracture due to axial loading applied at the foot.
- F :
-
Proximal tibia force (kN)
- A :
-
Age (years)
- m :
-
Body mass (kg)
Equation 4 provides the probability of fracture, Pf, based on the risk curve Ramg defined in Eq. 3. The parameters of the term were calculated by applying a Weibull fit curve to the data after consideration of age, sex and body mass.
Probability of fracture.
Results
Risk curves for an individual population can be derived by scaling the risk function by the reciprocal of the value of Eq. 3 for that population when a unit force is input. Figure 2 details risk curves for four 45-year-old individuals: a 70 kg male, an 85 kg male, a 70 kg female and an 85 kg female by using this method.

Probability of fracture for four populations, all aged 45 years old: 70 kg male and female (top) and 85 kg male and female (bottom). Ninety-five percent of confidence intervals are displayed as dashed lines
Discussion
Censoring
The censoring of injury data points has been handled in a variety of ways by different sources in the literature. Yoganandan et al. [12] treat all injury points as left censored, making the assumption that the fracture may also have occurred at a lower force level. However, based on evidence from Funk et al. [1] and Gallenberger [10], fracture data in the current study has been treated as uncensored. Funk et al. [1] use an acoustic sensor to determine fracture and found that it always occurs at the time of peak force. Gallenberger [10] finds that fracture occurs at or close to the time that peak force occurs. Further, Hasija et al. [20] state that treating the uncensored data as censored will lead to an incorrect risk function. As the authors of the current study are confident in the approach to censoring adopted, the effect of applying different options for censoring within the analysis on the resulting risk function has not been investigated. Further investigation of that aspect, however, could bound the significance of the approach adopted.
Combining Data Sets
It was decided to include tests whereby the tibia was loaded axially with a neutral foot, as it was appreciated that the failure mechanisms within the foot and ankle complex will vary with loading angle and foot posture. Despite the different boundary conditions employed between studies, the shape and duration of the force pulse measured in the leg was similar for each test rig. By conducting a sensitivity study, we found that the variation in time to peak force within the different data sets only has a weak influence on the outcome.
The different load cell locations between the different data sets added complexity to the creation of a risk function from a combined data set. It was found that proximal and distal tibia load cells produce a similar peak force; however, studies that used a mid-shaft tibia load cell were not capturing load transferred though the fibula, thus resulting in a lower peak force. In order to compensate for the lower peak force and include these data points in this study, a ratio of 1.167 was used to adjust the mid-shaft tibial load cell values. This scaling factor is based on the differences between the scale parameter, a, of the Weibull distributions when fitting data from different load cell locations. Inclusion of these data points in the study produces a more consistent data set. As new data appears in the literature that do not provide all of the variables employed within the risk curves developed herein, similar pragmatic approaches may be required to include them and further strengthen confidence in the risk curves. A larger data set will enable more robust set of parameter values to be obtained for the injury risk curves developed and for the reliance on any one such pragmatic approach to be reduced.
Comparison of Risk Curves in Terms of Sex
The risk metrics indicate that females have a lower fracture tolerance than males; however this gap closes as body mass increases. The probability values crossover at around 97 kg; the precise value is age dependent. This is a feature that should be treated with caution due to the limited data available above 90 kg, especially for female PMHSs.
Comparison of Risk Curves with Other Studies
From Table 2, it can be seen that the risk curve derived in this paper predicts a 50% probability of fracture at a higher force of 8.82 kN for a 45-year-old, 75 kg male compared to McKay [2], Yoganandan et al. [12] and Funk et al. [1]. Note that Funk et al. report the force for a 78 kg 45-year-old male so the force would be lower for a 75 kg male. Bailey et al. [13] on the other hand predict a higher force than this study. Only Funk et al. [1] and Bailey et al. [13] consider sex and body mass parameters while McKay [2] does not consider age either.
Conclusions
A new fracture risk function applicable to high rate axial loads has been derived for the human leg by conducting a meta-analysis of available PMHS data. A key aspect of this function is that it is designed to provide a better prediction of the risk of lower limb injuries for a younger population, one that is more representative of military personnel (of both sexes) that may be within military vehicles exposed to explosion threats, than the more elderly PMHS population for which the raw data is available. This new risk function uses a non-linear relationship between bone strength and age which is considered an improvement on the linear relationship used within some existing risk functions. Therefore, it is concluded that this new risk function provides an improved risk prediction capability if the loading exerted on the human were known. However, in military vehicle testing, an ATD is used when assessing the likelihood of such injury due to underbelly blast loading. For this new function to be useful in such testing, a transfer function between the load experienced by a human limb and the load measured by ATDs is required.
References
Funk JR, Khaewpong N, Eppinger RH, Crandall JR, Tourret LJ, CB MM, Patrie JT (2002) The axial injury tolerance of the human foot/ankle complex and the effect of Achilles tension. J Biomech Eng 124(6):750–757
McKay BJ (2010) Development of lower extremity injury criteria and biomechanical surrogate to evaluate military vehicle occupant injury during an explosive blast event. Dissertation, Wayne State University: Detroit
Lancianese SL, Kwok E, Beck CA, Lerner AL (2008) Predicting regional variations in trabecular bone mechanical properties within the human proximal tibia using MR imaging. Bone 43(6):1039–1046
Yoganandan N, Pintar FA, Boynton M, Begeman P, Prasad P, Kuppa SM, Eppinger RH (1996) Dynamic axial tolerance of the human foot-ankle complex. SAE Paper No 962426
Ding M, Dalstra M, Danielsen CC, Kabel J, Hvid I, Linde F (1997) Age variations in the properties of human tibial trabecular bone. J Bone Joint Surg Br Vol 79(6):995–1002
Chen H, Washimi Y, Kubo KY, Onozuka M (2011) Gender-related changes in three-dimensional microstructure of trabecular bone at the human proximal tibia with aging. Histol Histopathol 26(4):563–570
Havaldar R, Pilli SC, Putti BB (2012) Effects of ageing on bone mineral composition and bone strength. J Dent Med Sci 1(3):12–16
Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, Birge SJ (1988) Weight-bearing exercise training and lumbar bone mineral content in postmenopausal women. Ann Intern Med 108(6):824–828
Duncan CS, Blimkie CJ, Cowell CT, Burke ST, Briody JN, Howman-Giles R (2002) Bone mineral density in adolescent female athletes: relationship to exercise type and muscle strength. Med Sci Sports Exerc 34(2):286–294
Gallenberger K (2013). Foot and ankle injuries in variable energy impacts. Dissertation, Marquette University, Milwaukee, Wisconsin, USA
Barbir A (2005) Validation of lower limb surrogates as injury assessment tools in floor impacts due to anti-vehicular landmine explosions. Dissertation, Wayne State University, Detroit. Michigan, USA
Yoganandan N, Arun MW, Pintar FA, Banerjee A (2015) Lower leg injury reference values and risk curves from survival analysis for male and female dummies: meta-analysis of post-mortem human subject tests. Traffic Inj Prev 16(Suppl 1):S100–S107
Bailey AM, McMurry TL, Poplin GS, Salzar RS, Crandall JR (2015) Survival model for foot and leg high rate axial impact injury data. Traffic Inj Prev 12(sup2):S96–S102
Begeman P, Aekbote K (1996) Axial load strength and some ligament properties of the ankle joint. In Proceedings of the Injury Prevention Through Biomechanics Symposium, 125–135
Owen C, Lowne R, McMaster J (2001) Requirements for the evaluation of the risk of injury to the ankle in car impact tests. In 17th International Technical Conference on the Enhanced Safety of Vehicles
Henderson KA, Bailey AM, Christopher JJ, Brozoski F, Salzar RS (2013) Biomechanical response of the lower leg under high rate loading. IRCOBI Conference 2013, IRC-13-24
Seipel RC, Pintar FA, Yoganandan N, Boynton MD (2001) Biomechanics of calcaneal fractures: a model for the motor vehicle. Clin Orthop Relat Res 388:218–224
Currey JD (2002) Bones: structure and mechanics. Princeton University Press, Princeton
Haapasalo H, Kontulainen S, Sievänen H, Kannus P, Järvinen M, Vuori I (2000) Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density: a peripheral quantitative computed tomography study of the upper arms of male tennis players. Bone 27(3):351–357
Hasija V, Takhounts EG, Ridella SA (2011) Evaluation of statistical methods for generating injury curves. 22nd International Technical Conference on the Enhanced Safety of Vehicles, Paper 11–0331
Acknowledgements
SDM acknowledges the financial support of The Royal British Legion.
Funding
The contribution of Frazer-Nash Consultancy was funded by the UK Ministry of Defence under contract DSTLX1000087235. The contribution of Imperial College London was funded by the UK Ministry of Defence under contract DSTLX1000106165.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
Open Access Content includes material subject to © Crown copyright (2018), Dstl. This material is licenced under the terms of the Open Government Licence except where otherwise stated. To view this licence, visit http://www.nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gsi.gov.uk.
About this article

Cite this article
Mildon, P.J., White, D., Sedman, A.J. et al. Injury Risk of the Human Leg Under High Rate Axial Loading. Hum Factors Mech Eng Def Saf 2, 5 (2018). https://doi.org/10.1007/s41314-018-0009-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41314-018-0009-x