
Abstract
Introduction
Alglucosidase alfa received marketing approval for the treatment of Pompe disease in Japan in 2007. We conducted a post-marketing surveillance study to monitor the long-term safety and efficacy of alglucosidase alfa therapy among Japanese patients with Pompe disease.
Methods
The safety and efficacy outcomes were collected as real-world data for up to 9 years following the initiation of treatment with alglucosidase alfa, without any intervention to treatment strategies. The safety of the drug was assessed in 73 patients in terms of the rate of drug-related adverse events, infusion-associated reactions, and antibody titers. The efficacy was evaluated in 72 patients on the basis of subjective evaluation of their general condition after treatment, pulmonary function, 6-min walk test, and survival rate.
Results
Drug-related adverse events were observed in 29 of 73 (39.7%) cases, and the cumulative adverse event rate during the 9 years of the study was 45.7%. Immunoglobulin G antibodies against alglucosidase alfa were positive in 59 of 61 cases in which the titers were not correlated with drug-related adverse events or infusion-associated reactions. After the final dosing, the treating physicians determined that the disease was at least stabilized in 62 of 72 cases (86.1%), while the results of the physical function tests suggested that disease progression was actually not stopped completely. Survival of infantile-onset cases was sustained for 9 years.
Conclusion
The drug was generally well tolerated, and treatment with alglucosidase alfa was able to suppress disease progression in the majority of Japanese patients with Pompe disease included in this study.
Funding
Sanofi
Similar content being viewed by others


Introduction
Pompe disease is caused by an accumulation of glycogen as a result of the disordered degradation of glycogen in lysosomes due to a congenital abnormality in the acid α-glycosidase (GAA) gene [1,2,3,4,5]. This disease is an orphan disease with autosomal recessive inheritance; its incidence is estimated to be about one in 40,000 persons in the USA and it varies among ethnicities [1, 6]. The major symptoms of Pompe disease include skeletal and respiratory muscle weakness, and there is a wide disease spectrum, ranging from the infantile-onset type, which is characterized by the presence of cardiomegaly, to the adult-onset type, which occurs in advanced age [2, 3, 7]. It has been reported that patients with the most severe infantile-onset type of Pompe disease exhibit general hypotonia, cardiomegaly, and hepatomegaly and that the majority of these patients die from respiratory failure or cardiac failure less than 1 year after birth if the disease is left untreated [8]. Treatment for Pompe disease includes enzyme replacement therapy (ERT) with intravenous administration of recombinant human GAA (rhGAA) to supplement the deficency in GAA activity [9,10,11].
Alglucosidase alfa, an rhGAA, has widely been used as an ERT orphan drug for the treatment of Pompe disease in many countries and regions. It was approved for use in Japan in June 2007. The safety and efficacy of alglucosidase alfa have been examined in a number of clinical trials and research projects. Clinical trials conducted to date in patients with infantile-onset or late-onset Pompe disease have demonstrated positive effects in patients with either type of the disease, with sufficient short-term tolerance [12, 13]. In addition, post-marketing clinical studies have collected data on the long-term efficacy of this drug [10, 14]. However, these trials did not include Japanese patients, and to our knowledge there are currently no reported studies that examine the safety and efficacy of the long-term use of this drug in Japanese patients with Pompe disease.
Researchers have recently reported the genetic patterns of GAA gene of patients diagnosed with Pompe disease in Japan [15], and the results of newborn screening have also been published [16]. According to these reports the most frequent pathogenic variant of the GAA gene in the Japanese population is c.546G > T, which suggests that the genetic cause of Pompe disease in Japanese patients differs not only from that in patients in Western countries [17, 18], but also from that in patients in other Asian countries [19, 20]. In addition to the genetic difference, there are variations in cultural lifestyle among different ethnic groups. Therefore, to gain a true understanding of the pathological condition of a genetic disorder in a certain ethnic group and the efficacy and safety of treatment for the disease, analysis of epidemiological data on the group in question and the collection of data on changes in the pathological condition in the actual clinical setting are indispensable.
The objective of this study was to evaluate the safety and effectiveness of the long-term use of alglucosidase alfa in patients with Pompe disease in Japan. The post-marketing surveillance (PMS) was based on the Good Post-marketing Surveillance Practice (GPSP). We report here the analysis of long-term data from 73 evaluable cases of Pompe disease over a period of 9 years in terms of the incidence of adverse events (AEs), antibody production, pulmonary function, motor function, and survival rate.
Methods
Study Design and Ethical Issues
This PMS study targeted all patients with Pompe disease in Japan who received alglucosidase alfa, with treatment continuing for 9 years, from June 2007 to June 2016. We collected data on the background of patients with Pompe disease who were receiving ERT in clinical practice and on the safety and efficacy of alglucosidase alfa, without any intervention in the treating physicians’ discretion in adopting alglucosidase alfa therapy for their respective patient(s). In Japan, alglucosidase alfa has been approved for intravenous administration at 20 mg/kg every other week. In this study, data were available from 92 cases of Pompe disease, and publication of data was approved by the respective investigators or medical institutions for 73 of the 92 cases. These 73 cases whose data were subjected to analysis were widely distributed around the country (when finally evaluated: 8 in the Tohoku and Hokkaido area; 31 in the Kanto and Koshin area; 5 in the Tokai and Hokuriku area; 14 in the Kinki area, 4 in the Chugoku and Shikoku area; 11 in the Kyoshu area).
This PMS was required by the Pharmaceutical and Medical Device Agency, and it was conducted as a part of the risk management plan of alglucosidase alfa in accordance with the GPSP, an ordinance of the Ministry of Health, Labour and Welfare (MHLW). Approval of the ethical committee for the entire protocol of this study is exempted under GPSP ordinance by the MHLW. Also, because the surveillance of all patients who received the drug was a condition of approval by HMLW, the informed consent was also exempted under the GPSP. This study conforms to the provisions of the Declaration of Helsinki of 1964, as revised in 2013.
Case Composition
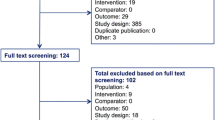
A total of 92 cases of Pompe disease in 79 institutions in Japan were registered in this surveillance (Fig. 1). Among these 92 cases, 73 were subjected to safety analysis and 19 were excluded because no consent to publication was obtained. One case was excluded from the efficacy analysis, as no data on overall improvement were available. The study was discontinued in nine cases due to the following: death (n = 6); transfer to hospital care by the patient (n = 2); other reason (n = 1).

Flow chart of case composition. Data for 92 cases were registered in this surveillance under the Good Post-marketing Surveillance Practice ordinance by the Ministry of Health, Labour and Welfare, of which data for 73 cases were included in the analysis
The treating physicians classified their respective patient(s) into one of three disease categories: infantile-, juvenile-, or adult-onset Pompe disease. As the Japanese guideline for Pompe disease suggests that such classification should take both age at disease onset and disease severity of each patient into consideration, there is no uniform and definitive criteria.
Safety
All AEs, other than those determined to have no causal relationship with alglucosidase alfa by the physician in charge, were defined as drug-related AEs (related-AEs). Related-AEs that occurred on the day of drug administration were defined as infusion-associated reactions (IARs), and their occurrence was investigated. The relationship between the presence or absence of antibody production and the incidence rate of related-AEs or IARs was evaluated. AEs were classified by means of the system organ class of the International Conference on Harmonisation Medical Dictionary for Regulatory Activities Ver. 19.1 and Preferred Terms. The following patient background factors were examined for a correlation with the incidence rates of related-AEs and IARs because they might affect the safety of the drug: gender, current age, age at onset, age at established (initial) diagnosis, time from onset to the beginning of treatment, time from established (initial) diagnosis to the beginning of treatment, type of Pompe disease, presence or absence of the history of treatment with this drug, height, body weight, presence or absence of history of the disease and complications, level of GAA enzyme activity, mean daily dose, mean single dose, mean total number of doses, and mean duration of administration.
Antibody Titer Assay
The production of anti-alglucosidase alfa antibodies [immunoglobulin G (IgG) and immunoglobulin E (IgE)] was determined by the enzyme-linked immunosorbent assay (ELISA) and radioimmunoprecipitation (RIP) assay [21]. For each patient, antibody titers were measured by collecting blood samples at baseline and just before administration of the drug every 3 months, until the end of the study. When there was a moderate or severe IAR, IgE antibody testing was performed on the patient. In the same manner as described above, the anti-alglucosidase alfa IgE antibody titer was determined by ELISA and RIP assays in blood samples collected from patients before administration of the drug.
Effectiveness
For assessment of each physical function, the physician recorded the forced vital capacity (FVC) of the patient in the standing position and the distance of 6-min walk test (6MWT). Pulmonary function was evaluated in terms of percentage of predicted FVC (%FVC). The survival rate was also determined using the Kaplan–Meier method. In addition, we evaluated the overall change in the disease state in each study participant. Overall improvement, as compared with the baseline status, was rated into six grades, namely, “well improved”, “improved”, “relatively improved”, “stable”, “worsened”, and “not evaluable”, by comprehensive judgment of the physician based on prior treatment, disease status, clinical symptoms, and improvement or deterioration in each symptom. In this report, the degree of changes at the time of the final evaluation is discussed.
Statistical Analysis
The category percentage and the basic statistics value were calculated for each patient background factor. To determine factors that might affect the safety of the treatment, stratified analysis of the frequency of related-AE cases and of the improvement rate for each patient background factor was performed using Fisher’s exact probability test. Items of efficacy evaluation were analyzed by the Chi-square test and Fisher’s exact probability test. Differences were regarded to be significant in all tests at a significance level of < 5% (two-tailed).
Results
Baseline Characteristics
A list of the baseline characteristics of the 73 patients (41 men; 32 women) who were evaluated for safety is provided in Table 1. All treating physicians classified their respective patient(s) into one of the three disease categories described in the Case Composition section, resulting in 10, 42, and 21 patients with infantile-, juvenile-, and adult-onset Pompe disease, respectively. In this cohort, juvenile-onset Pompe disease was the most prevalent, reported in 57.5% of patients. Available data on onset age showed that the classification of disease category was largely based on onset age and hence probably in accordance with disease severity. We calculated the average age at onset of the total patient cohort to be 8.5 years, but consider that it must have been higher because data on age at onset were frequently missing for adult-onset cases. The average age at diagnosis was 15.1 years. In the analysis of age at onset and at diagnosis, we excluded the data of four patients with juvenile-onset disease whose age at diagnosis were described as younger than age at onset. The most frequent symptom found in the patients was skeletal muscle symptoms, followed, in decreasing order of frequency, by respiratory, gastrointestinal, neurological, and cardiovascular symptoms.
Safety
Adverse Events
Among the 73 patients evaluated for safety, 504 AEs were identified in 55 (75.3%) patients. Of these AEs, 145 were related-AEs, found in 29 (39.7%) patients (Table 2). Cumulative incidence rates of related-AEs are shown in Electronic Supplementary Material (ESM) Fig. 1. When these data were analyzed in relation to patient age at baseline, the incidence rate of related-AEs was 19/33 in patients aged < 15 years, 8/34 in those aged 15 to < 65 years, and 1/4 in those aged ≥ 65 years, which shows a significant correlation between the incidence rate of related-AEs and patient age (P = 0.010). In relation to the mean daily dose, the incidence rate of related-AEs was 14/19 for doses of < 19 mg/kg and 15/53 for doses of ≥ 19 mg/kg. Thus, the incidence rate was significantly higher for those patients on lower doses (P < 0.01). In relation to the history of prior treatment, the corresponding rate was 5/23 in those with a history of prior treatment and 23/48 in those without such history, showing a slight but significant difference between the two groups (P < 0.05).
There were six deaths, which resulted from the following: primary disease (n = 3; comorbid advanced lung lesion present in one case); a complication (n = 1); severe pneumonia (n = 1); and unknown cause (n = 1). Laboratory tests revealed decreased blood pressure, increased eosinophil count, decreased oxygen saturation, and increased leukocyte count in one patient each. Overall, alglucosidase alfa was well tolerated throughout the study, with no treatment cessation due to AEs. The observed related-AEs in this Japanese population were similar to those previously reported in a multinational phase 3 trial [12].
Production of Anti-alglucosidase Alfa Antibody and the Relationship with AE Expression
In this study, the association of the production of anti-alglucosidase alfa antibodies (IgG and IgE) following administration of the drug and the IgG antibody titer with the incidence rates of related-AEs or IARs was examined. IgG antibody production was found in 59/61 (96.7%) of patients who received antibody tests. One patient underwent IgE antibody testing, and the result was negative. Changes in IgG antibody titer in patients with infantile-onset, juvenile-onset, and adult-onset Pompe disease after the administration of alglucosidase alfa are shown in Fig. 2a–c. The incidence rates of related-AEs and IARs were highest in a group of patients with IgG antibody titers of ≥ 400 to < 3200 (Table 3). However, there was no significant difference in the incidence rate of related-AEs or IARs among the three groups classified according to the IgG antibody titer (< 400, ≥ 400 to < 3200, and ≥ 3200).

Immunoglobulin G (IgG) titers of each patient. Of 61 patients with Pompe disease who underwent IgG testing, 59 were antibody positive at some point during the study period. a–c IgG titers of patients with infantile-onset Pompe disease (a), juvenile-onset Pompe disease (b), adult-onset Pompe disease (c). The data of each patient is shown in different colors. There was no obvious difference in IgG expression among patients with the three disease types for > 8 years
Effectiveness
Survival Rate
Figure 3 shows the Kaplan–Meier curves of the survival rates of patients up to 9 years after the initiation of ERT. In this study, six patients died during the 9 years of the ERT; the survival rate was therefore 89.5% [95% confidence interval (CI) 77.5–95.3]. Of the six patients who died, two were classified as having juvenile-onset Pompe disease and four were classified as having adult-onset disease. The survival rates of those with juvenile- and adult-onset Pompe disease after 9 years of ERT were 95.2% (95% CI 82.1–98.8) and 70.2% (95% CI 37.2–88.1), respectively. The cause of death was documented in only five of the six cases (one case of juvenile-onset disease was excluded) as follows: progression of the primary disease (n = 3), a complication (n = 1; details unclear), and severe pneumonia (n = 1). No deaths were reported among the ten patients with evaluable infantile-onset Pompe disease (Fig. 3b).

a Kaplan–Meier curve of survival rate of entire patient population. Survival rate at 9 years after initiation of enzyme replacement therapy (ERT) was 89.5% [95% confidence interval (CI) 77.5–95.3]. b Kaplan–Meier curve of survival rate of patients with infantile-, juvenile-, and adult-onset Pompe disease, respectively. Survival rates of patients with juvenile- and adult-onset Pompe disease at 9 years after ERT initiation were 95.2% (95% CI 82.1–98.8) and 70.2% (95% CI 37.2–88.1), respectively
Assessment of Respiratory and Motor Function
Decreased pulmonary function is the main cause of decreased quality of life and death in patients with Pompe disease, and the maintenance of pulmonary function appears to be a highly critical factor in the vital prognosis of these patients [22, 23]. In this study, the %FVC values in patients who received ERT for at least 2 years were analyzed (ESM Fig. 2a). When all the data points were converged into a linear regression, the %FVC values were found to decrease at an average rate of − 0.07% per month.
Impaired motor function is also one of the largest issues confronting patients with Pompe disease. In contrast to the FVC examination, however, we were able to collect only limited data on the 6MWT, likely because conducting this test in clinical practice places a heavy burden on both patients and physicians (ESM Fig. 2b). Data from 15 patients over a period of 2 years (range 30–102 months) were obtained, and the distance was found to decrease at an average rate of − 7.1 m per year for these 15 patients.
It has been suggested that anti-rhGAA antibody can mitigate the effectiveness of alglucosidase alpha [24], although the antibody is not always neutralizing. In order to evaluate the impact of IgG expression in this cohort, we analyzed the correlation between IgG titer and long-term respiratory outcome (ESM Fig. 2c). The data of 28 patients who received ERT for at least 2 years and for whom FVC data were available for at least 1 year were analyzed. The long-term outcome in each patient was evaluated by calculating a slope of %FVC regression from each trajectory, and these slopes were plotted against the highest titer value of IgG antibody. Although there was a tendency towards high antibody expression having a negative impact on the respiratory outcome, the overall correlation was weak (r = − 0.364) and did not reach statistical significance (P = 0.057).
Overall Improvement
Each of the 72 patients was evaluated at the final evaluation for overall improvement. Of these 72 patients, the physicians assessed 4 patients (5.6%) as well improved, 3 (4.2%) as improved, 8 (11.1%) as relatively improved, 47 (65.3%) as stable, 9 (12.5%) as worsened, and 1 (1.4%) as not evaluable.
Among the ten patients who were diagnosed with infantile-onset Pompe disease, symptoms were found to be relatively improved or better in four patients and stable in six. Among the 62 patients who were diagnosed with late-onset Pompe disease (42 juvenile- and 20 adult-onset), symptoms were found to be relatively improved or better in 11 patients (2 adult-onset), stable in 41 (16 adult-onset), worsened in 9 (1 adult-onset), and not evaluable in 1 (adult-onset). We were unable to detect a significant difference in the ratio of the patients whose symptoms were relatively improved or better among the three disease types (P = 0.160), but most of the patients were < 15 years of age at baseline (13/15 patients, P < 0.001).
Discussion
In this study we examined the safety and efficacy of long-term use of alglucosidase alfa therapy (up to 9 years) using real-world data collected on Japanese patients with Pompe disease. The drug was well tolerated, and no new concerns about safety and efficacy of this drug were found.
The treating physicans categorized the disease types as juvenile-onset (57.5% of patients), adult-onset (28.8% of patients), and infantile-onset (13.7% of patients). In previous studies conducted in Europe and North America, the age at onset of this disease was frequently reported to be ≥ 18 years, excluding patients with typical infantile-onset Pompe disease [25]. In this cohort, however, for the 50 patients with juvenile- and adult-onset whose age at diagnosis was available, more than half (33/50) were diagnosed at a age of < 18 years, suggesting that the distribution of age at onset in Japanese patients diagnosed with late-onset Pompe disease may differ from that of patients in Europe and North America. The distribution of age at onset in patients diagnosed with late-onset Pompe disease may be influenced by the level of disease recognition in that region, but it is also possible that the disease itself has region-specific properties. One possible explanation is the presence of genetic ethnicity [15, 16], but unfortunately in this study we did not collect information on genetic patterns. It was therefore impossible to investigate the relationship between genotypes and disease severity or the presence of phenotypes which might be associated with certain genotypes. The ethnicity factor of Pompe disease was thus left uninvestigated in this study. Large-scale screening of neonates and extensive genetic analysis of the general Japanese population are required to investigate this issue [16, 26,27,28]. Genetic disorders may not only exhibit ethnic specificity [29, 30], but also regional specificity [31], and there is a possibility that detailed investigation of the characteristics of Pompe disease in Japan may lead to a deeper understanding of this disease.
A total of 145 related-AEs were observed in 29 of the 73 patients. The major related-AEs included urticaria, fever, and coughing, and the related-AEs found in this study were similar to those of reported in an international trial [12]. Among the patients who experienced related-AEs, these related-AEs tended to occur in an early stage of treatment (ESM Fig. 1). The incidence rate of related-AEs was higher in younger patients (< 15 years) and in those who were given a lower daily dose. The higher incidence rate among the latter group of patients may be partly attributable to the presence of young patients in this group for whom no dose adjustment was made for increased body weight or for whom the dose was decreased due to the occurrence of IARs. Among nine patients for whom the administration of this drug was discontinued completely, there was no case which discontinuation was due to insufficient efficacy or the occurrence of AEs. A previous study documented that the administration of alglucosidase alfa for up to 168 weeks led to the production of IgG antibodies to this drug in 19 (95%) of 20 patients (infants and children) with Pompe disease [32]. Although our results also revealed that there was a high percentage of IgG antibody production after the administration of this drug, as found in 59 (96.7%) of 61 patients, including those with adult-onset disease, there was no significant difference between the IgG antibody titer and the incidence rate of related-AEs or IARs in these patients. Based on these findings, we can report no new concerns related to alglucosidase alfa therapy in the Japanese patient population.
Although immune modulation has been recommended for cross-reactive immunologic material-negative patients with infantile-onset Pompe disease, the influence of antibody production on ERT in patients with late-onset Pompe disease remains unclear [33, 34]. Observation of changes in the antibody titer revealed that there was no decrease in antibody production during the long-term administration of alglucosidase alfa (Fig. 2), unlike results reported in previous studies [34]. In terms of the influence of antibody production on the effectiveness of alglucosidase alfa, we observed only a weak tendency towards a negative impact on the long-term respiratory outcome which did not reach statistical significance (ESM Fig. 2). Further study on the larger dataset with physical evaluations before and after ERT initiation will enable us to evaluate the outcome more precisely, and multi-variate analyses taking other influential factors into consideration, such as disease severity and treatment adherence, will also be useful to clarify the actual impact of antibody production on the effectiveness of ERT.
Although the disease state was generally unchanged in the majority of the patients (65.3%), physical function tests showed a gradual deterioration during the study period. This discrepancy is likely to be due, at least in part, to a bias in the questionnaire related to the choice of six grades on overall improvement, with three choices that were improvement related, one for stable, and one for worsening. However, the decrease in %FVC in our study (− 0.07%/month) was actually more gradual than that reported in the placebo group of a clinical trial in late-onset Pompe disease (− 0.11%/month) [12], which demonstrates a certain level of ERT effectiveness in slowing down disease progression. Although it has been suggested that the maintenance of respiratory function after the introduction of ERT is still one of the unmet needs of disease treatment, the result is consistent with those reported previously showing the mitigation of respiratory deterioration by ERT [9, 10]. On the other hand, no initial increase in %FVC was observed in this study when compared with previous clinical trial and meta-analysis findings [9, 12]. This difference might be explained partly by the difference in disease severity between the participants in the different studies. In actuality, judged from the available data of ages at onset and diagnosis, it is likely that the mean age at onset in this cohort was lower than that of the patient group in a phase 3 study (30.3 ± 12.3 years for the active drug; 23.9 ± 11.0 years for the placebo). Also, patient groups with different disease types might have been included in this cohort. Another factor which may contribute to the discrepancy is that some patients in the present study had already received the drug before study initiation as compassionate use (see following text).
Among the patients included in this study, all those with infantile-onset Pompe disease were alive at the end of the study period. It has been reported that the survival rate of untreated patients with infantile-onset Pompe disease is 1.9% at 52 weeks [13]. Therefore, the efficacy of this drug on the survival rate of this group of patients has now also been confirmed in Japan. The efficacy of alglucosidase alfa on the survival rate of patients with late-onset Pompe disease was the focus of a previous study [14]. However, considering the lack of natural history in the Japanese cohort, it is difficult to discuss the influence of this drug on the survival of this group of patients based on the data obtained in this study.
This observational study has a number of significant limitations, which arise from the study design. First, the data were collected only after alglucosidase alfa therapy had officially been approved in Japan. Therefore, as mentioned previously, data on the specific use of this drug before approval could not be included. Thus, the collection of data did not necessarily begin at the time of initiation of this drug therapy in all patients. Second, the quality control of data collected by this PMS was insufficient relative the that of clinical trials, and there may have been bias due to differences in the evaluation criteria among different physicians. Therefore, the level of evidence was not as high as that in clinical trials conducted under strict conditions. Third, the study was significantly influenced by physicians’ permission to use the data. This report included the data of only 73 patients, for whom publication of the results was permitted by the investigator or the medical institution. Therefore, it is possible that permission to use data might have been affected by the prognosis of the patient or a transfer to hospital care by the patients.
Despite the above-mentioned limitations, the data from this study are invaluable to promoting a better understanding of the pathological conditions of Pompe disease in Japan. Data on 78% (73 of 92 patients) of all patients were used for this report, and there was no obvious discrepancy from the results of safety and efficacy evaluations in all 92 patients used for the report to the Japanese authority (Pharmaceuticals and Medical Devices Agency). Thus, we consider that the content of this report well reflects the actual characteristics of the disease and the use of alglucosidase alfa in Japan. Previous studies have demonstrated that Pompe disease is a complex disease [7]. To further deepen our understanding of Pompe disease, it is necessary to collect and analyze multiphasic data with a certain level of quality control for a longer period of time.
Conclusions
This paper reports the results of a large-scale, prolonged survey on alglucosidase alfa for the treatment of Pompe disease in Japanese patients. We found that most related-AEs were not serious (outcome: recovered/resolved or recovering/resolving) and that the treatment with alglucosidase alfa was well tolerated with no treatment cessation due to an AE. Even with the slow progression of physical symptoms, the disease state was assessed as “stabilized” or “better” in 86.1% of the patients, and the survival rate was maintained at high levels during the long-term administration of therapy with alglucosidase alfa. Based on these findings, we conclude that there are no new concerns about the safety and efficacy of this drug for long-term use in Japan.
References
Reuser AJ, Hirschhorn R, Kroos MA. Pompe disease: glycogen storage disease type II, acid α-glucosidase (acid maltase) deficiency. In: Valle D, Beaudet AL, Vogelstein B, Kinzler KW, Antonarakis SE, Ballabio A, Gibson K, Mitchell G, eds. The online metabolic and molecular bases of inherited disease. New York: McGraw-Hill; 2014. http://ommbid.mhmedical.com/content.aspx?bookid=971§ionid=62641992.
Kishnani PS, Steiner RD, Bali D, et al. Pompe disease diagnosis and management guideline. Genet Med. 2006;8(5):267–88.
van der Ploeg AT, Reuser AJ. Pompe’s disease. Lancet. 2008;372(9646):1342–53.
Chien YH, Hwu WL, Lee NC. Pompe disease: early diagnosis and early treatment make a difference. Pediatr Neonatol. 2013;54(4):219–27.
Lim JA, Li L, Raben N. Pompe disease: from pathophysiology to therapy and back again. Front Aging Neurosci. 2014;6:177.
Martiniuk F, Chen A, Mack A, et al. Carrier frequency for glycogen storage disease type II in New York and estimates of affected individuals born with the disease. Am J Med Genet. 1998;79(1):69–72.
Chan J, Desai AK, Kazi ZB, et al. The emerging phenotype of late-onset Pompe disease: a systematic literature review. Mol Genet Metab. 2017;120(3):163–72.
van den Hout HM, Hop W, van Diggelen OP, et al. The natural course of infantile Pompe’s disease: 20 original cases compared with 133 cases from the literature. Pediatrics. 2003;112:332–40.
Schoser B, Stewart A, Kanters S, et al. Survival and long-term outcomes in late-onset Pompe disease following alglucosidase alfa treatment: a systematic review and meta-analysis. J Neurol. 2017;264(4):621–30.
Kuperus E, Kruijshaar ME, Wens SCA, et al. Long-term benefit of enzyme replacement therapy in Pompe disease: A 5-year prospective study. Neurology. 2017;89(23):2365–73.
Toscano A, Schoser B. Enzyme replacement therapy in late-onset Pompe disease: a systematic literature review. J Neurol. 2013;260(4):951–9.
Ploeg AT, Clemens PR, Corzo D, et al. A randomized study of alglucosidase alfa in late-onset Pompe’s disease. N Engl J Med. 2010;362(15):1396–406.
Kishnani PS, Corzo D, Nicolino M, et al. Recombinant human acid [alpha]-glucosidase: major clinical benefits in infantile-onset Pompe disease. Neurology. 2007;68(2):99–109.
Güngör D, Kruijshaar ME, Plug I, et al. Impact of enzyme replacement therapy on survival in adults with Pompe disease: results from a prospective international observational study. Orphanet J Rare Dis. 2013;8:49.
Fukuhara Y, Fuji N, Yamazaki N, et al. A molecular analysis of the GAA gene and clinical spectrum in 38 patients with Pompe disease in Japan. Mol Genet Metab Rep. 2017;14:3–9.
Momosaki K, Kido J, Yoshida S, et al. Newborn screening for Pompe disease in Japan: report and literature review of mutations in the GAA gene in Japanese and Asian patients. J Hum Genet. 2019. https://doi.org/10.1038/s10038-019-0603-7.
Laforêt P, Nicolino M, Eymard PB, et al. Juvenile and adult-onset acid maltase deficiency in France: genotype–phenotype correlation. Neurology. 2000;55(8):1122–8.
Kroos MA, Van der Kraan M, Van Diggelen OP, et al. Glycogen storage disease type II: frequency of three common mutant alleles and their associated clinical phenotypes studied in 121 patients. J Med Genet. 1995;32(10):836–7.
Liu X, Wang Z, Jin W, et al. Clinical and GAA gene mutation analysis in mainland Chinese patients with late-onset Pompe disease: identifying c.2238G>C as the most common mutation. BMC Med Genet. 2014;15:141.
Park HD, Lee DH, Choi TY, et al. Three patients with glycogen storage disease type II and the mutational spectrum of GAA in Korean patients. Ann Clin Lab Sci. 2013;43(3):311–6.
Kishnani PS, Nicolino M, Voit T, et al. Chinese hamster ovary cell-derived recombinant human acid alpha-glucosidase in infantile-onset Pompe disease. J Pediatr. 2006;149(1):89–97.
Hagemans ML, Winkel LP, Van Doorn PA, et al. Clinical manifestation and natural course of late-onset Pompe’s disease in 54 Dutch patients. Brain. 2005;128(Pt 3):671–7.
Güngör D, de Vries JM, Hop WC, et al. Survival and associated factors in 268 adults with Pompe disease prior to treatment with enzyme replacement therapy. Orphanet J Rare Dis. 2011;6:34.
de Vries JM, Kuperus E, Hoogeveen-Westerveld M, et al. Pompe disease in adulthood: effects of antibody formation on enzyme replacement therapy. Genet Med. 2017;19(1):90–7.
Winkel LP, Hagemans ML, van Doorn PA, et al. The natural course of non-classic Pompe’s disease; a review of 225 published cases. J Neurol. 2005;252(8):875–84.
Chiang SC, Hwu WL, Lee NC, Hsu LW, Chien YH. Algorithm for Pompe disease newborn screening: results from the Taiwan screening program. Mol Genet Metab. 2012;106(3):281–6.
Oda E, Tanaka T, Migita O, et al. Newborn screening for Pompe disease in Japan. Mol Genet Metab. 2011;104(4):560–5.
Yamaguchi-Kabata Y, Yasuda J, Tanabe O, et al. Evaluation of reported pathogenic variants and their frequencies in a Japanese population based on a whole-genome reference panel of 2049 individuals. J Hum Genet. 2018;63:213–30.
Watanabe M, Kobayashi K, Jin F, et al. Founder SVA retrotransposal insertion in Fukuyama-type congenital muscular dystrophy and its origin in Japanese and Northeast Asian populations. Am J Med Genet A. 2005;138(4):344–8.
Eto Y, Ida H. Clinical and molecular characteristics of Japanese Gaucher disease. Neurochem Res. 1999;24(2):207–11.
Ikeda S, Nakazato M, Ando Y, Sobue G. Familial transthyretin-type amyloid polyneuropathy in Japan: clinical and genetic heterogeneity. Neurology. 2002;58(7):1001–7.
Nicolino M, Byrne B, Wraith JE, Leslie N, Mandel H. Clinical outcomes after long-term treatment with alglucosidase alfa in infants and children with advanced Pompe disease. Genet Med. 2009;11(3):210–9.
Patel TT, Banugaria SG, Case LE, Wenninger S, Schoser B, Kishnani PS. The impact of antibodies in late-onset Pompe disease: a case series and literature review. Mol Genet Metab. 2012;106(3):301–9.
Masat E, Laforêt P, De Antonio M, et al. Long-term exposure to Myozyme results in a decrease of anti-drug antibodies in late-onset Pompe disease patients. Sci Rep. 2016;6:36182.
Acknowledgements
The authors express their sincere gratitude to all physicians and investigators who cooperated in this surveillance study and provided valuable data. The authors also express their greatest thanks to the participants of the study.
Funding
This surveillance was conducted in accordance with Good Post-marketing Surveillance Practice in Japan and was fully funded and conducted by Sanofi K.K. The Rapid Service Fee was also funded by Sanofi K.K. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Medical Writing and/or Editorial Assistance
The authors thank Akira Karikome at CMIC Co., Ltd. for statistical analysis assistance and thank Honyaku Center Inc. for preparation of the first draft of this manuscript. Sanofi K.K. provided funding for this assistance.
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval of the version to be published.
Authorship Contributions
HN contributed to the study design, analyzed and interpreted the data, and drafted and finalized the manuscript. JH contributed to the study design, analyzed and interpreted the data, and critically revised the manuscript for intellectual content. HK and KU interpreted the data and critically revised the manuscript for intellectual content.
Disclosures
Hitoshi Nagura is an employee of Sanofi. Jiro Hokugo is an employee of Sanofi. Kazuo Ueda is an employee of Sanofi.
Compliance with Ethics Guidelines
This PMS was required by the Pharmaceutical and Medical Device Agency and conducted as a part of risk management plan of alglucosidase alfa in accordance with the Good Post-marketing Surveillance Practice (GPSP), an ordinance of the Ministry of Health, Labour and Welfare (MHLW). Ethical committee approval of the entire protocol of this study is exempted under GPSP ordinance by MHLW. Also, because the surveillance of all the patients who received the drug was a condition of approval by the HMLW, a requirement for informed consent was also exempted under the GPSP. This study conforms to the provisions of the Declaration of Helsinki of 1964, as revised in 2013.
Data Availability
The datasets generated and/or analyzed during the current study are fully owned by Sanofi K.K., and not publicly available. They are available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced digital features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.9822683.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Nagura, H., Hokugo, J. & Ueda, K. Long-Term Observation of the Safety and Effectiveness of Enzyme Replacement Therapy in Japanese Patients with Pompe Disease: Results From the Post-marketing Surveillance. Neurol Ther 8, 397–409 (2019). https://doi.org/10.1007/s40120-019-00157-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-019-00157-4