
Abstract
Purpose
Peripheral facial nerve palsy (FP) is the most common single nerve affection. Most cases are idiopathic, but a relevant fraction is caused by potentially treatable aetiologies including infections. Not all current diagnosis and treatment guidelines recommend routine cerebrospinal fluid (CSF) analysis in the diagnostic workup of this symptom. In this study, we evaluated frequency of aetiologies and relevance of CSF analysis in an interdisciplinary cohort.
Methods
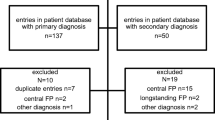
We retrospectively analysed all cases of newly diagnosed FP treated at a German university medical centre in a 3-year period. Diagnostic certainty was classified for infectious aetiologies according to clinical and CSF parameters.
Results
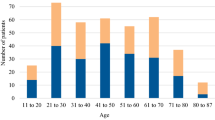
380 patients with FP were identified, 63 children and 317 adults. Idiopathic Bell´s palsy was predominant in 61 %. 25 % of FP was attributed to infections, and other causes were identified in 14 %. Clinical presentation alone was not conclusive for infectious aetiology, in almost half of patients with infection-attributed FP the reported symptoms or clinical signs did not differ from common symptoms of idiopathic Bell`s palsy. Determination of C-reactive protein or white blood cell count was not helpful in the identification of infectious causes, and radiological imaging was performed in a high proportion of adult patients without conclusive results. Nuchal rigidity was found only in 7 % of patients with CSF pleocytosis. The predominant infectious agents were Borrelia burgdorferi, VZV and HSV, and in most of these cases diagnosis relied on the findings of CSF analysis.
Conclusions
This study outlines the importance of careful differential diagnosis to identify infectious causes of facial nerve palsy. The high incidence and frequent unspecific clinical presentation of infectious FP underlines the importance of including CSF analysis in the diagnostic routine workup of FP.




Similar content being viewed by others

References
Rowlands S, Hooper R, Hughes R, Burney P. The epidemiology and treatment of Bell’s palsy in the UK. Eur J Neurol. 2002;9:63–7.
Tveitnes D, Oymar K, Natas O. Acute facial nerve palsy in children: how often is it lyme borreliosis? Scand J Infect Dis. 2007;39:425–31.
Monini S, Lazzarino AI, Iacolucci C, Buffoni A, Barbara M. Epidemiology of Bell’s palsy in an Italian Health District: incidence and case-control study. Acta Otorhinolaryngol Ital. 2010;30:198.
Rowhani-Rahbar A, Baxter R, Rasgon B, Ray P, Black S, Klein JO, et al. Epidemiologic and clinical features of Bell’s palsy among children in Northern California. Neuroepidemiology. 2012;38:252–8.
Salinas RA, Alvarez G, Daly F, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2010;3. doi:10.1002/14651858.CD001942.
Gagyor I, Madhok VB, Daly F, Somasundara D, Sullivan M, Gammie F, et al. Withdrawn: antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2015;9. doi:10.1002/14651858.CD001869.
Gilden DH. Clinical practice: Bell’s Palsy. N Engl J Med. 2004;351:1323–31.
Baugh RF, Basura GJ, Ishii LE, Schwartz SR, Drumheller CM, Burkholder R, et al. Clinical practice guideline: Bell’s Palsy executive summary. Otolaryngol Head Neck Surg. 2013;149:656–63.
de Almeida JR, Guyatt GH, Sud S, Dorion J, Hill MD, Kolber MR, et al. Management of Bell palsy: clinical practice guideline. CMAJ. 2014;186:917–22.
Heckmann JG, Urban P, Glocker FX, Weder B, Reiter G, Bischoff C, et al. Therapie der idiopathischen Fazialisparese (Bell’s Palsy). In: Diener H, Weimar C, editors. Leitlinien für diagnostik und therapie in der neurologie. Stuttgart: Thieme; 2012. p. 656–66.
Mygland A, Ljostad U, Fingerle V, Rupprecht T, Schmutzhard E, Steiner I, et al. EFNS guidelines on the diagnosis and management of European Lyme neuroborreliosis. Eur J Neurol. 2010;17:e11–4.
Rauer S, Kaiser R, Kölmel HW, Pfister HW, Schmutzard E, Sturzenegger M, et al. Neuroborreliose. In: Diener H, Weimar C, editors. Leitlinien für diagnostik und therapie in der neurologie. Stuttgart: Thieme; 2012. p. 513–22.
Häusler M, Rostásy K, Orlikowsky T, Christen HJ. Nicht-eitrige ZNS Infektionen von Gehirn und Rückenmark im Kindes- und Jugendalter. AWMF. 2015 (Register Nr. 022/004).
Tunkel AR, Glaser CA, Bloch KC, Sejvar JJ, Marra CM, Roos KL, et al. The management of encephalitis: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. 2008;47:303–27.
Nagel MA, Cohrs RJ, Mahalingam R, Wellish MC, Forghani B, Schiller A, et al. The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features. Neurology. 2008;70:853–60.
Reiber H, Lange P. Quantification of virus-specific antibodies in cerebrospinal fluid and serum: sensitive and specific detection of antibody synthesis in brain. Clin Chem. 1991;37:1153–60.
Kaiser R, Lucking CH. Intrathecal synthesis of specific antibodies in neuroborreliosis. Comparison of different ELISA techniques and calculation methods. J Neurol Sci. 1993;118:64–72.
Belman AL, Reynolds L, Preston T, Postels D, Grimson R, Coyle PK. Cerebrospinal fluid findings in children with Lyme disease-associated facial nerve palsy. Arch Pediatr Adolesc Med. 1997;151:1224–8.
Heininger U, Ries M, Harms D, Brade V. Facial palsy with elevated protein in otherwise normal CSF in a child with Lyme disease. Infection. 1991;19:245–6.
Blumenthal DT, Shacham-Shmueli E, Bokstein F, Schmid DS, Cohrs RJ, Nagel MA, et al. Zoster sine herpete: virologic verification by detection of anti-VZV IgG antibody in CSF. Neurology. 2011;76:484–5.
Ratzka P, Schlachetzki JC, Bahr M, Nau R. Varicella zoster virus cerebellitis in a 66-year-old patient without herpes zoster. Lancet. 2006;367:182.
Broekhuijsen-van Henten DM, Braun KP, Wolfs TF. Clinical presentation of childhood neuroborreliosis; neurological examination may be normal. Arch Dis Child. 2010;95:910–4.
Hato N, Yamada H, Kohno H, Matsumoto S, Honda N, Gyo K, et al. Valacyclovir and prednisolone treatment for Bell’s palsy: a multicenter, randomized, placebo-controlled study. Otol Neurotol. 2007;28:408–13.
Rupprecht TA, Lechner C, Tumani H, Fingerle V. CXCL13: a biomarker for acute Lyme neuroborreliosis: investigation of the predictive value in the clinical routine. Nervenarzt. 2014;85:459–64.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standard
The Ethics Committee of the University Medical Centre Göttingen approved the research protocol for this non-interventional retrospective data analysis and did not see any need for obtaining patient consent. Therefore, this data analysis was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Funding
This study was supported by the Else Kröner-Fresenius-Stiftung (to A.S., H.E. and R.N.) and by the Robert-Koch-Institut (to A.S.) within the network “Klinisches Netzwerk Neuroborreliose”.
Rights and permissions
About this article

Cite this article
Henkel, K., Lange, P., Eiffert, H. et al. Infections in the differential diagnosis of Bell’s palsy: a plea for performing CSF analysis. Infection 45, 147–155 (2017). https://doi.org/10.1007/s15010-016-0933-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-016-0933-8