
Abstract
Background
In the management of chronic obstructive pulmonary disease (COPD), knowledge of disease attributes and preferences that are important to patients is crucial. This knowledge may support drug development and optimization of COPD management strategies.
Objective
To assess patient preferences in COPD and to use the conjoint methodology in order to propose a self-assessment tool based on patients’ preferences gained from this conjoint analysis. This tool might then be used in future observational study settings.
Methods
A two-step procedure was applied: an initial qualitative research module consisting of interviews with eight COPD patients served to assess COPD patients’ health state in-depth, their attitudes towards COPD and their information sources regarding the disease, symptomatology, unmet needs, and their preferences for future COPD medications. In the main quantitative research part of the study, 300 patients (with an average age of 55 years) from across Germany suffering from COPD (n = 225 with stage II and n = 75 with stage III COPD) participated. Each participant was presented with 15 different scenarios during the conjoint exercise. Additionally, the Clinical COPD Questionnaire (CCQ) had to be completed and attitudes towards COPD were assessed.
Results
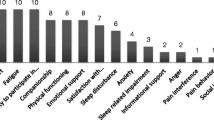
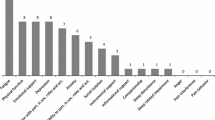
According to the participants, the three COPD attributes of the highest relative importance were dyspnea, performance capability, and sleep quality. Frequency of administration of the medication, onset of medication, and emotional state due to COPD base medication played only a minor role. COPD symptoms were reported to have the highest impact on quality of life, according to the CCQ.
Conclusions
Our study proposes an alternative utility-based approach of a self-reported health state concept, utilizing the fact that patients with moderate to severe COPD would trade, e.g., ease of administration and onset of medication for relief from dyspnea.

Similar content being viewed by others

References
WHO. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach. Geneva: World Health Organization; 2007.
Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–73.
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442.
Mittmann N, Kuramoto L, Seung, et al. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med. 2008;102(3):413–21.
Agh T, Inotai A, Meszaros A. Factors associated with medication adherence in patients with chronic obstructive pulmonary disease. Respiration. 2011;82(4):328–34.
Dolce JJ, Crisp C, Manzella B, et al. Medication adherence patterns in chronic obstructive pulmonary disease. Chest. 1991;99(4):837–41.
Bosley CM, Parry DT, Cochrane GM. Patient compliance with inhaled medication: does combining beta-agonists with corticosteroids improve compliance? Eur Respir J. 1994;7(3):504–9.
Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: a randomized trial. Med Care. 1999;37(1):5–14.
Hyland ME, Stahl E. Asthma treatment needs: a comparison of patients’ and health care professionals’ perceptions. Clin Ther. 2004;26:2141–52.
Ryan M. Discrete choice experiments in health care. BMJ. 2004;14(328):360–1.
Ryan M, Farrar S. Using conjoint analysis to elicit preferences for health care. BMJ. 2000;320(7248):1530–3.
Haughney J, Partridge MR, Vogelmeier C, et al. Exacerbations of COPD: quantifying the patient’s perspective using discrete choice modelling. Eur Respir J. 2005;26(4):623–9.
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. GOLD; 2011. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2011_Feb21.pdf. Accessed 30 Jan 2013.
McFadden D, Train K. Mixed MNL models for discrete response. J Appl Econ. 2000;15(5):447–70.
Kuhfeld WF. Marketing research methods in SAS: experimental design, choice, conjoint, and graphical techniques [SAS 9.2 ed.]. Cary (NC): SAS Institute Inc.; 2010.
van der Molen T, Willemse BW, Schokker S, Ten Hacken NH, Postma DS, Juniper EF. Development, validity and responsiveness of the Clinical COPD Questionnaire. Health Qual Life Outcomes. 2003;1(1):13.
Ryan M, Gerard K. Using discrete choice experiments to value health care programmes: current practice and future research reflections. Appl Health Econ Health Policy. 2003;2(1):55–64.
Dransfield MT, Bailey W, Crater G, et al. Disease severity and symptoms among patients receiving monotherapy for COPD. Prim Care Respir J. 2011;20(1):46–53.
Kinsman RA, Yaroush RA, Fernandez E, et al. Symptoms and experiences in chronic bronchitis and emphysema. Chest. 1983;83(5):755–61.
Rutten-van Molken MP, Oostenbrink JB, Tashkin DP, et al. Does quality of life of COPD patients as measured by the generic EuroQol five-dimension questionnaire differentiate between COPD severity stages? Chest. 2006;130(4):1117–28.
Jehn M, Schindler C, Meyer A, et al. Daily walking intensity as a predictor of quality of life in patients with COPD. Med Sci Sports Exerc. 2012;44(7):1212–8.
Agusti A, Hedner J, Marin JM, et al. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(21):183–94.
Partridge MR, Karlsson N, Small IR. Patient insight into the impact of chronic obstructive pulmonary disease in the morning: an internet survey. Curr Med Res Opin. 2009;15(8):2043–8.
Nunes DM, Mota RM, de Pontes Neto OL, et al. Impaired sleep reduces quality of life in chronic obstructive pulmonary disease. Lung. 2009;187(3):159–63.
Jones PW, Agusti AG. Outcomes and markers in the assessment of chronic obstructive pulmonary disease. Eur Respir J. 2006;27(4):822–32.
Stege G, Vos PJ, van den Elshout FJ, et al. Sleep, hypnotics and chronic obstructive pulmonary disease. Respir Med. 2008;102(6):801–14.
Acknowledgments
Novartis Pharma GmbH funded the study and provided financial support for a publication for academic purposes. The authors thank Marion Schwankl for working tirelessly on the project management and for providing organizational support.
Conflicts of Interest
GP has received financial support from Novartis Pharma GmbH for study conception, travel to meetings for the study, and the preparation and review of the manuscript. GP and SF are employed by Kantar Health GmbH, which conducted the study, the analysis, and the manuscript preparation on behalf of Novartis Pharma GmbH. RS received financial support from Novartis Pharma GmbH for the literature search and manuscript preparation.
Author Contributions
GP organized the data collection. GP and SF designed the study and performed the statistical analyses. All three authors contributed to the interpretation of the data, the preparation of the manuscript, and the critical revisions of the manuscript. The guarantor for the overall content is GP.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Pisa, G., Freytag, S. & Schandry, R. Chronic Obstructive Pulmonary Disease (COPD) Patients’ Disease-Related Preferences. Patient 6, 93–101 (2013). https://doi.org/10.1007/s40271-013-0007-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-013-0007-2