
Abstract
Background and Objective
Tolvaptan, an oral vasopressin V2 receptor antagonist, has been widely used for the treatment of patients with cirrhosis and ascites. However, its efficacy in patients with renal dysfunction remains unknown. The objective of this study was to investigate the efficacy and safety of tolvaptan in patients with decompensated cirrhosis and severe chronic kidney disease (s-CKD).
Methods
We studied 43 patients with liver cirrhosis who received tolvaptan (7.5 mg/day) for refractory ascites. s-CKD was defined as an estimated glomerular filtration rate (eGFR) < 45 mL/min/1.73 m2. Response to tolvaptan was defined as weight loss ≥ 1.5 kg in 7 days of treatment.
Results
Eighteen patients (42%) had s-CKD (s-CKD group), while the other 25 patients (58%) did not have s-CKD (n-CKD group). Rates of response to tolvaptan were similar: 68% in the n-CKD group and 56% in the s-CKD group. Urine volumes increased significantly from baseline to day 7 in both groups. Incidences of adverse events were also similar (P = 0.93). Mean eGFR did not decline even in the s-CKD group (27.3 ± 2.2 mL/min/1.73 m2 at baseline vs. 26.6 ± 2.3 mL/min/1.73 m2 on day 7; P = 0.9). The cumulative survival rate did not differ significantly between the n-CKD and s-CKD groups. In the s-CKD group, responders obtained a better prognosis than non-responders.
Conclusions
Tolvaptan significantly increased urine volumes similarly in patients with s-CKD and n-CKD without affecting renal function. As responders achieved a better prognosis, tolvaptan could be a good option to treat ascites in patients with cirrhosis and s-CKD.
Similar content being viewed by others

In this study, we showed that tolvaptan was effective and safe in patients with decompensated cirrhosis and chronic kidney disease. |
Since tolvaptan had a protective effect on the kidneys, it could be a good choice in ascitic patients complicated by renal dysfunction. |
1 Introduction
Hepatic factors, renal factors, and systemic circulatory dynamics are involved in the progression of ascites in patients with liver cirrhosis. In liver cirrhosis, peripheral vasodilation and arteriovenous anastomosis in various organs occur via increased nitric oxide production, resulting in a hyperdynamic state. In addition, as fluids leak into the third space due to hypoalbuminemia, the effective circulatory volume and renal blood flow decrease, leading to activation of the renin–angiotensin–aldosterone system (RAAS). The activated RAAS enhances reabsorption of sodium and water in proximal renal tubules, which further deteriorates water retention. The decrease in renal blood flow also promotes secretion of arginine vasopressin (AVP), which controls free water clearance and enhances reabsorption of free water in renal collecting ducts. Consequently, ascites occurs [1, 2]. Diuretics such as furosemide cause renal dysfunction by decreasing renal blood flow and further activating the RAAS [3]. Progression of renal dysfunction in patients with liver cirrhosis is associated with increased mortality [4].
In Japan, tolvaptan, an oral vasopressin V2 receptor antagonist that reduces water reabsorption in renal collecting ducts, was approved in September 2013 for the treatment of patients with cirrhosis and refractory ascites [5]. The 2015 Japanese “Evidence-based Clinical Practice Guidelines for Liver Cirrhosis 2015” recommends the use of tolvaptan for the treatment of ascites (evidence level A) [6]. Unlike furosemide, the action of tolvaptan is not influenced by serum albumin levels [7]. Tolvaptan does not activate RAAS and increases urine volume without affecting renal blood flow [8]. In addition, it does not reduce the estimated glomerular filtration rate (eGFR) in patients with heart failure and severe renal impairment [9]. However, as cases with a serum creatinine (SCr) level > 2.0 mg/dL were excluded in the Japanese phase III placebo-controlled study for patients with cirrhosis and ascites [5], the effectiveness of tolvaptan in those with decompensated liver cirrhosis and severe chronic kidney disease (s-CKD) remains unknown.
Therefore, in this study, we investigated the efficacy and safety of tolvaptan in the treatment of patients with cirrhosis and s-CKD and also analyzed the factors associated with response to the drug.
2 Methods
2.1 Study Design and Patient Population
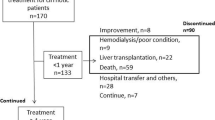
We retrospectively studied 43 consecutive patients with liver cirrhosis who received tolvaptan (7.5 mg/day) for refractory ascites between September 2013 and March 2015 at Tokai University Hospital. We enrolled patients whose ascites had been poorly controlled even with furosemide (≥ 20 mg/day) and spironolactone (≥ 25 mg/day). Patients with spontaneous bacterial peritonitis or hepatic encephalopathy (coma scale score ≥ II) and those who had received intravenous albumin within 7 days prior to tolvaptan administration were excluded from the study. Hepatocellular carcinoma (HCC) was classified by TNM (tumor, node, metastasis) staging according to the staging system of the Liver Cancer Study Group of Japan [10], and was treated based on the treatment guideline from this group [11]. Tolvaptan treatment was initiated at a dose of 7.5 mg/day upon hospitalization. Patients continued to take the same doses of furosemide and spironolactone during tolvaptan therapy. This study was approved by the Institutional Review Board for Clinical Research at Tokai University (no. 16R-242) and was conducted in accordance with the Helsinki Declaration.
2.2 Evaluation of Treatment Response and Renal Function
After oral administration of tolvaptan, the amount of fluid intake, urine volume and body weight were measured each day. Laboratory and urinary analyses were performed on days 1, 4, and 7. Urinary osmolality was also measured 4 h after the initial tolvaptan administration.
Response to tolvaptan was defined as weight loss ≥ 1.5 kg on day 7 from baseline [12]. Renal function was evaluated based on eGFR [13], and classification of CKD was according to Kidney Disease Improving Global Outcome (KDIGO) criteria [14]. s-CKD was defined as eGFR < 45 mL/min/1.73 m2 (CKD stages G3b, G4, and G5), while non-s-CKD (n-CKD) was defined as CKD stages G1, G2, and G3a. We also evaluated renal function using criteria proposed by the Acute Dialysis Quality Initiative and the International Ascites Club (IAC) Working Group (ADQI-IAC criteria) [15], which is often used for cirrhotic patients. CKD based on ADQI-IAC criteria was defined as a glomerular filtration rate of < 60 mL/min for > 3 months calculated using the Modification of Diet in Renal Disease formula. Acute kidney injury (AKI) was defined as an increase in SCr level ≥ 0.3 mg/dL or ≥ 50% from baseline in < 48 h. Patients with hepatorenal syndrome (HRS) were diagnosed according to the IAC guidelines [16]. Changes in body weight, urine volume, and eGFR were compared between patients with and without CKD.
2.3 Follow-Up and Assessment of Safety and Prognosis
After discharge from the hospital, patients were required to visit the outpatient clinic every 1 or 2 months, and body weight, clinical symptoms, and laboratory data were recorded. Adverse events were also recorded on each visit. The severity of adverse events was assessed according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. Patients were followed up until death or 31 January 2018.
2.4 Statistical Analysis
Continuous and categorical variables were compared between patients with s-CKD and n-CKD using the Mann–Whitney U test and chi-square test, respectively. Changes in body weight, urine volume, and eGFR in each group were compared using the paired t test with Bonferroni correction. Uni- and multivariate logistic regression analyses were performed to identify the factors associated with response to tolvaptan, and a receiver operating characteristic (ROC) curve was created to obtain the best cutoff value of these factors. The log-rank test using the Kaplan–Meier method was adopted to compare cumulative survival rates.
All analyses were performed using SPSS® version 24 (SPSS Japan, Tokyo, Japan), and P values < 0.05 were considered statistically significant.
3 Results
3.1 Clinical Characteristics
Clinical characteristics of the 43 patients are shown in Table 1. There were 27 men (62.8%) and 16 women (37.2%) with a median age of 68 years (range 39–84 years). Median doses of furosemide and spironolactone before tolvaptan therapy were 40 mg (range 20–120 mg) and 50 mg (range 25–100 mg), respectively. Hepatitis C virus was the most common etiology of liver cirrhosis, and nine patients (20.9%) had HCC (five patients with stage III and four patients with stage IV).
Of the 43 patients, 25 (58%; G1, three; G2, seven; G3a, 15) and 18 (42%; G3b, nine; G4, seven; G5, two) were categorized to the n-CKD and s-CKD groups, respectively. The proportions of patients with HCC and Child–Pugh C were similar between the n-CKD and s-CKD groups: 16.0% and 56.0% in the n-CKD group versus 27.8% and 50.0% in the s-CKD group, respectively. There were more patients with type 2 diabetes mellitus in the s-CKD than n-CKD groups: 12.0% in the n-CKD group and 50.0% in the s-CKD group (P = 0.007). Proteinuria in the spot urine test was detected more often in the s-CKD than in the n-CKD groups. SCr, blood urea nitrogen (BUN), and serum potassium were higher in the s-CKD than in the n-CKD groups. There were no differences in age, sex, body weight, etiology of liver cirrhosis, dose of diuretics (furosemide, spironolactone), proportions of patients receiving branched-chain amino acid (BCAA) supplementation, clinical stage of HCC, urine osmolality, and liver function (serum albumin, prothrombin time, total bilirubin) at the beginning of tolvaptan between the n-CKD and s-CKD groups.
According to the ADQI-IAC criteria, 28 (65.1%) patients had CKD (ADQI-IAC-CKD), and the remaining 15 (34.9%) did not have CKD (non-ADQI-IAC-CKD). Most of the ADQI-IAC-CKD patients were overlapped with the s-CKD patients and their baseline characteristics were similar (data not shown).
3.2 Efficacy of Tolvaptan
The mean ± standard error (SE) change in body weight from baseline to day 7 was − 2.0 ± 0.4 kg (range − 7.1 to + 4.8 kg; Fig. 1). A total of 27 patients (62.8%) had lost ≥ 1.5 kg on day 7; these patients were judged as responders. The other 16 patients (37.2%) were classified as non-responders. Mean ± SE change in body weight from baseline to day 7 was not significantly different between the n-CKD and s-CKD groups (− 2.2 ± 0.4 vs. − 1.8 ± 0.8 kg; P = 0.596; Fig. 1). Urine volume increased significantly from baseline to days 1, 3, and 7 in both groups (Fig. 2). The mean ± SE urine volumes in the s-CKD group were as follows: baseline, 766 ± 62 mL; day 1, 1416 ± 204 mL (P = 0.011); day 3, 1528 ± 256 mL (P = 0.022); and day 7, 1723 ± 252 mL (P = 0.004). Rates of response to tolvaptan were similar: 68% in the n-CKD group and 55.6% in the s-CKD group (P = 0.79). The incidence of re-exacerbation events such as hospitalization for intravenous administration of diuretics and albumin, ascites drainage, peritoneal–venous shunt, and cell-free and concentrated ascites reinfusion therapy (CART) was similar; 68.0% (17/25) in the n-CKD group and 61.1% (11/18) in the s-CKD group (P = 0.644). The period until re-exacerbation did not differ significantly: median of 175 days in the n-CKD group and 106 days in the s-CKD group (P = 0.367).

Changes in body weight in the n-CKD and s-CKD groups. Data are shown as mean ± standard error. The n-CKD and s-CKD groups were defined as patients with liver cirrhosis and n-CKD (eGFR ≥ 45 mL/min/1.73 m2) and those with liver cirrhosis and s-CKD (eGFR < 45 mL/min/1.73 m2), respectively. eGFR estimated glomerular filtration rate, n-CKD non-severe chronic kidney disease, s-CKD severe chronic kidney disease

Changes in urine volume in the n-CKD and s-CKD groups. Data are shown as mean ± standard error. The n-CKD and s-CKD groups were defined as patients with liver cirrhosis and n-CKD (eGFR ≥ 45 mL/min/1.73 m2) and those with liver cirrhosis and s-CKD (eGFR < 45 mL/min/1.73 m2), respectively. *P < 0.01 vs. baseline. eGFR estimated glomerular filtration rate, n-CKD non-severe chronic kidney disease, s-CKD severe chronic kidney disease
We also compared the response to tolvaptan based on the ADQI-IAC criteria. The mean ± SE change in body weight from baseline to day 7 was not significantly different between the non-ADQI-IAC-CKD and ADQI-IAC-CKD groups (− 2.3 ± 0.4 vs. − 1.8 ± 0.6 kg; P = 0.503). The response rate to tolvaptan was 60.0% (9/15) and 64.3% (18/28) in the non-ADQI-IAC-CKD and ADQI-IAC-CKD groups, respectively, showing no significant difference (P = 0.788). HRS type 2 was observed in six patients, of whom four (66.7%) were considered tolvaptan responders.
3.3 Predictors of Response to Tolvaptan
We assessed the variables associated with response to tolvaptan. The proportion of patients with HCC was significantly greater in non-responders than in responders (37.5% vs. 11.1%; P = 0.014). The numbers of stage I, II, III, and IV patients were zero, zero, one, and two, respectively, in responders, and zero, zero, four, and two, respectively, in non-responders (P = 0.093). As a previous treatment for HCC, two responders and three non-responders received radiofrequency ablation (P = 0.344) and three responders and six non-responders underwent super-selective transarterial chemoembolization (P = 0.058). The proportion of clinical stage of HCC and patients who had previous treatment did not differ significantly between responders and non-responders. The baseline serum sodium level was significantly higher in responders than in non-responders (138.0 vs. 133.0 mEq/L; P = 0.027). Although baseline urinary osmolality was not significantly different (429.0 vs. 378.0 mOsm/L; P = 0.456), the rate of decrease in urinary osmolality 4 h after tolvaptan administration was significantly greater in responders than in non-responders (44.6% vs. 16.1%; P = 0.008). The rate of decrease in urinary osmolality in 7 days was also significantly greater in responders than in non-responders (33.9% vs. 21.4%; P = 0.029). Baseline variables associated with renal function, such as SCr, BUN, eGFR, and CKD stage, were not significantly different between responders and non-responders. The proportion of patients receiving BCAA supplementation did not differ between responders and non-responders (66.7% vs. 75.0%; P = 0.57). Multivariate analysis revealed that two variables were significant independent predictors of response to tolvaptan: serum sodium level (odds ratio [OR] 1.179; 95% confidence interval [CI] 1.017–1.367; P = 0.029) and rate of decrease in urinary osmolality after 4 h (OR 1.077; 95% CI 1.023–1.134; P = 0.005; Table 2). The area under the concentration–time curve (AUC) and best cut-off value were 0.719 and 134.0 mEq/L, respectively, for serum sodium level, and 0.773% and 37.8%, respectively, for rate of decrease in urinary osmolality after 4 h.
3.4 Safety
Adverse events occurring during tolvaptan treatment were as follows: thirst, seven (16.3%); fatigue, three (7%); muscle cramps, one (2.3%); hypernatremia (> 145 mEq/L), one (2.3%); hepatic encephalopathy, one (2.3%); and variceal bleeding, one (2.3%). Incidences of adverse events were similar: 32% in the n-CKD group and 33.3% in the s-CKD group (P = 0.93; Table 3). Thirst, fatigue, muscle cramps, and hypernatremia were judged as grade 1–2, and hepatic encephalopathy and variceal bleeding were judged as grade 3. Tolvaptan did not affect eGFR even in the s-CKD group (27.3 ± 2.2 mL/min/1.73 m2 at baseline vs. 26.6 ± 2.3 mL/min/1.73 m2 on day 7; P = 0.9; Fig. 3).

Changes in eGFR in the n-CKD and s-CKD groups. Data are shown as mean ± standard error. The n-CKD and s-CKD groups were defined as patients with liver cirrhosis and n-CKD (eGFR ≥ 45 mL/min/1.73 m2) and those with liver cirrhosis and s-CKD (eGFR < 45 mL/min/1.73 m2), respectively. eGFR estimated glomerular filtration rate, n-CKD non-severe chronic kidney disease, s-CKD severe chronic kidney disease
3.5 Effect of Tolvaptan on Survival
During a median follow-up of 374 days, 30 patients (69.8%) died. Most of the causes of death were liver-related; 21 patients died of liver failure and six patients died of HCC. The cumulative survival rate was significantly higher in responders than in non-responders (P < 0.001; Fig. 4a). However, the cumulative survival rate did not differ significantly between the n-CKD and s-CKD groups (P = 0.503; Fig. 4b). In the s-CKD group, responders obtained a better prognosis than non-responders with regard to survival in 90 and 180 days: 90% and 70% in responders versus 50% and 13% in non-responders, respectively (P = 0.006; Fig. 4c). We summarized the baseline characteristics of the four groups classified by renal function and response to tolvaptan (Electronic Supplementary Material Table). The baseline serum sodium level was significantly higher in the n-CKD/responders group than in the n-CKD/non-responders group (138.0 vs. 131.0 mEq/L; P < 0.001). In the s-CKD group, more non-responders had HCC, but the difference was not significant (P = 0.082). Other variables including BCAA supplementation did not differ significantly. In the analysis of non-ADQI-IAC-CKD and ADQI-IAC-CKD patients, similar results were obtained; the cumulative survival rate did not differ significantly between these two groups, and responders obtained a better prognosis than non-responders in the ADQI-IAC-CKD group (data not shown).

Cumulative survival rates in patients with liver cirrhosis and ascites treated with tolvaptan. The log-rank test using the Kaplan–Meier method was adopted to compare cumulative survival rates between responders and non-responders (a); between the n-CKD and s-CKD group (b); and based on renal function (n-CKD or s-CKD) and response to tolvaptan (responders or non-responders) (c). The n-CKD and s-CKD groups were defined as patients with liver cirrhosis and n-CKD (eGFR ≥ 45 mL/min/1.73 m2) and those with liver cirrhosis and s-CKD (eGFR < 45 mL/min/1.73 m2), respectively. eGFR estimated glomerular filtration rate, n-CKD non-severe chronic kidney disease, s-CKD severe chronic kidney disease
4 Discussion
Patients with liver cirrhosis often have renal impairment. Renal impairment is a poor prognostic factor [17], and use of diuretics for fluid retention may further worsen renal function. Previously, the effectiveness of tolvaptan in patients with s-CKD has been unknown. In this study, we showed that tolvaptan effectively increased urine volume in ascitic patients with s-CKD without affecting renal function, with similar results in those with normal or mildly impaired renal function.
Unlike conventional diuretics, tolvaptan acts from the vascular side of the collecting ducts in the kidney, and its effect is not influenced by reduced glomerular filtration volume [18]. It was previously reported that tolvaptan increased urine volume in patients with chronic heart failure and s-CKD without reducing renal blood flow and eGFR [8, 9]. Conventional diuretics, such as loop diuretics, are apt to induce renal dysfunction, hepatic encephalopathy, and hyponatremia [19]. In decompensated cirrhosis with ascites, AKI may be induced by an increase in diuretic dose [20]. Repeated AKI gradually shifts to CKD, subsequently resulting in poor prognosis [21]. Therefore, avoiding AKI is critically important in the treatment of patients with cirrhosis and ascites. In this study, we demonstrated that tolvaptan was effective and safe in patients with ascites irrespective of renal function. We propose that tolvaptan should be used before renal function is impaired by prolonged and escalating doses of conventional diuretics. In addition, loop diuretics impair skeletal myoblast differentiation and exercise-induced muscle hypertrophy [22]. Hanai et al. [23] recently showed that use of a higher dose of loop diuretics resulted in more rapid decrease of skeletal muscle mass and lower survival rate in patients with liver cirrhosis independent of severity of liver disease, suggesting the association of loop diuretics use with development of sarcopenia. Therefore, adding tolvaptan rather than increasing the dose of loop diuretics should be considered from the viewpoint of preventing sarcopenia progression.
Previously, several factors were reported as predictive of tolvaptan effectiveness in patients with liver cirrhosis. However, discussing the results is difficult because these studies adopted different definitions of response to tolvaptan. Recently, the Japanese Society of Gastroenterology proposed weight loss ≥ 1.5 kg/week as a definition of response to tolvaptan [12]. Using this criterion, we found that the serum sodium level and rate of decrease in urinary osmolality after 4 h were significant predictive factors for tolvaptan efficacy. Hyponatremia is associated with increased risk of mortality [24, 25] and occurrence of complications, such as hepatic encephalopathy, HRS, and spontaneous bacterial peritonitis, in patients with cirrhosis [26]. In this study, 30% of patients had hyponatremia (< 135 mEq/L) at baseline and those patients were less likely to respond to tolvaptan. Because hyponatremia is associated with unresponsiveness to tolvaptan as well as deterioration of liver disease, tolvaptan should be started before progression of hyponatremia. The rate of decrease in urinary osmolality after 4 h was another significant factor associated with tolvaptan effectiveness, which was reported in a previous study [27]. Urinary osmotic pressure reflects the osmotic pressure of the renal interstitium. Tolvaptan suppresses urea uptake from collecting ducts to the interstitium by the urea transporter via vasopressin V2 receptor inhibition, and decreases the interstitial osmotic pressure, leading to suppression of water reabsorption [18]. Thus, the reduction in urinary osmotic pressure indicates the effect of tolvaptan. Baseline urinary osmolality > 352 mOsm/L and rate of decrease in urinary osmolality > 26% at 4–6 h after tolvaptan administration were reported as significant predictors of good response in patients with decompensated heart failure [28]. Baseline urinary osmolality was not a predictor in our patients with liver cirrhosis, and the best cutoff value for the rate of decrease in urinary osmolality after 4 h was 37.8%. These differences may be derived from the differences in background diseases (i.e., heart failure vs. liver cirrhosis) and concomitantly administered diuretics.
Renal function has attracted attention as a factor related to tolvaptan efficacy. Although reports have indicated that serum BUN or SCr is related to efficacy [29,30,31,32], other reports stated that they could not be used as predictors [33,34,35,36], showing that there is no consensus. SCr levels may decline along with the decrease in skeletal muscle mass, which often occurs in liver cirrhosis. Thus, creatinine levels do not accurately reflect renal function in cirrhotic patients [37]. Moreover, as serum BUN levels increase due to liver dysfunction and malnutrition, they are not appropriate as a biomarker for renal function in liver cirrhosis [38].
We also performed an analysis using the ADQI-IAC criteria that were recently proposed for renal evaluation in liver cirrhosis [13]. Results were similar to those obtained using the KDIGO criteria. In other words, tolvaptan efficacy was sustained in cirrhotic patients with and without CKD according to ADQI-IAC criteria. In addition, tolvaptan showed 66.7% (4/6) efficacy even in patients with HRS type 2. These results were in agreement with the study of Zhang et al. [39]; according to their report, all of the seven ascitic patients complicated by HRS type 2 responded to tolvaptan with a urine volume increase to ≥ 500 mL/24 h and a decrease in waist circumference as well, whereas two HRS type 1 patients showed no improvement. Our study did not include any HRS type 1 cases.
As shown in Table 1, the type 2 diabetes was more common in the s-CKD group. Moreover, many patients with s-CKD revealed proteinuria in the spot urine test, demonstrating the presence of diabetic nephropathy. Several reports state that tolvaptan is effective against diabetic nephropathy associated with fluid retention in CKD patients [40,41,42]. Tolvaptan acts on the collecting ducts, which are relatively preserved in ischemic renal diseases caused by diabetes, so the effects of tolvaptan are readily demonstrated.
In this study, we demonstrated that responders had better survival than non-responders, similar to previous studies [31, 32, 43]. Notably, this observation was true even for the patients with s-CKD. Furthermore, the prognosis of s-CKD patients was not poorer than that of n-CKD patients, an observation that is discordant with a previous study demonstrating that the prognosis of liver cirrhosis complicated by renal dysfunction was poor [44]. However, a couple of studies showed that baseline renal function was not associated with the prognosis of patients who were treated with tolvaptan [32, 45]. Treatment with this drug may lead to the dose reduction of other diuretic drugs such as furosemide and, consequently, prolong life expectancy via maintaining renal function in cirrhotic patients [46]. Furthermore, tolvaptan itself has a renoprotective action through improving kidney congestion [18, 47]. Therefore, tolvaptan may have an even better effect on patients with impaired renal function. This topic needs further investigation.
This study has some limitations: first, the number of patients was too small to confirm our conclusion. Second, this study is retrospective, and hence a selection bias may not be totally excluded. Therefore, further larger-scale prospective studies are needed to confirm our results.
5 Conclusion
In our study, we showed that tolvaptan significantly increased urine volume similarly in patients with s-CKD and with those without s-CKD without affecting renal function. As responders achieved a better prognosis, tolvaptan could be a good option for treating refractory ascites in patients with cirrhosis and s-CKD. These results warrant a large-scale prospective study.
References
Ginès P, Cárdenas A, Arroyo V, Rodés J. Management of cirrhosis and ascites. N Engl J Med. 2004;350:1646–54.
Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology. 1988;8:1151–7.
Kim WR, Biggins SW, Kremers WK, Wiesner RH, Kamath PS, Benson JT, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359:1018–26.
Montoliu S, Ballesté B, Planas R, Alvarez MA, Rivera M, Miquel M, et al. Incidence and prognosis of different types of functional renal failure in cirrhotic patients with ascites. Clin Gastroenterol Hepatol. 2010;8:616–22.
Sakaida I, Kawazoe S, Kajimura K, Saito T, Okuse C, Takaguchi K, et al. Tolvaptan for improvement of hepatic edema: a phase 3, multicenter, randomized, double-blind, placebo-controlled trial. Hepatol Res. 2014;44:73–82.
Fukui H, Saito H, Ueno Y, Uto H, Obara K, Sakaida I, et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J Gastroenterol. 2016;51:629–50.
Sakaida I, Nakajima K, Okita K, Hori M, Izumi T, Sakurai M, et al. Can serum albumin level affect the pharmacological action of tolvaptan in patients with liver cirrhosis? A post hoc analysis of previous clinical trials in Japan. J Gastroenterol. 2015;50:1047–53.
Costello-Boerrigter LC, Smith WB, Boerrigter G, Ouyang J, Zimmer CA, Orlandi C, et al. Vasopressin2-receptor antagonism augments water excretion without changes in renal hemodynamics or sodium and potassium excretion in human heart failure. Am J Physiol Ren Physiol. 2006;290:F273–8.
Otsuka T, Sakai Y, Ohno D, Murasawa T, Sato N, Tsuruoka S. The effects of tolvaptan on patients with severe chronic kidney disease complicated by congestive heart failure. Clin Exp Nephrol. 2013;17:834–8.
Minagawa M, Ikai I, Matsuyama Y, Yamaoka Y, Makuuchi M. Staging of hepatocellular carcinoma: assessment of the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772 patients in Japan. Ann Surg. 2007;245:909–22.
Kokudo N, Hasegawa K, Akahane M, Igaki H, Izumi N, Ichida T, et al. Evidence-based clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2013 update (3rd JSH-HCC guidelines). Hepatol Res. 2015;45:123–7.
Hiramine Y, Uojima H, Nakanishi H, Hiramatsu A, Iwamoto T, Kimura M, et al. Response criteria of tolvaptan for the treatment of hepatic edema. J Gastroenterol. 2018;53:258–68.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150.
Wong F, Nadim MK, Kellum JA, Salerno F, Bellomo R, Gerbes A, et al. Working party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut. 2011;60:702–9.
Salerno F, Gerbes A, Ginès P, Wong F, Arroyo V. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Gut. 2007;56:1310–8.
Fede G, D’Amico G, Arvaniti V, Tsochatzis E, Germani G, Georgiadis D, et al. Renal failure and cirrhosis: a systematic review of mortality and prognosis. J Hepatol. 2012;56:810–8.
Mori T, Ohsaki Y, Oba-Yabana I, Ito S. Diuretic usage for protection against end-organ damage in liver cirrhosis and heart failure. Hepatol Res. 2017;47:11–22.
Arroyo V, Colmenero J. Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management. J Hepatol. 2003;38:S69–89.
Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut. 2013;62:131–7.
Sharma A, Mucino MJ, Ronco C. Renal functional reserve and renal recovery after acute kidney injury. Nephron Clin Pract. 2014;127:94–100.
Mandai S, Furukawa S, Kodaka M, Hata Y, Mori T, Nomura N, et al. Loop diuretics affect skeletal myoblast differentiation and exercise-induced muscle hypertrophy. Sci Rep. 2017;7:46369.
Hanai T, Shiraki M, Miwa T, Watanabe S, Imai K, Suetsugu A, et al. Effect of loop diuretics on skeletal muscle depletion in patients with liver cirrhosis. Hepatol Res. 2018. https://doi.org/10.1111/hepr.13244 (Epub 2018 Aug 29).
Goh KP. Management of hyponatremia. Am Fam Physician. 2004;69:2387–94.
Planas R, Montoliu S, Ballesté B, Rivera M, Miquel M, Masnou H, et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clin Gastroenterol Hepatol. 2006;4:1385–94.
Angeli P, Wong F, Watson H, Gines P, Investigators CAPPS. Hyponatremia in cirrhosis: results of a patient population survey. Hepatology. 2006;44:1535–42.
Iwamoto T, Maeda M, Hisanaga T, Saeki I, Fujisawa K, Matsumoto T, et al. Predictors of the effect of tolvaptan on the prognosis of cirrhosis. Intern Med. 2016;55:2911–6.
Imamura T, Kinugawa K, Shiga T, Kato N, Muraoka H, Minatsuki S, et al. Novel criteria of urine osmolality effectively predict response to tolvaptan in decompensated heart failure patients—association between non-responders and chronic kidney disease. Circ J. 2013;77:397–404.
Hiramine Y, Uto H, Imamura Y, Hiwaki T, Kure T, Ijuin S, et al. Efficacy of vasopressin V2 receptor antagonist tolvaptan in treatment of hepatic edema. Hepatol Res. 2017;47:542–57.
Kawaratani H, Fukui H, Moriya K, Noguchi R, Namisaki T, Uejima M, et al. Predictive parameter of tolvaptan effectiveness in cirrhotic ascites. Hepatol Res. 2017;47:854–61.
Kogiso T, Yamamoto K, Kobayashi M, Ikarashi Y, Kodama K, Taniai M, et al. Response to tolvaptan and its effect on prognosis in cirrhotic patients with ascites. Hepatol Res. 2017;47:835–44.
Atsukawa M, Tsubota A, Kato K, Abe H, Shimada N, Asano T, et al. Analysis of factors predicting the response to tolvaptan in patients with liver cirrhosis and hepatic edema. J Gastroenterol Hepatol. 2018;33:1256–63.
Ohki T, Sato K, Yamada T, Yamagami M, Ito D, Kawaishi K, et al. Efficacy of tolvaptan in patients with refractory ascites in a clinical setting. World J Hepatol. 2015;7:1685–893.
Nakagawa A, Atsukawa M, Tsubota A, Kondo C, Okubo T, Arai T, et al. Usefulness of portal vein pressure for predicting the effects of tolvaptan in cirrhotic patients. World J Gastroenterol. 2016;22:5104–13.
Komiyama Y, Kurosaki M, Nakanishi H, Takahashi Y, Itakura J, Yasui Y, et al. Prediction of diuretic response to tolvaptan by a simple, readily available spot urine Na/K ratio. PLoS One. 2017;12:e0174649.
Uojima H, Kinbara T, Hidaka H, Sung JH, Ichida M, Tokoro S, et al. Close correlation between urinary sodium excretion and response to tolvaptan in liver cirrhosis patients with ascites. Hepatol Res. 2017;47:E14–21.
Sherman DS, Fish DN, Teitelbaum I. Assessing renal function in cirrhotic patients: problems and pitfalls. Am J Kidney Dis. 2003;41:269–78.
Francoz C, Nadim MK, Durand F. Kidney biomarkers in cirrhosis. J Hepatol. 2016;65:809–24.
Zhang X, Wang SZ, Zheng JF, Zhao WM, Li P, Fan CL, et al. Clinical efficacy of tolvaptan for treatment of refractory ascites in liver cirrhosis patients. World J Gastroenterol. 2014;20:11400–5.
Shimizu M, Ishikawa S, Yachi Y, Muraoka M, Tasaki Y, Iwasaki H, et al. Tolvaptan therapy for massive edema in a patient with nephrotic syndrome. Pediatr Nephrol. 2014;29:915–7.
Sato E, Nakamura T, Amaha M, Nomura M, Matsumura D, Yamagishi H, et al. Effect of tolvaptan in patients with chronic kidney disease due to diabetic nephropathy with heart failure. Int Heart J. 2014;55:533–8.
Takada T, Masaki T, Hoshiyama A, Toki T, Kamata Y, Shichiri M. Tolvaptan alleviates excessive fluid retention of nephrotic diabetic renal failure unresponsive to furosemide. Nephrology (Carlton). 2018;23(9):883–6. https://doi.org/10.1111/nep.13390.
Yamada T, Ohki T, Hayata Y, Karasawa Y, Kawamura S, Ito D, et al. Potential effectiveness of tolvaptan to improve ascites unresponsive to standard diuretics and overall survival in patients with decompensated liver cirrhosis. Clin Drug Investig. 2016;36:829–35.
Llach J, Ginès P, Arroyo V, Rimola A, Titó L, Badalamenti S, et al. Prognostic value of arterial pressure, endogenous vasoactive systems, and renal function in cirrhotic patients admitted to the hospital for the treatment of ascites. Gastroenterology. 1988;94:482–7.
Tahara T, Mori K, Mochizuki M, Ishiyama R, Noda M, Hoshi H, et al. Tolvaptan is effective in treating patients with refractory ascites due to cirrhosis. Biomed Rep. 2017;7:558–62.
Tajiri K, Tokimitsu Y, Ito H, Atarashi Y, Kawai K, Minemura M, et al. Survival benefit of tolvaptan for refractory ascites in patients with advanced cirrhosis. Dig Dis. 2018;36:314–21.
Kimura K, Momose T, Hasegawa T, Morita T, Misawa T, Motoki H, et al. Early administration of tolvaptan preserves renal function in elderly patients with acute decompensated heart failure. J Cardiol. 2016;67:399–405.
Acknowledgements
We would like to thank Editage for English language editing.
Author information
Authors and Affiliations
Contributions
YA planned this study’s content, collected patients’ data, performed statistical analysis, and wrote the manuscript. TK participated in the design of the study and helped to write the manuscript. KT, HS, ET, KA, SH, RD, KS, and TM participated in the collection of patients’ data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Funding
This study had no sources of funding.
Conflict of Interest
Yoshitaka Arase, Tatehiro Kagawa, Kota Tsuruya, Hirohiko Sato, Erika Teramura, Kazuya Anzai, Shunji Hirose, Ryuzo Deguchi, Koichi Shiraishi, and Tetsuya Mine declare that they have no conflict of interest.
Data availability
All data generated or analyzed during this study are included in this published article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board for Clinical Research at Tokai University (no. 16R-242).
Informed consent
As this was a retrospective study, formal consent was not required.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Arase, Y., Kagawa, T., Tsuruya, K. et al. Impaired Renal Function May Not Negate the Efficacy of Tolvaptan in the Treatment of Cirrhotic Patients with Refractory Ascites. Clin Drug Investig 39, 45–54 (2019). https://doi.org/10.1007/s40261-018-0714-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-018-0714-5