
Abstract
Objective
This study aimed to investigate the relationship between serum cystatin C level and pregnancy complications and abnormal glucose tolerance at 6-week postpartum in patients with gestational diabetes mellitus (GDM).
Methods
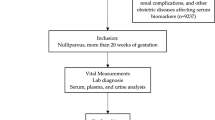
Clinical data of 298 cases of GDM delivered in Taizhou People’s Hospital from January 2017 to June 2018 were retrospectively analyzed. According to the level of cystatin C before delivery, they were divided into normal group (≤ 1.1 mg/L) and elevated group (> 1.1 mg/L). The general situation, complications of pregnancy, and the incidence of abnormal glucose tolerance at 6 weeks after delivery were compared between the two groups. According to concomitant gestational hypertension in late pregnancy, the patients were divided into group A (GDM with hypertensive disorder complicating pregnancy (HDCP)) and group B (GDM without HDCP). The differences of age, parity, body mass index (BMI) and mean arterial pressure (MAP) in the first trimester of pregnancy, levels of cystatin C, creatinine, urinary microalbumin, and glycosylated hemoglobin in 24-week gestation and before delivering were compared between the two groups.
Results
There was no significant difference in age and parity between the normal group and the elevated group (p > 0.05). The levels of BMI (25.06 ± 3.46 vs 26.34 ± 3.65 kg/m2), creatinine (38.76 ± 16.52 vs 59.75 ± 17.82 mmol/L), and urinary microalbumin (37.11 ± 49.20 vs 61.25 ± 43.52 mg/L) and the incidence of premature delivery (9.35% vs 17.8%), premature rupture of membranes (11.22% vs 20.94%), and abnormal glucose tolerance at 6-week postpartum (18.69% vs 42.93%) in the normal group of cystatin C were significantly lower than that in the elevated group of cystatin C (p < 0.05). There was no significant difference in the incidence of hypertension (8.41% vs 7.85%) and oligohydramnios (33.64% vs 24.61%) between the two groups (p > 0.05). The clinical characteristics of group A (GDM with HDCP) and group B (GDM without HDCP) were compared. The results showed that the levels of age, BMI, and mean arterial pressure (MAP) were significantly different (p < 0.001). The results of binary logistic regression analysis showed that the significance value of MAP was 0.005 after controlling age factors, which indicated that MAP was an independent risk factor of GDM with HDCP, and the OR value of MAP was 1.420 (1.109–1.817).
Conclusion
The increase of cystatin C in patients with GDM does not increase the risk of HDCP, but it does increase the risks of premature delivery, PROM, and abnormal glucose tolerance at 6-week postpartum. Cystatin C is a biological index that may be valuable in predicting the occurrence of these diseases in GDM patients. The independent risk factor of GDM complicating HDCP is MAP.
Similar content being viewed by others


References
Sun WJ, Yang HX. Maternal and fetal outcomes in pregnant women with abnormal glucose metabolism. Zhonghua Fu Chan Ke Za Zhi. 2007;42(6):377–81 Chinese.
Bjornstad P, Cherney DZI. Kidney function can predict pregnancy outcomes. Clin J Am Soc Nephrol. 2017;12:1029–31.
Nevis IF, Reitsma A, Dominic A, McDonald S, Thabane L, Akl EA, et al. Pregnancy outcomes in women with chronic kidney disease: a systematic review. Clin J Am Soc Nephrol. 2011;6:2587–98.
Piccoli GB, Attini R, Vasario E, Conijn A, Biolcati M, D’Amico F, et al. Pregnancy and chronic kidney disease: a challenge in all CKD stages. Clin J Am Soc Nephrol. 2010;5:844–55.
Bellos I, Fitrou G, Daskalakis G, Papantoniou N, Pergialiotis V. Serum cystatin-c as predictive factor of preeclampsia: a meta-analysis of 27 observational studies. Pregnancy Hypertens. 2019 Apr;16:97–104.
Risch M, Purde MT, Baumann M, Mohaupt M, Mosimann B, Renz H, et al. High first-trimester maternal blood cystatin C levels despite normal serum creatinine predict pre-eclampsia in singleton pregnancies. Scand J Clin Lab Invest. 2017 Dec;77(8):634–43.
Niraula A, Lamsal M, Baral N, et al. Combination of NGAL and Cystatin C for prediction of preeclampsia at 10–14 weeks of gestation. Clin Lab. 2019;65(5).
Thilaganathan B, Ralph E, Papageorghiou AT, Melchiorre K, Sheldon J. Raised maternal serum cystatin C: an early pregnancy marker for preeclampsia. Reprod Sci. 2009;16(8):788–93.
Franceschini N, Qiu C, Barrow DA, Williams MA. Cystatin C and preeclampsia: a case control study. Ren Fail. 2008;30(1):89–95.
Yarcı GA, Tasci Y, Hatice C, et al. The prognostic value of first-trimester cystatin C levels for gestational complications. J Perinat Med. 2016;44(3):295–9.
Yalcin S, Ulas T, Eren MA, et al. Relationship between oxidative stress parameters and cystatin C levels in patients with severe preeclampsia. Medicina (Kaunas). 2013;49:118–23.
Zhao W, Pan J, Li H, Huang Y, Liu F, Tao M, et al. Relationship between high serum cystatin C levels and the risk of gestational diabetes mellitus. PLoS One. 2016;11(2):e0147277.
Uruska A, Araszkiewicz A, Zozulinska-Ziolkiewicz D, et al. Does serum cystatin C level reflect insulin resistance in patients with type 1 diabetes? Clin Biochem. 2014;47(13–14):1235–8.
Reutens AT, Bonnet F, Lantieri O, Roussel R, Balkau B, For the data from an epidemiological study on the insulin resistance syndrome study group. Epidemiological study on the insulin resistance syndrome study group. The association between cystatin C and incident type 2 diabetes is related to central adiposity. Nephrol Dial Transplant. 2013;28(7):1820–9.
Lee SH, Parka SA, Ko SH, et al. Insulin resistance and inflammation may have an additional role in the link between cystatin C and cardiovascular disease in type 2 diabetes mellitus patients. Metabolism. 2010;59(2):241–6.
Curhan G. Cystatin C: a marker of renal function or something more? Clin Chem. 2005;51:293–4.
Wattanavaekin K, Kitporntheranunt M, Kreepala C. Cystatin C as a novel predictor of preterm labor in severe preeclampsia. Kidney Res Clin Pract. 2018 Dec;37(4):338–46.
Chad L, Miriam M, Wolfgang K, Frank R. Association of maternal uric acid and cystatin C serum concentrations with maternal and neonatal cardiovascular risk markers and neonatal body composition: the Ulm SPATZ Health Study. PLoS One. 2018;13(7).
Wu LF, Liu DY, Huang XH, et al. Postpartum reclassification in women with gestational diabetes and analyzing the high risk factors associated with them. Zhonghua Fu Chan Ke Za Zhi. 2003;38(3):140–2 Chinese.
Yinchuan L, Zhenjuan T, Qing T, et al. Analysis of postpartum follow-up results of pregnant women with abnormal glucose tolerance. Chin J Pract Gynecol Obstet. 2007;23(12):960–2 Chinese.
Yogev Y, Langer O, Brustman L, Rosenn B. Pre-eclampsia and gestational diabetes mellitus: does a correlation exist early in pregnancy? J Matern Fetal Neonatal Med. 2004;15(1):39–43.
Funding
This work was supported by the Taizhou People’s hospital under grant number ZD201711.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics statement
This study was approved by the Ethics Committee of Taizhou People’s Hospital in Jiangsu Province. It was designed in accordance with the principle of the Helsinki Declaration. Written informed consent was obtained from all of participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tang, X., Ju, H., Yang, L. et al. Relationship between serum cystatin C level and pregnancy complications and abnormal glucose tolerance at 6-week postpartum in patients with gestational diabetes mellitus. Int J Diabetes Dev Ctries 40, 532–537 (2020). https://doi.org/10.1007/s13410-020-00839-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-020-00839-y