
Abstract
Purpose of Review
This article provides an overview of simulation as an effective and evolving tool for teaching clinical pharmacology within the health professions. Further, opportunities for positioning this methodology to meet current educational challenges are presented.
Recent Findings
Clinical pharmacology is an essential core competency for all health professionals, correlating with ability to appropriately and safely prescribe, administer, or optimize medication regimens. Computer-assisted learning became the earliest form of simulation applied to pharmacology teaching, arising from increasing pressure to deviate from animal and tissue experiments in undergraduate education in the 1990s. In the last decade, high fidelity patient simulation, using manikin technology, has demonstrated benefit in building connectivity between knowledge and clinical application within patient care. Serious games, or computer-based educational games, provide an alternative method for creating context, with potential realized for newer technologies like augmented reality. These tools, while beneficial, are not applied in a uniform manner across programs. We advocate for routine incorporation of these tools as they offer significant opportunities to address the challenges faced in today’s healthcare education, particularly with the need for continued social distancing and limitations on in-person educational engagement during coronavirus. Partnership with faculty utilizing simulation in other areas of the curriculum will assist in overcoming potential barriers to implementation.
Summary
Simulation provides various methods that have significant potential to address the challenges in today’s provision of clinical pharmacology education, especially with new directives for social distancing and limitations for in-person educational engagement.
Similar content being viewed by others


Introduction
The complexity of medicine in the living organism and an ever-changing list of advances in technology, knowledge, and discoveries in healthcare have created a rapidly evolving dynamic in educating and training the next generation of providers in all healthcare disciplines. These shifting landscapes of healthcare, education, and the speed at which information is found has offered traditional classroom methods of lecture and assessment novel tools and opportunities using simulation as a lever in a system of reflection, development, and collaborative action. Ultimately, the goals for both the clinician and researcher must be able to understand the application of pharmacology to patient care to achieve the best outcomes through translational research or at the bedside [1•].
As relatively new modalities in education, the formal concept of simulation-based education (SBE) is gaining greater adoption across several professional curriculums in healthcare. Over the last decade, the importance of simulation as a tool in teaching basic sciences has been emphasized by several key bodies governing standards for education in the various healthcare professions [2]. When viewed through the lens of pharmacy, simulation can be used to demonstrate and apply concepts and knowledge from both the basic and clinical science components for learners at all levels from undergraduate to practicing clinicians. Healthcare simulation is an “educational technique that replaces or amplifies real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner” [3]. In a clinical curriculum, it allows progression of skills from novice to expert in a safe environment for both the learner and the simulated patient which is hopefully extrapolated to a real patient. In the basic science curriculum, simulation can supply the context and relevance of the content, which is vital as adult learners must know why something must be learned and how it will advance their experience [4]. This cognition must translate into behavior to impact one’s profession, whether it be within research or clinical practice (Fig. 1). Simulation has been applied in the basic sciences most commonly to teaching physiology but also has obtained a greater foothold in anatomy, biochemistry, and pharmacology [5] by creating important context for these core knowledge bases. When the context of how basic science knowledge applies to clinical careers is lacking, the result is often rote memorization for short-term application instead of gaining the long-term retention and method of applying the knowledge [5, 6].

Miller’s pyramid applied to basic and clinical sciences
Clinical pharmacology is a core of clinical practice competency for healthcare professionals as patient care providers. Within medicine programs, competency-based medical education (CBME) standards recognize the rationale for prescribing as directly correlating with competency in pharmacology [7•, 8]. Anesthesia training is founded on pharmacology and cardiopulmonary physiology [9]. Nursing programs correlate competency in pharmacology with medication safety and medication administration practices [10, 11]. The World Health Organization’s Patient Safety Curriculum Guide speaks to the need for healthcare curricula to integrate patient safety training, including medication safety, uniformly [12]. Pharmacy education recognizes the interconnectivity of clinical pharmacology and therapeutics with many curriculums integrating the teaching of these subjects through collaboration of pharmacology and clinical faculty [13]. A periodic evaluation of teaching concepts finds interactive methods that involve student feedback and immersion using simulation [14] plays a vital role in implementation of novel approaches. Simulation-based education (SBE), in all its forms within healthcare and education, offers a potential solution to address several of these challenges in the basic sciences and professional education realms.
While simulation is an increasingly integrated tool used to teach clinical pharmacology across healthcare programs, variability exists across disciplines and schools in the type and extent to which it is currently applied. The Education Working Group of the European Association for Clinical Pharmacology and Therapeutics identified a significant need to harmonize pharmacology education to improve prescribing proficiency of physicians in a survey of 185 medical schools in 27 countries in the European Union [7•]. They identified that traditional methods remain the backbone for teaching pharmacology; simulation methods were used in only 4–24% of programs [7•]. Simulation-based teaching methods are more commonly applied to clinical curricular components (i.e., therapeutics and experiential training) than basic science curricular components [15]. In a 2013 survey of 88 US colleges and schools of pharmacy, respondents identified in which core competency domains, as defined by the Accreditation Council for Pharmacy Education (ACPE), simulation was applied. Only 31% of respondents said simulation was used for patient safety and 77% for identification and assessment of a drug-related problem as compared with 82% using it for patient assessment and 73% for patient counseling [16].
Simulation has been demonstrated to benefit teaching of clinical pharmacology and remains a useful, if even an underutilized, resource. Given the definitive link between patient safety and clinical pharmacology competency across healthcare professions, we will explore the literature trends in using simulation to teach pharmacology to advocate for continued integration of simulation-based teaching methods with the goal of providing recommendations for establishing uniformity for its use in curricula.
The Current State of Simulation in Teaching Clinical Pharmacology
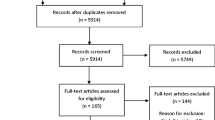
Simulation has been used to teach pharmacology in medicine, nursing, and pharmacy programs. This section explores the current state of simulation for this purpose. Literature was identified through a focused search of English language studies in human subjects using Medline and Google Scholar using the search terms “simulation” and “clinical pharmacology” or “pharmacology” and “pharmacy” or “nursing” or “medicine” and “education.” The resulting body of relevant studies describes the use of simulation, including computer-assisted learning (CAL), high-fidelity patient simulation (HFPS), and serious games, in educating students in clinical pharmacology among health professions programs.
Computer-Assisted Learning in Clinical Pharmacology
Of the various simulation methods used in pharmacology, computer-assisted learning (CAL) has had the longest footing because of its role in providing a new platform for experiments demonstrating core concepts and techniques. Undergraduate pharmacology training had long relied on animal and tissue laboratories. Increasing pressure to find alternatives to animal laboratories opened the door for CAL as educators explored other teaching methods. This shift was driven by a multitude of factors. Ethical concerns surrounded the use of animals for targeting cognitive, not psychomotor, skills development using methods that were largely observational and interpretative. The cost and practical complexity of housing and working with animals, as well as the drugs of interest, also contributed to seeking alternatives [17, 18].
CAL software is designed for pharmacology instruction by mimicking experiments once conducted in animals. Pharmacokinetic (PK) and pharmacodynamic (PD) principles reinforcing core knowledge can be demonstrated in a versatile platform for a broad range of agents without the need to acquire or store large inventories of medications. CAL simulations can teach principles and theoretical concepts, data handling and interpretation skills, communication and report writing skills, as well as experimental design skills [19]. Software commonly has integrated assessment components, allowing for the feedback and reinforcement that is key for success with adult learners. CAL also addresses various learning styles, allowing learners to progress at their own pace. The body of evidence that has evolved since the mid-1990s establishes the efficacy and acceptance of CAL as a method to achieve learning objectives and targeted knowledge development [20,21,22]. Originally focused on undergraduate medical students, more recent studies demonstrate similar applicability across healthcare professions [23,24,25,26,27,28,29] with CAL being superior to graphic illustration methods. [14]
This foundation in CAL is evolving with technological advances, with the most recent studies exploring expansion of CAL into virtual environments. Through multimedia integration of video, animation, and audio, virtual environments increase fidelity, or realness, as compared with CAL. In a recent study of a virtual vs. traditional experimental instruction in pharmacology, pharmacy students demonstrated greater autonomy and innovation within virtual environments [30]. Additionally, new studies have evaluated the feasibility of CAL in resource challenged environments, such as in Sub-Saharan Africa [31]. This study, interestingly, investigated computer programs that were free to download and avoided the expenditures of consumables and equipment associated with traditional wet laboratory experiments. The programs included CyberPatient, OBSim, AutonomiCAL, and Virtual Cat and Virtual Rat (RatCVS) software (Table 1).
High-Fidelity Patient Simulation
As a much newer simulation modality than CAL in teaching pharmacology, high-fidelity patient simulation (HFPS) represents a bridge between the basic and clinical sciences. Its ability to accurately demonstrate pharmacodynamic responses in a human model makes pharmacology relatable to healthcare students. A gap often exists between applying basic science knowledge learned early in curricula to later clinical experiences [6, 7•]; thus, HFPS teaches clinical pharmacology in the same context through which later therapeutics concepts are taught, creating a natural link between the two.
Although research surrounding HFPS use has increased over the last 14 years, this modality of simulation remains underutilized in the teaching of the basic sciences [15]. HFPS has been demonstrated to be an effective tool for both health professions [6, 35,36,37,38,39,40,41,42,43,44,45] as well as PhD [1•] candidates in increasing pharmacology knowledge as well as perceived understanding of the material and its context within both clinical practice and for translational research. Studies have evaluated the clinical pharmacology of multiple agents and classes (Table 2).
Initial studies focused on evaluating whether HFPS provided any perceived or measurable difference in pharmacology knowledge. Studies were conducted largely in students enrolled in pharmacology courses, some with preclinical learners [6, 41, 42] and others with clinical learners [46]. Three studies [6, 41, 42] evaluated the use of HFPS integrated into existing pharmacology courses, recognizing that early learners in healthcare programs lack clinical context for the material taught. Both the medical and nursing students involved in these courses reported increased understanding of the knowledge that influenced their clinical functions of prescribing and management of medications or medication administration, respectively.
More recent studies have evaluated the impact of long-term knowledge retention when HFPS is used to teach pharmacology, which may be increasingly impacted as curricula continue to move toward a problem-based learning (PBL) or organ module format [44]. In a parallel-group, randomized study of medical students, Arcoraci and colleagues [36] demonstrated that HFPS increased both the long-term retention and ability to apply ionotropic pharmacology knowledge to clinical scenarios as compared with traditional lectures or low-fidelity simulation. Students enrolled in a medical school pharmacology course attended a traditional lecture on inotropes and then were randomized to one of three simulation scenarios—a “sham” scenario that involved no pharmacotherapy, a low-fidelity cardiogenic shock scenario, or a high-fidelity cardiogenic shock scenario. Knowledge of the topic was assessed at baseline, after lecture, after simulation, and 90 days after simulation. While all students had comparable knowledge at baseline and after lecture, those in the HFPS group demonstrated significantly higher knowledge retention after simulation and at 90 days.
As healthcare has grown increasingly interprofessional in its teaching and practice, several studies in 2017 evaluated the impact of specific interprofessional integration. In a novel study, Ginzburg and colleagues [37] found that conducting small-group HFPS collaboratively with both basic science and clinical faculty improved the connectivity of basic and clinical knowledge in early medical learners. During the first 100 weeks of the curriculum, students were exposed to integrated course modules that established foundational basic science (e.g., anatomy, pharmacology) and clinical knowledge (e.g. physical diagnosis, medical imaging). At the conclusion of each module, students applied the modules’ content to HFPS scenarios that were then debriefed by both basic science and clinical faculty collaboratively. When surveyed, 95% of students reported that the presence of both faculty members enhanced their understanding of the clinical significance of the basic science content. Furthermore, 91% responded that they understood the role of basic science in patient care. Another study [38] described successful integration of HFPS into an interprofessional activity of 146 s year nursing and pharmacy students who were enrolled in pharmacology courses of similar content. Students’ survey reflected that 91.6% felt that simulation enhanced their pharmacology knowledge and 90.2% reported that it enhanced their understanding of how to apply pharmacology knowledge to patient cases while also developing their interprofessional perceptions and attitudes. Of interest, pharmacy students found the simulation to be more beneficial than the nursing students. Similar increases in confidence and knowledge were found in studies of online, remote teaching pharmacology courses that included recorded HFPS content [43, 47].
Other studies have sought to merge evolving practice safety competencies into pharmacology courses. Sanko and colleagues [40] integrated Quality and Safety Education for Nurses (QSEN) standards using HFPS into a nursing pharmacology course of 120 students, evaluating if doing so impacted student’s confidence and competence, medication adverse events, and observed administration techniques. During the simulations, which involved insulins, heparin, oral antiarrhythmics, and parenteral antibiotics, nurses were required to explain the purpose of the medication and possible adverse effects as part of the QSEN patient-centered competency. Ninety four percent of students reported the activity as being beneficial to their pharmacology knowledge, ultimately increasing safe medication administration competencies.
Consistent with these findings, many other studies of HFPS’ impact acknowledge that engagement in these clinical scenarios increases and reinforces pharmacology knowledge, even if not specifically measured by the investigators [48,49,50,51]. Beyond initial teaching, this structure supports continued reinforcement of knowledge through continued application.
Serious Games
Serious games are the newest modality of simulation discussed here, referring to games played strictly for purposes other than entertainment. As is true for most modalities of simulation, serious games have been used across industries, such as in the military for the rehearsal, training, and exploration of military options [52•]. These options vary from single role player games where the learner completes specific lessons and challenges to either provide care to a single avatar patient or networked multiple player disaster scenarios that train for emergency medical surge capacity and command.
Low-fidelity (non-computer) games have been described, such as adaptations of popular card and board games focusing on pharmacology content. In junior baccalaureate nursing students, a “Pharmacology Go Fish” card game was used in small groups to successfully review for the comprehensive final exam [53]. In “AntimicroGAME”, Polish medical students enrolled in a pharmacology course engaged in a board game that focused on the bacteriology and antimicrobial mechanism of action content of the course in preparation for the final exam [54]. While neither of these descriptions demonstrated superiority over traditional techniques, they reflect the recognized need described earlier to actively engage adult healthcare learners.
A pilot study in 79 third-year baccalaureate nursing students demonstrated a statistically significant improvement in knowledge of opioids and management of postoperative pain, additionally correlating with increased student confidence, while using a serious game during a pharmacology course [55]. Students review the provided materials and listen to a recorded shift sign out before logging into an e-classroom platform. Here they entered the game, applying pharmacology knowledge to clinical assessment, with their decisions altering the course of events that unfolded in the patient’s postoperative course.
In a group of pharmacy learners, serious games corresponded with increased knowledge in cardiac pharmacology [56]. This group used gaming templates available online from Articulate Global, Inc. that provided at least two of the following desired characteristics: points, levels, and achievement, were competitive, were interactive, were challenging, and promoted collaboration. These authors noted that current availability of gaming tools does not require dedicated funding or advanced technological skills, addressing two common barriers that sometimes lead to the limited application of simulation technologies.
These representative studies reflect the potential for serious games in teaching pharmacology but also highlight the need for further research to identify the key aspect of gaming platforms that correlate with both short- and long-term knowledge retention. While student satisfaction with interactive teaching methods is consistent across studies, varying results have been reported regarding improvement over traditional methods [55,56,57,58].
Challenges and Opportunities: The Future of Simulation for Teaching Clinical Pharmacology
The use of simulation has been demonstrated to be effective in enhancing knowledge and creating the context linking basic and clinical sciences, allowing students to apply core knowledge to patient care [59••]. While CAL, HPFS, and serious games have been useful tools in teaching pharmacology and most commonly CAL for replacing undergraduate animal experiments, none are applied in a routine or uniform manner across disciplines or curricula, highlighting an opportunity to optimize the use and positioning of these tools in undergraduate healthcare education.
So why has there not been more uniform adoption of these technologies? Many barriers must be considered. While CAL and serious games are available as free or low-cost software and require no specialized training for educators, HFPS is associated with cost and special skill sets. HFPS requires access to costly manikins as well as faculty and staff with sufficient training required to operate the equipment and orchestrate the sessions. While some schools own manikins, others require partnership with simulation facilities for such access. Manikins require upgrades and maintenance and thus are at risk of becoming outdated without dedicated ongoing resources to maintain their intended level of fidelity. Additionally, there is a technical proficiency required of faculty to appropriately match learning objectives with available technology, and the appropriate fidelity levels are a concern for efficiency and budgeting.
Recent challenges in the use of simulation from COVID-19 have also pushed the boundaries and necessitated innovations in simulation. Considerations for student’s safety and access in clinical areas have created both challenge and opportunity, allowing simulation to fill needs as learning shifts from in-person experience to remote experiences. Social distancing has impacted even the routine use of simulation in our pharmacy and medical schools when students were not allowed to physically attend the simulation instruction session. Leveraging Cisco’s WebEx meetings and CAE’s Learning Space video recording system, our simulation center was able to use simulation to meet these needs by bringing the teams of learners into a teleconference platform, limiting physical contact for both learners and educators, in a manner that continued to meet educational objectives. This blending of remote human interaction with manikins and teachers through teleconferencing has demonstrated both the capacity and limitations of simulation to address unique challenges. Latency of video and audio connections, internet bandwidth or connectivity interruptions, and hardware problems can each create potential failure points toward the objectives of teaching. This has highlighted that simulation educators must be adaptable, having contingency plans to achieve the simulation objectives based on available resources and circumstance.
The cost of operating a simulation program can vary widely from ultra-low cost using student role models or low-fidelity task trainers made by healthcare simulation operation specialists costing a few dollars to expensive video capture servers and holographic technology. While resources are typically considered a high barrier for entry, not all simulation requires large balance sheets. For example, the inaugural use of simulation studied in Sub-Saharan Africa to teach midwifery skills prior to entering the clinical environment used part-task trainers and role players [60] to achieve learner confidence like traditional instruction. Educational research will need to continue to identify the best application of resources and find the optimal applications for pharmacology instruction.
The evolution of newer and cheaper technology will continue to cause the use of simulation to improve and reach into even more applications of pharmacy and education. The use of VR technology may also offer new opportunities to pharmacology all the way up to and include the patient interaction. According to Fox and Felkey [61] the use of VR applications could provide visual and auditory instructions to patients regarding standard medication safety and efficacy and yield better therapy compliance. VR head-mounted displays can be used to illustrate the best choice of a drug design or alternative treatments to a prescriber and be shared with the patient to improve understanding and ultimately compliance.
Virtual reality (VR) and augmented reality (AR) options have been developed to run entire scenarios in a computer-constructed setting of the operating room or bedside at the clinic, but severe limitations in the control technology will need to be overcome to make a seamless experience for the user. Currently, most VR simulations require the user to hold a physical controller like the OCULUS Quest/Rift Touch Controller or HTC Vive to achieve selections and haptic feedback. These gaming controllers or similar devices that collect position data and offer buttons to make commands require additional learning by the user. As new VR headsets are continuously introduced into the market and improve the immersive environment still suffer from substantial limitations of their controllers in terms of functionality and ability to capture the user’s gesture and movements in a natural way [62].
In the learning environment, augmented reality currently offers a better blending of physical equipment such as the high-fidelity manikin with a visualization platform like Microsoft HoloLens. This allows the haptics to be generated on a larger platform of the body and includes intangible learning on body posture, personal limitations, and even endurances. Augmented reality systems can be used to construct a setting that in turn can be used for other pharmacy-related endeavors such as systems engineering, process management, and research into latent safety threats that can be identified in the environment before it is physically built.
The pandemic response and adaptations made necessary since the entrance of COVID-19 creates a potential opportunity to innovate and reconsider the positioning of the technology of simulation and the value to educators. On the cutting edge of simulation, we find the opportunities to innovate therapy and solutions to emerging pathogens such as SARS-CoV-2 and include the call for timely in silico modeling and simulation supporting basic science and translational scientists’ research in drug discovery and support rapid proposal of clinical trials. There is a sub-segment of computer-based simulations that leverage modeling into “virtual clinical trial populations” that can be used to run parallel to existing clinical trials and allow the researcher and learner to experiment virtually to test efficacy and safety. This again creates an influx of opportunity for specific medication data that in turn may further drive the development of future clinical simulations involving the decisions and capacity of a simulated patient avatar considering economics, side effect profiles, and even cultural and social determinates into the scenario.
Recognition and Comments on Overcoming Barriers to Implementation
Fostering a formal mentorship in simulation is useful, since many disparate healthcare educational programs already use simulation, in various components of their curricula. In clinical pharmacology, a coordinated pairing of experienced with the novice simulation educators will help the faculty to better understand the potential of the available technology within their courses and ease the development of activities that might otherwise seem overwhelming for those not familiar with the session development and flow process or the technology involved. This partnership also supports overall curricular development, since earlier exposure to various cases will likely require any existing simulation cases to evolve in complexity for the learners. Additionally, the need for simulation faculty should not be overlooked or underestimated as the number of simulation faculty is associated to the degree of SBE implementation [63].
In pharmacology, there is great potential for simulation-based education. The routine application of CAL to replace animal laboratory work is well established and has been beneficial. HFPS allows demonstration of PD/PK concepts in a manner that automatically links and engages the student’s other fundamental knowledge, such as physiology. Newer technologies, such as VR/AR, provide computer modeling and simulation of bioactive compounds in either a physical or virtual classroom, which can be particularly helpful in assisting visual learners in embracing concepts when presented beyond simple two-dimensional drawings.
We propose to anyone considering the integration of the various forms of simulation to start with a gap analysis and plan stepwise integration with feedback and development. If a course of instruction is amenable to applying simulation, identify one to two lessons to begin, increasing each semester based on feedback from the faculty and learners and increased with experience in performing the simulations. Create working partnerships with the faculty already applying simulation within the curriculum to support faculty, as well as curricular, development. Such partnerships from faculty across the curricula have the potential to shape a continuity of learning that is seamless and strongly integrated from the learner’s perspective.
Conclusions
Simulation teaching methods create context and a bridge between basic and clinical science content. While CAL and HFPS are currently used in the teaching of pharmacology across the health professions, simulation application remains inconsistent, and standards have yet to be established, leaving potential for optimizing and leveraging these teaching methods. Applying these technologies strengthens health professions of students’ ability to solidify pharmacology knowledge as the essential core for their discipline-specific practices, such as prescribing, medication administration, and medication regimen optimization. Consistent with trends in healthcare education, collaboration between basic science and clinical faculty during simulation creates the natural relationship between pharmacology and patient care. Given the more frequent application of simulation for clinical content, such partnership also can assist with overcoming barriers to implementing simulation within the basic sciences as they relate to technology familiarity, faculty comfort, and session design.
A holistic approach to integrating clinical to basic sciences using the entire spectrum of simulation modalities offers a golden opportunity to connect the learner with a safe and efficient system of care in the future. It allows them to model and experience the application of their knowledge within the context of relationships with their patients and colleagues to form aspirational healthcare system. We recommend a move toward standardizing the role and placement of simulation in pharmacology as a key element of bridging these essential foundations and patient care.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
• Bosseau Murray W, Wood J, Schwab M, Fritz M, Karpa KD. Human patient simulation in pharmacology graduate education: bridging the bench-to-bedside gap. Mol Interv. 2010;10(3):127–32. https://doi.org/10.1124/mi.10.3.2. Although a decade old, this article is one of few that specifically addresses the benefit of simulation in pharmacology education to bridge the gap that currently exists from “bench-to-bedside.
Cooke M, Irby D, O’Brien BC. Educating physicians: a call for reform of medical school and residency. San Francisco, CA: Jossey-Bass; 2010.
Gaba DM. The future vision of simulation in health care. Quality and Safety in Health Care. 2004;13(suppl1):i2–i10. https://doi.org/10.1136/qshc.2004.009878.
Knowles MS. The adult learner: a neglected species. Rev. ed. Houston, US: Gulf Publishing Company; 1990.
Eason M. The use of simulation in teaching basic science. Curr Opin Anesthesiol. 2013;26:721–5.
Thompson TL, Bonnel WB. Integration of high-fidelity simulation in an undergraduate pharmacology course. J Nursing Ed. 2008;47(11):518–21. https://doi.org/10.3928/01484834-20081101-10.
• Brinkman D, Tichelaar J, Okorie M, Bissell L, Christiaens T, Liki R, et al. Pharmacology and therapeutics education in the European Union needs harmonization and modernization: a cross-sectional survey among 185 medical schools in 27 countries. Clin Pharmacol Ther. 2017;102:815–22. https://doi.org/10.1002/cpt.682. This EU based statement highlights the potential for standardization in pharmacology education in medical education.
Shah N, Desai C, Jorwekar G, Badyal D, Singh T. Competency-based medical education: an overview and application in pharmacology. Indian J Pharmacol. 2016;48(Suppl 1):S5–9. https://doi.org/10.4103/0253-7613.193312.
Lipps J., Meyers L. Undergraduate Medical Education. In: Mahoney B., Minehart R., Pian-Smith M. (eds) Comprehensive Healthcare Simulation: Anesthesiology. Comprehensive Healthcare Simulation. Springer, Cham; 2020.
Lee SE, Quinn BL. Incorporating medication administration safety in undergraduate nursing education: a literature review. Nurse Educ Today. 2019;72:77–83. https://doi.org/10.1016/j.nedt.2018.11.004.
Gil M, Anderson E, Hilsmann N. Best practices for teaching pharmacology to undergraduate nursing students: a systemic review of the literature. Nurse Educ Today. 2019;74:15–24. https://doi.org/10.1016/j.nedt.2018.11.017.
Farley D, Zheng H, Rousi E, Leotsakos A. Field test of the World Health Organization Multi-Professional Patient Safety Curriculum Guide. PLOS ONE 2015;10(9): e0138510. https://doi.org/10.1371/journal.pone.0138510
ACPE. Accreditation standards and key elements for the professional program in pharmacy leading to the doctor of pharmacy degree. Chicago: IL; 2016. Available at: https://www.acpe-accredit.org/pdf/Standards2016FINAL.pdf.
Kaur G, Garg P, Sharma V, Singh J, Matreja PS, Khanna PML. Comparison of computer simulation and graphical illustration for teaching experimental pharmacology to undergraduate students. Int J Basic Clin Pharmacol 2017;6:788–794. Doi:https://doi.org/10.18203/2319-2003.ijbcp20171082
Helyer R, Dickens P. Progress in the utilization of high-fidelity simulation in basic science education. Adv Physiol Educ. 2016;40:143–4. https://doi.org/10.1152/advan.00020.2016.
Vyas D, Bhutada NS, Feng X. Patient simulation to demonstrate students’ competency in core domain abilities prior to beginning advanced pharmacy practice experiences. Am J Pharm Educ. 2012 Nov 12;76(9):176. https://doi.org/10.5688/ajpe769176.
John LJ. A review of computer assisted learning in medical undergraduates. Journal of Pharmacology and Pharmacotherapeutics 2013;4(2):86–90. Doi:10.4103%2F0976-500X.110870.
Badyal DK, Desai C. Animal use in pharmacology education and research: the changing scenario. Indian J Pharmacol 2014;46:257–65. Doi:10.4103%2F0253–7613.132153.
Hughes IE. Computer-based learning an aid to successful teaching in pharmacology? Naunyn Schmiedeberg's Arch Pharmacol. 2002;366:77–82. https://doi.org/10.1007/s00210-002-0552-z.
Dewhurst DG, Hardcastle J, Hardcastle PT, Stuart E. Comparison of a computer simulation program and a traditional laboratory practical class for teaching the principles of intestinal absorption. Am J Phys. 1994;267:S95–104. https://doi.org/10.1152/advances.1994.267.6.S95.
Leathard HL, Dewhurst DG. Comparison of cost effectiveness of a computer assisted learning program with tutored demonstration to teach intestinal motility to medical students. ALT-J. 1995;3:118–25. https://doi.org/10.1080/0968776950030119.
McAteer E, Neil D, Barr NBrown M, Draper S, Henderson F. Simulation software in a life sciences practical laboratory. Computers and Education. 1996;26:101–12. https://doi.org/10.1016/0360-1315(96)00011-5.
Ezeala CC, Ram AA, Vulakouvaki N. Learning gain of pharmacy students after introducing guided inquiry learning with computer simulation in a pharmacology course in Fiji. J Educ Eval Health Prof 2013:10;9 • Doi:https://doi.org/10.3352/jeehp.2013.10.9
Struys MMRF, DeSmit T, Mortier EP. Simulated drug administration: an emerging tool for teaching clinical pharmacology during anesthesia training. Nature. 2008;84(1):170–4. https://doi.org/10.1038/clpt.2008.76.
Amirtha R, Gupta R, Rehan HS. Impact of computer assisted teaching as teaching modality on learning & understanding of pharmacology among undergraduate medical students. Indian J Physiol Pharmacol. 2017;61(2):202–7.
Al-Sallami H, Loke SK. Learning a complex dose-response relationship with the computer simulation CoaguSim. Currents in Pharmacy Teaching and Learning. 2018;10:1406–13. https://doi.org/10.1016/j.cptl.2018.07.009.
Dewhurst D. Is it possible to meet the learning objectives of undergraduate pharmacology classes with non-animal models? AATEX. 2008;14:207–12.
Badyal DK, Madgill V, Kaur J. Computer simulation models are implementable as replacement for animal experiments. ATLA 2009;37:191–195. Doi:10.1177%2F026119290903700208.
Wang L. Computer-simulated pharmacology experiments for undergraduate pharmacy students: experiences from an Australian university. Indian Journal of Pharmacology. 2001;33:280–2.
Zhao C, Wang L, Qu M, Li W, Yanna LV, Kong Y, et al. Application of simulation teaching in pharmacology experimental teaching. International Conference on Education Research, Economics and Management 2019;118–121. Doi:https://doi.org/10.12783/dtem/icerem2019/30816
Ezaela CC. Integration of computer-simulated practical exercises into undergraduate medical pharmacology education at Mulungushi University, Zambia. J Educ Eval Health Prof 2020;17:8. Doi:https://doi.org/10.3352/jeehp.2020.17.8.
Bolger MB. Cyber patient [Internet]. LabSoft Solutions [cited 2020 Feb 20]. Available from: http://labsoft.com/software.html.
University of Strathclyde. Strathclyde pharmacology simulations [Internet]. Glasgow: University of Strathyberclyde [cited 2020 Feb 16]. Available from: http://spider.science.strath.ac.uk/ sipbs/software_sims.htm.
Lew MJ, Kennedy GE, Ziogas J. A CAL for learning about autonomic drugs through hypothesis-based exploration [Internet]. San Francisco (CA): Scribd HQ [cited 2020 Feb 20]. Available from:. https://www.scribd.com/document/62544351/Read- Me.
Pereira N, Udaykumar P, Sherif L. Simulation based learning methodology in pharmacology: knowledge and perception among second year medical under-graduate students. Int J Basic Clin Pharmacol 2019;8:420–4. Doi:https://doi.org/10.18203/2319-2003.ijbcp20190510
Arcoraci V, Squadrito F, Altavilla D, et al. Medical simulation in pharmacology learning and retention: a comparison study with traditional teaching in undergraduate medical students. Pharmacol Res Perspect. 2018;e449. Doi:https://doi.org/10.1002/prp2.449
Ginzburg S. Brenner J, Cassara M, Kwiatkowski T, Willey JM. Contextualizing the relevance of basic sciences: small-group simulation with debrief for first and second-year medical students in an integrated curriculum. Advances in Medical Education and Practice 2017:8 79–84. Doi:10/2147/AMEP.S124851
Meyer BA, Seefeldt TM, Ngorsuraches S, Hendrickx LD, Lubeck PM, Farver DK, et al. Interprofessional education in pharmacology using high-fidelity simulation. Currents in Pharmacy Teaching and Learning. 2017;9:1055–62. https://doi.org/10.1016/j.cptl.2017.07.015.
Mueller MP, Christ T, Dobrev D, Nitsche I, Stehr SN. Ravens U, et al. Teaching antiarrhythmic therapy and ECG in simulator-based interdisciplinary undergraduate medical education British Journal of Anaesthesia. 2005;95(3):300–4. https://doi.org/10.1093/bja/aei174.
Sanko JS, McKay M. Use of simulation-enhanced pharmacology education in pre-licensure nursing education. Nurse Educ. 2017;42(5S):S32–7. https://doi.org/10.1097/NNE.0000000000000409.
Seropian M, Dillman D, Lasater K, Gavilanes J. Mannequin-based simulation to reinforce pharmacology concepts. Sim Healthcare. 2007;2:218–23. https://doi.org/10.1097/SIH.0b013e31815b156b.
Kasturi R, Heimburger G, Nelson E, Phero J, Millard RW. 2009. Does human simulator-aided learning improve long-term retention of autonomic pharmacology concepts and facts by year II medical students? Med Sci Educ. 2009;19(3):89–94.
Via DK, Kyle RR, Trask JD, Shields CH, Mongan PD. Using high-fidelity patient simulation and an advanced distance education network to teach pharmacology to second year medical students. J Clin Anesth. 2004;16:144–51. https://doi.org/10.1016/j.jclinane.2003.09.001.
Gorman L, Castigliono A, Hernandez C, Asmar A, Cendan J, Harris D. Using preclinical high-fidelity medical simulations to integrate pharmacology and physiology with clinical sciences. Medical Science Educator 2015;25(4):521–532. Doi:10/1007/s40670–015-0173-z.
Hassan Z, DiLorenzo MA, Amy MA, Sloan P. Teaching opioid pharmacology with the human patient simulator. Journal of Opioid Management. 2010;6(2):125–13. https://doi.org/10.5055/jom/2020.0012.
Morgan PJ, CleaveHogg D, Desousa S, Lam-Mcculloch J. Applying theory to practice in undergraduate education using high fidelity simulation. Medical Teacher. 2006;28(1):e10–5. https://doi.org/10.1080/01421590600568488.
East L, Hutchinson M. Evaluation of a filmed clinical scenario as a teaching resource for an introductory pharmacology unit for undergraduate health students: a pilot study. Nurse Educ Today. 2015;35:1252–6. https://doi.org/10.1016/j.nedt.2015.04.009.
Alluri RK, Tsing P, Lee W, Napolitano J. A randomized controlled trial of high-fidelity simulation versus lecture-based education in preclinical medical students. Medical Teacher. 2016;38(4):404–9. https://doi.org/10.3109/0142159X.2015.1031734.
Konieczy L. Using high-fidelity simulation to increase nursing student knowledge in medication administration. Teach Learn Nurs. 2016;11:199–203. https://doi.org/10.1016/j.teln.2016.08.003.
Seybert AL, Kane-Gill S. Elective course in acute care using online learning and patient simulation. Amer J Pharm Ed 2011;75(3):Article 54. Doi:10.5688%2Fajpe75354.
Seybert AL, Kobulinsky LR, McKaveney TP. Human patient simulation in a pharmacotherapy course. Amer J Pharm Ed 2008; 2008:72(2):Article 37. Doi:10.5688%2Faj720237.
• Lioce L. (Ed.), downing D, Chang TP, Robertson JM, Anderson M, Diaz DA, and Spain AE (Assoc. Eds.) and the terminology and concepts working group (2020), healthcare simulation dictionary –Second Edition. Rockville, MD: Agency for Healthcare Research and Quality; January 2020. AHRQ Publication No. 20-0019. DOI: https://doi.org/10.23970/simulationv2, 2020. This reference is the official dictionary for simulation per the Society of Simulation in Healthcare, thus a great reference for teachers newly considering simulation in their instruction.
Kaylor SK (letter). Fishing for pharmacology success: gaming as a strategy for interactive learning. J Nurse Ed 2016;55(2):119. Doi:https://doi.org/10.3928/01484834-20160114-12
Karbownick MS, Wiktorowska-Owczarek A, Kowalczyk E, Mokros L, Pietras T. Board game versus lecture-based seminar in the teaching of pharmacology of antimicrobial drugs—a randomized controlled trial. FEMS Microbiol Lett. 2013;363(7):1–9. https://doi.org/10.1093/femsle/fnw045.
Lancaster RJ. Serious game simulation as a teaching strategy in pharmacology. Clinical Sim in Nursing. 2014;10:e129–37. https://doi.org/10.1016/j.ecns.2013.10.005.
Lee CY, White PJ, Malone DT. Online educational games improve the learning of cardiac pharmacology in undergraduate pharmacy teaching. Pharm Educ. 2018;18(1):298–302.
Valente P, Lora PS, Landell MF, Schiefelbein CS, Girardi FM, Souza LDR, et al. A game for teaching antimicrobial mechanisms of action. Med Teach. 2009;31:e383–92. https://doi.org/10.1080/01421590802637958.
Buur JL, Schmidt PL, Barr MC. Using educational games to engage students in veterinary basic sciences. J Vet Med Educ. 2013;40:278–81. https://doi.org/10.3138/jvme.0113-014R.
•• Seybert AL, Smithburger PL, Benedict NJ, Kobulinksy LR, Kane-Gill SL, Coons JC. Evidence for simulation in pharmacy education. J Am Coll Clin Pharm. 2019;2:686–92. https://doi.org/10.1002/jac5.1167. This article, authored by the most proliferative researcher in pharmacy simulation education, is a recent and comprehensive update as to the state of simulation use in pharmacy education.
Tyer-Viola L, Zulu B, Maimbolwa M, Guarino A. Evaluation of the use of simulation with student midwives in Zambia. Int J of Nursing Ed Scholarship. 2012;9(1). Doi:https://doi.org/10.1515/1548-923X.2379.
Fox BI, Feckly BG. Virtual reality and pharmacy: opportunities and challenges. Hosp Pharm. 2017;52(2):160–1. https://doi.org/10.1310/hpj5202-160.
Marchesi M, Ricco, B. GLOVR: a wearable hand controller for virtual reality applications. RIC '16: Proceedings of the 2016 Virtual Reality International Conference. 2016;18:1–2. Doi:https://doi.org/10.1145/2927929.2927959
Takahashi J, Shiga T, Funakoshi H, Homma Y, Mizobe M, Ishigami Y, et al. Association of the number of simulation faculty with the implementation of simulation-based education. Simul Healthc. 2019;14(4):223–7. https://doi.org/10.1097/SIH.0000000000000360.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interest or financial disclosures, actual or perceived, relevant to this manuscript. The opinions expressed by the authors in this publication are those of the authors and do not necessarily reflect those of the authors’ employer.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Clinical Pharmacology
Rights and permissions
About this article

Cite this article
Andrews, L.B., Barta, L. Simulation as a Tool to Illustrate Clinical Pharmacology Concepts to Healthcare Program Learners. Curr Pharmacol Rep 6, 182–191 (2020). https://doi.org/10.1007/s40495-020-00221-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40495-020-00221-w