
Abstract
Background and Objectives
The safety of inflammatory bowel disease medications during lactation is of significant relevance to women of childbearing potential. Available data regarding the transfer of biologic agents for inflammatory bowel disease via breast milk are limited to case reports. The objective of this prospective postmarketing lactation study was to assess vedolizumab concentrations in breast milk from lactating vedolizumab-treated women with inflammatory bowel disease.
Methods
Breast milk was serially collected throughout the dosing interval from 11 patients receiving established intravenous vedolizumab 300-mg maintenance therapy every 8, 6, or 4 weeks. Maternal safety was also assessed.
Results
Vedolizumab was detectable in ~90% of milk samples collected from all patients. Following the day 1 dose, vedolizumab milk concentrations increased with a median of 3–4 days to peak concentration, and subsequently decreased exponentially. For the nine patients receiving vedolizumab every 8 weeks, the average relative infant dose was 20.9%. Using a mean trough serum concentration of 11.2 µg/mL from historical studies, the ratio of mean vedolizumab milk-to-serum concentration was ~ 0.4 to 2.2%, consistent with published data on vedolizumab and other monoclonal antibody therapeutics for inflammatory bowel disease. The maternal safety profile was similar to that observed in previous vedolizumab studies. Published vedolizumab studies also showed no adverse findings for infants breastfed by vedolizumab-treated mothers.
Conclusions
Vedolizumab was present in human breast milk at a low level. The decision to use vedolizumab should balance the benefit of therapy to the mother and the potential risks to the infant.
Trial Registration
ClinicalTrials.gov, NCT02559713; registered 24 September, 2015.
Similar content being viewed by others


Vedolizumab was detected at a low concentration in breast milk in lactating mothers with ulcerative colitis or Crohn’s disease who received vedolizumab 300 mg every 8 weeks: the average milk concentration was approximately 0.13 µg/mL with the peak concentration up to 0.56 µg/mL; the relative infant dose was 20.9%. |
The maternal safety profile was similar to that observed in previous vedolizumab studies. |
Before initiating vedolizumab treatment, the mother’s treatment benefit should be balanced with the potential risks to the infant. |
1 Introduction
Ulcerative colitis (UC) and Crohn’s disease (CD) are chronic, idiopathic, inflammatory bowel diseases (IBDs) that peak in incidence during the reproductive years [1, 2]. Given the potential harmful effects of active IBD on pregnancy outcomes and the risk of disease flare during pregnancy and the postpartum period, female patients are counseled to continue most IBD therapy throughout this period [3, 4]. Therefore, the safety of IBD therapy during pregnancy and lactation is of significant interest, as these medications may be transferred in utero or through breast milk from nursing mothers with IBD to their newborns [5].
Monoclonal antibody (mAb) therapy, a form of biologic therapy, has become a mainstay of IBD treatment, and transport of these therapeutic molecules into breast milk has been consistently reported at a relatively low but detectable level [6,7,8,9,10]. However, the majority of available data on mAb detection in breast milk are limited to case reports and small case series in which confounding factors, such as timing of milk sample collections, whether the pharmacokinetic (PK) assay used was validated with breast milk, or differences in the therapeutic regimens of individual nursing mothers, could impact the estimation of milk concentrations.
Vedolizumab, a gut-selective, humanized IgG1 mAb directed against the human lymphocyte integrin α4β7 [11], has a well-established positive benefit-risk profile in adult patients with IBD based on extensive clinical trial data and postmarketing experience [12]. The recommended dosage in the USA for UC and CD is an intravenous (IV) 300-mg infusion at weeks 0, 2, and 6, then once every 8 weeks (Q8W) thereafter. Detectable vedolizumab in the breast milk of nursing mothers with IBD has been reported in two published studies [13, 14]. Importantly, results from up to 10 months of follow-up on breast milk-fed infants showed no increase in general or gastrointestinal infections, complication with vaccines, or developmental milestone delays.
Here, we present a controlled multicenter lactation study to determine vedolizumab concentrations in breast milk and to estimate the amount in milk relative to maternal exposure in nursing mothers with UC or CD who were receiving vedolizumab treatment. Data from published literature for vedolizumab and several other mAbs indicated for the treatment of IBD are also leveraged to facilitate the discussion and interpretation of exposure data.
2 Methods
2.1 Study Design
This was a prospective, open-label, multicenter, postmarketing milk-only study to assess concentrations of vedolizumab in the breast milk of up to 12 (minimum of ten) lactating women with active UC or CD who were at least 18 years old and were receiving established vedolizumab maintenance therapy. In accordance with the 2005 US Food and Drug Administration (FDA) draft guidance, this study was designed as a “milk-only” study and conducted between November 2017 and February 2019 across four tertiary care centers in the USA [15]. This study was initiated as a site-based enrollment study and then modified to an open-enrollment model to facilitate enrollment and provide the opportunity for eligible mothers who did not reside near one of the traditional study sites to participate in the study remotely. The study design and protocol were approved by the local ethics committee or institutional review board at each participating site, or by a central institutional review board, as applicable. All mothers provided written informed consent to participate. Importantly, the decision to treat with vedolizumab or to breastfeed was made independently from and prior to the patient consenting to participate in this study.
Eligible mothers aged 18 years or older who delivered a single normal-term infant (at least 37 weeks’ gestation) were required to be at least 5 weeks postpartum. They also had to be on established vedolizumab maintenance treatment and to have received at least one dose of 300 mg of IV vedolizumab postpartum or completed vedolizumab induction therapy (300 mg of IV vedolizumab at weeks 0, 2, and 6) before enrolling in this study. Lactation was required to be well established, with the mother exclusively breastfeeding her infant (maximum allowed: one supplemental bottle of formula/day) at the time of enrollment and continually throughout the duration of the study. The main patient exclusion criteria included: (1) maternal exposure to any investigational compound or approved biologic or biosimilar agent other than vedolizumab within 60 days prior to enrollment in the study; (2) maternal exposure to any live vaccinations within 30 days prior to vedolizumab administration; and (3) a history of breast implants, breast augmentation, or breast reduction surgery.
2.2 Study Procedures and Assessments
Study participants received 300 mg of vedolizumab via an IV infusion over approximately 30 minutes on day 1 of the study, and remained at the clinic, study site, or other healthcare provider office until after the day 1 milk PK and safety assessments were completed. Serial milk samples were collected over the dosing interval (4, 6, or 8 weeks) following vedolizumab treatment to determine the concentration of vedolizumab in breast milk and to derive the PK parameters. The prespecified time points for sample collection included predose (60 minutes before the start of infusion) and approximately 1 h after the end of infusion on day 1, as well as on days 4 (± 1), 8 (± 2), 15 (± 3), 29 (± 3), and 57 (± 3). The total volume of milk collected and the start and finish time of each collection were recorded. For milk sample collection on days 4 through 57 (days 4 through 29, prior to the next scheduled dose, for patients on once every 4 weeks [Q4W] vedolizumab therapy), study sites were encouraged to schedule the visit at approximately the same time as the day 1 post-dose sampling time to reduce the potential influence of diurnal variation. Visits after day 1 could be completed in the patient’s home setting in the presence of a qualified nurse. The study exit/follow-up safety assessment occurred on day 57 (± 3 days). The total duration on the study for each patient was approximately 3 months, including screening.
During each sample collection, milk was completely expressed from each breast using an electric milk pump provided by the study coordination center and pooled before sampling to ensure that the observed drug concentration in milk mimicked the mean drug concentration during each feeding. Two 5-mL aliquots taken from pooled milk samples at each collection time point were stored at − 70 °C until analysis. Milk concentrations of vedolizumab were measured using a validated enzyme-linked immunosorbent assay with a validated reference vedolizumab concentration range of 40 (lower limit of quantification [LLOQ]) to 4000 ng/mL.
In addition to PK assessments, maternal adverse events (AEs) and vital sign measurements were also recorded pretreatment (at screening) and from the start of vedolizumab treatment on days 1, 4 (± 1 day), 8 (± 2), 15 (± 3), 29 (± 3), and 57 (± 3)/study exit/follow-up. Vital signs (oral temperature, respiration, pulse, and blood pressure) were measured after 5 minutes supine and at the same time of the day across visits, if possible. Physical examination was performed at screening, day 1, and day 57 (±3 days)/exit/follow-up and any significant clinical change was also recorded as an AE.
2.3 Data Analysis
The primary objective of this study was to assess the concentration of vedolizumab in breast milk from lactating women with active UC or CD who were receiving IV vedolizumab therapeutically. Pharmacokinetic parameters were derived using standard non-compartmental methods based on the concentration data. Samples below the LLOQ for vedolizumab in milk were set to 0 µg/mL, and actual sample collection times were used in the parameter calculations. The concentrations of vedolizumab and derived PK parameters in milk were summarized by regimen (Q8W, once every 6 weeks [Q6W], or Q4W) over each scheduled sampling time point using descriptive statistics.
Based on the average concentration of vedolizumab (Cavg) and standardized milk consumption of a fully breastfed 2-month-old infant (150 mL/kg/day), the daily dosage of vedolizumab excreted in milk and consumed by the infant was estimated using the below equation adopted from the 2005 FDA draft guidance recommendations [15]. The average concentration was calculated from the area under the concentration–time curve over the actual dosing interval.
Subsequently, the percentage of the weight-adjusted maternal dosage consumed in breast milk over the dosing interval (identical to relative infant dose [RID] and hereinafter referred to as RID) was calculated as [16, 17]:
In addition, the ratio of vedolizumab milk concentration-to-published adult vedolizumab serum concentration from historical studies was also calculated [18, 19].
3 Results
3.1 Patients
A total of 12 patients were screened for enrollment, with one screen failure. Of the 11 enrolled patients (five with UC and six with CD), ten completed the study, and one patient missed the last study visit because of an AE. Nine of these 11 patients were receiving vedolizumab with Q8W dosing; of the remaining two, one was receiving vedolizumab Q6W and the other Q4W. The demographics and baseline characteristics of all enrolled nursing women are presented in Table 1. Most patients were white, the median age was 31 years, and the median body weight was 64 kg. Six patients had experience with breastfeeding, and no patients reported problems with producing breast milk for previously breastfed infants.
3.2 Pharmacokinetics
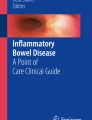
Vedolizumab was detectable in the majority of milk samples collected on days 1 and 57, and in all samples collected at other time points. The mean vedolizumab milk concentration–time profiles following IV infusion are presented in Fig. 1 by vedolizumab dosing regimen. Following IV infusion on day 1, the vedolizumab concentrations in breast milk increased over a period of 3–4 days and then decreased monoexponentially during the sampling period. Measurable vedolizumab milk concentrations were observed in predose samples (trough concentration [Ctrough] on day 1), reflecting prior vedolizumab dosing (per study design), for seven of 11 patients across all dosing regimens. The mean breast milk peak vedolizumab concentration (Cmax) was 0.252 µg/mL for patients receiving vedolizumab Q8W; the Cmax was 0.165 µg/mL for the patient receiving vedolizumab Q6W, and 0.305 µg/mL for the patient receiving vedolizumab Q4W.

Mean ± standard deviation vedolizumab milk concentrations over time by regimen following an infusion of intravenous vedolizumab at 300 mg (a: linear; b: semi-log). Frequency of dosing: Q4W every 4 weeks, Q6W every 6 weeks, Q8W every 8 weeks
Summaries of vedolizumab milk concentrations by collection day and by key vedolizumab PK parameters are presented in Tables 2 and 3, respectively, for the nine patients on the vedolizumab Q8W dosing regimen. The mean vedolizumab milk Ctrough on day 57 was 0.0471 μg/mL for the Q8W regimen, with measurable vedolizumab concentrations in milk observed on day 57 samples for six patients (for the remaining three patients, one day 57 sample was not collected, one sample was collected after subsequent dosing, and one sample was below the limit for quantification). Trough concentration data were not collected for the patient receiving vedolizumab Q6W. For the patient receiving vedolizumab Q4W, milk Ctrough on day 29 was 0.156 μg/mL (n = 1). Based on Cavg, the geometric mean daily infant dosage for Q8W regimen patients was 0.0194 mg/kg/day and the corresponding RID (geometric mean percent of the body weight-adjusted maternal dosage) was 20.9%.
In this lactation study, the range of mean Ctrough values at day 57 to mean Cmax was approximately 0.05–0.25 μg/mL. Relative to the published historical mean serum Ctrough in adult patients with IBD (11.2 μg/mL for UC and 13.0 μg/mL for CD) [18, 19], the percentage of vedolizumab concentrations in breast milk relative to maternal serum was ~ 0.4 to 2.2%.
3.3 Safety
Overall, five AEs were reported by three out of 11 mothers (27.3%). Four of these AEs (in two out of 11 patients, 18.2%) were mild in severity (flare-up of CD, motility disorder, paronychia, and viral infection), and were assessed as not related to study treatment. One of 11 patients (9.1%) experienced a serious AE of worsening UC that was assessed as related to study treatment. No patients in this study discontinued study participation because of an AE or serious AE. No deaths occurred during the study. Based upon a review of all safety data, no new or unexpected findings were observed.
4 Discussion
This study was a postmarketing lactation study in 11 lactating women with IBD receiving IV vedolizumab treatment to evaluate the transfer of vedolizumab from maternal circulation into the breast milk. Vedolizumab was detectable at a relatively low concentration in breast milk that was estimated to be ~ 0.4 to 2.2% of that in serum. This finding is comparable to the results of two independent studies evaluating vedolizumab in lactating women [13, 14]. Both studies found that the vedolizumab Cmax in breast milk was equivalent to or less than 1% of the maternal serum concentration, and that the vedolizumab serum concentrations in lactating mothers were similar to those reported in adult patients with IBD from the vedolizumab GEMINI phase III trials [18, 19]. Similar to our study (3–4 days), the Cmax of vedolizumab in breast milk was also reported at 3–5 days after dosing in most of the patients [13, 14]. In our study, serially collected samples allowed estimation of the infant dosage, which was approximately 20.9% of the body weight-adjusted maternal dosage over the duration of the dosing interval.
The majority of published lactation data from nursing mothers treated with mAbs comes from case reports and observational studies rather than controlled trials. These studies are limited by small patient numbers and short durations of milk PK samplings, and PK assays that might not be validated in human milk. All of these factors could prevent adequate estimates of the infant dosage consumed through milk for mAbs that usually have a long half-life. In contrast, our study could provide a more accurate estimate because of its controlled nature, higher number of patients (n = 11), and a validated PK assay. In addition to RID, drug concentrations in milk and serum samples and the ratio of milk-to-serum concentrations were often reported, facilitating comparison of results across studies and between mAbs. Although the measured mAb concentrations in milk were variable across different studies for the same mAb because of different sampling times, PK assays, and inclusion criteria; recent published literature has consistently shown mAbs were generally detectable at very low concentrations in human breast milk. For the anti-tumor necrosis factor mAbs infliximab and adalimumab, the milk drug concentrations were reported to be ~ 0.5 to 5% and ~ 0.1 to 1% of maternal serum concentrations, respectively, which are similar to the range estimates for vedolizumab both in our study and previous reports [6,7,8, 13, 14]. In a large prospective observational study for women with IBD treated with infliximab, adalimumab, certolizumab, and ustekinumab, peak concentration ranges in milk at around 24–48 h following drug administration were 0.15–0.74 µg/mL (n = 19), 0.45–0.71 µg/mL (n = 2), 0.27–0.29 µg/mL (n = 3), and 0.72–1.57 µg/mL (n = 4), respectively [20]. The RID reported in the literature for other biologic agents was 1.7% for natalizumab and <1% for rituximab (approved for multiple indications including certain types of cancer and rheumatoid arthritis) [21,22,23]. CRADLE (NCT02154425), which is another postmarketing milk-only lactation study with a similar overall design to the present study, showed that there was minimal to no transfer of certolizumab pegol into the breast milk of women with CD, rheumatoid arthritis, ankylosing spondylitis, axial spondyloarthritis, or psoriatic arthritis [9]. The reported RID for certolizumab was 0.15% (range 0.04–0.30) [9, 23]. This finding was consistent with the minimal placental transfer of the certolizumab pegol, likely related to its fragment crystallizable (Fc)-free molecular structure [9, 20].
During pregnancy, the mother’s placenta transports immunoglobulin G (IgG) to the fetus via a neonatal Fc receptor, and these maternal IgG antibodies protect the infant during the first 6 months after birth while its own immune system is developing [24]. After birth, IgA, secretory IgA, IgM, and IgG are absorbed by infants through human milk via the Fc receptor to also provide protection against pathogens [25]. Vedolizumab, like the majority of mAbs approved to treat IBD, is an IgG antibody. As such, the neonatal Fc receptor on human epithelial cells may similarly promote the uptake of undigested mAbs and facilitate the transfer of intact mAbs into the infant systemic circulation, especially for preterm infants with lower protein digestion capacity [9, 25]. Although the available data are very limited and inconsistent in terms of whether a drug concentration is measurable in infant serum, a certain amount of mAbs in breast milk is expected to be absorbed to the infant systemic circulation. Previous studies in adult healthy volunteers have demonstrated that low serum concentrations of vedolizumab (< 10 µg/mL) are cleared at a much faster rate than its 25.5-day half-life for concentrations >10 µg/mL, presumably attributed to target-mediated elimination via interaction with α4β7 integrin complexes and target internalization [26]. Infant serum vedolizumab concentrations are expected to be very low considering the immaturity of the infant reticuloendothelial system, the substantially lower concentration of vedolizumab in breast milk relative to maternal serum, and that only a small fraction of vedolizumab is transferred from milk to the infant systemic circulation. However, infant gastrointestinal tract maturation may impact vedolizumab degradation and infant systemic exposure.
In the present study, no new safety issues were identified, and the safety profile of vedolizumab was similar to that observed in previous studies [18, 19, 27]. Upon review of the Takeda global safety database from launch to 19 May, 2019, a total of 133 lactation reports consisting of 133 AEs were identified, with 21 of the AEs reported in infants and assessed as non-serious. The estimated postmarketing exposure of vedolizumab (as of 19 May, 2019) was 336,400 patient-years; therefore, the number of lactation-related AEs reported was consistent with exposure.
As a lactation study, challenges in patient recruitment were expected. Multiple modifications to the study design, including incorporation of an open-enrollment model, removal of certain restrictive inclusion criteria (e.g., weight restriction, need for stable doses of other UC and CD medications at study entry), and reduction of the study procedure burden on patients, were implemented without compromising the fulfillment of study objectives or introducing major confounding factors. A main limitation of this study was that neither maternal nor infant serum samples were collected to provide estimates of paired milk-to-serum ratios and aid our understanding of infant exposure to vedolizumab through breast milk. Thus, the milk to serum percentage reported represents only an estimate using the average serum concentration in adults from historical studies. Furthermore, the design of the study did not include safety follow-up of exposed infants. However, one study showed that there were no adverse findings for those infants exposed to the breast milk of their vedolizumab-treated mothers [14].
5 Conclusions
A low concentration of vedolizumab was found to be present in human breast milk from mothers who received vedolizumab treatment for IBD. These findings add to the existing literature on the exposure of suckling infants to vedolizumab through breast milk. The decision to use vedolizumab should balance the benefit of therapy to the mother and the potential risks to the infant, and the results of this study should help breastfeeding women with IBD and their physicians make informed decisions regarding their postpartum treatment.
References
Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2018;390(10114):2769–78.
Shannahan SE, Erlich JM, Peppercorn MA. Insights into the treatment of inflammatory bowel disease in pregnancy. Therap Adv Gastroenterol. 2019;12:1756284819852231.
Nguyen GC, Seow CH, Maxwell C, Huang V, Leung Y, Jones J, IBD in Pregnancy Consensus Group; Canadian Association of Gastroenterology, et al. The Toronto consensus statements for the management of inflammatory bowel disease in pregnancy. Gastroenterology. 2016;150(3):734-57.e1.
Nørgård B, Hundborg HH, Jacobsen BA, Nielsen GL, Fonager K. Disease activity in pregnant women with Crohn’s disease and birth outcomes: a regional Danish cohort study. Am J Gastroenterol. 2007;102(9):1947–54.
Nielsen OH, Maxwell C, Hendel J. IBD medications during pregnancy and lactation. Nat Rev Gastroenterol Hepatol. 2014;11(2):116–27.
Ben-Horin S, Yavzori M, Kopylov U, Picard O, Fudim E, Eliakim R, et al. Detection of infliximab in breast milk of nursing mothers with inflammatory bowel disease. J Crohns Colitis. 2011;5(6):555–8.
Fritzsche J, Pilch A, Mury D, Schaefer C, Weber-Schoendorfer C. Infliximab and adalimumab use during breastfeeding. J Clin Gastroenterol. 2012;46(8):718–9.
Ben-Horin S, Yavzori M, Katz L, Picard O, Fudim E, Chowers Y, et al. Adalimumab level in breast milk of a nursing mother. Clin Gastroenterol Hepatol. 2010;8(5):475–6.
Clowse ME, Förger F, Hwang C, Thorp J, Dolhain RJ, van Tubergen A, et al. Minimal to no transfer of certolizumab pegol into breast milk: results from CRADLE, a prospective, postmarketing, multicentre, pharmacokinetic study. Ann Rheum Dis. 2017;76(11):1890–6.
Klenske E, Osaba L, Nagore D, Rath T, Neurath MF, Atreya R. Drug levels in the maternal serum, cord blood and breast milk of a ustekinumab-treated patient with Crohn’s disease. J Crohns Colitis. 2019;13(2):267–9.
Soler D, Chapman T, Yang LL, Wyant T, Egan R, Fedyk ER. The binding specificity and selective antagonism of vedolizumab, an anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. J Pharmacol Exp Ther. 2009;330(3):864–75.
Battat R, Ma C, Jairath V, Khanna R, Feagan BG. Benefit-risk assessment of vedolizumab in the treatment of Crohn’s disease and ulcerative colitis. Drug Saf. 2019;42(5):617–32.
Julsgaard M, Kjeldsen J, Bibby BM, Brock B, Baumgart DC. Vedolizumab concentrations in the breast milk of nursing mothers with inflammatory bowel disease. Gastroenterology. 2018;154(3):752-4.e1.
Lahat A, Shitrit AB, Naftali T, Milgrom Y, Elyakim R, Goldin E, et al. Vedolizumab levels in breast milk of nursing mothers with inflammatory bowel disease. J Crohns Colitis. 2018;12(1):120–3.
US Food and Drug Administration. Guidance for industry. Clinical lactation studies: study design, data analysis, and recommendations for labeling. 2005. https://wayback.archive-it.org/7993/20170111015208/http://www.fda.gov/downloads/RegulatoryInformation/Guidances/ucm127505.pdf. Accessed 13 Nov 2020.
European Medicines Agency. Guideline on good pharmacovigilance practices (GVP). Product- or population-specific considerations III: pregnant and breastfeeding women. 2019. https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-good-pharmacovigilance-practices-product-population-specific-considerations-iii_en.pdf. Accessed 6 Nov 2020.
US Food and Drug Administration. Guidance for industry. Clinical lactation studies: considerations for study design. 2019. https://www.fda.gov/media/124749/download. Accessed 29 Oct 2020.
Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel JF, Sandborn WJ, GEMINI 1 Study Group, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699–710.
Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel JF, Sands BE, GEMINI 2 Study Group, et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med. 2013;369(8):711–21.
Matro R, Martin CF, Wolf D, Shah SA, Mahadevan U. Exposure concentrations of infants breastfed by women receiving biologic therapies for inflammatory bowel diseases and effects of breastfeeding on infections and development. Gastroenterology. 2018;155(3):696–704.
Baker TE, Cooper SD, Kessler L, Hale TW. Transfer of natalizumab into breast milk in a mother with multiple sclerosis. J Hum Lact. 2015;31(2):233–6.
Krysko KM, LaHue SC, Anderson A, Rutatangwa A, Rowles W, Schubert RD, et al. Minimal breast milk transfer of rituximab, a monoclonal antibody used in neurological conditions. Neurol Neuroimmunol Neuroinflamm. 2020;7(1):e637.
LaHue SC, Anderson A, Krysko KM, Rutatangwa A, Dorsey MJ, Hale T, et al. Transfer of monoclonal antibodies into breastmilk in neurologic and non-neurologic diseases. Neurol Neuroimmunol Neuroinflamm. 2020;7(4):e769.
Palmeira P, Quinello C, Silveira-Lessa AL, Zago CA, Carneiro-Sampaio M. IgG placental transfer in healthy and pathological pregnancies. Clin Dev Immunol. 2012;2012:985646.
Demers-Mathieu V, Underwood MA, Beverly RL, Nielsen SD, Dallas DC. Comparison of human milk immunoglobulin survival during gastric digestion between preterm and term infants. Nutrients. 2018;10(5):631.
Rosario M, Dirks NL, Gastonguay MR, Fasanmade AA, Wyant T, Parikh A, et al. Population pharmacokinetics-pharmacodynamics of vedolizumab in patients with ulcerative colitis and Crohn’s disease. Aliment Pharmacol Ther. 2015;42(2):188–202.
Sandborn WJ, Baert F, Danese S, Krznarić Z, Kobayashi T, Yao X, et al. Efficacy and safety of vedolizumab subcutaneous formulation in a randomized trial of patients with ulcerative colitis. Gastroenterology. 2020;158(3):562-72.e12.
Acknowledgements
Editorial assistance was provided by Peggy Robinet, PharmD, PhD, of ProEd Communications, Inc., and Milena Wagner, PhD, of Excel Medical Affairs, and funded by Takeda.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by Takeda.
Conflicts of Interest/Competing interest
Jingjing Chen, Sonya McKnight, Harisha Kadali, and Richard A. Lirio are Takeda employees and hold Takeda stock or stock options. Blair Fennimore has no conflicts of interest that are directly relevant to the content of this article. Dawn B. Beaulieu reports consulting fees from Takeda and AbbVie. Razvan Arsenescu reports consulting and speaker fees from Takeda. Adam C. Stein reports consulting and speaker fees from AbbVie and speaking fees from Pfizer. Tiffany Lin is contracted by Takeda via Certara. Wan Sun and Maria Rosario were Takeda employees at the time this research was conducted, and Maria Rosario reports granted patents and pending patent applications relating to the clinical pharmacology of vedolizumab.
Ethics approval
The study design and protocol were approved by the local ethics committee or institutional review board at each participating site, or by a central institutional review board, as applicable.
Consent to participate
All patients provided written informed consent to participate. The decision to treat with vedolizumab or to breastfeed was made independently from and prior to the patient consenting to participate in this study.
Consent for publication
Not applicable.
Availability of data and material
The datasets, including the redacted study protocol, redacted statistical analysis plan, and individual participants’ data supporting the results reported in this article, will be made available within 3 months from an initial request, to researchers who provide a methodologically sound proposal. The data will be provided after its de-identification, in compliance with applicable privacy laws, data protection, and requirements for consent and anonymization.
Code availability
Not applicable.
Authors’ contributions
WS, JC, TL, SM, MR, and RAL contributed to the study concept and design. BF, DBB, RA, ACS, and SM participated in the data acquisition. WS, BF, DBB, RA, ACS, JC, TL, HK, MR, and RAL provided the data analysis and interpretation. All authors had access to the data and participated in drafting and revising the manuscript. All authors approved the final draft for submission.
Additional information
Wan Sun and Maria Rosario were employees of Takeda at the time of this research.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sun, W., Fennimore, B., Beaulieu, D.B. et al. Vedolizumab Concentrations in Breast Milk: Results from a Prospective, Postmarketing, Milk-Only Lactation Study in Nursing Mothers with Inflammatory Bowel Disease. Clin Pharmacokinet 60, 811–818 (2021). https://doi.org/10.1007/s40262-021-00985-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-021-00985-4