
Abstract
Objective
To apply the process mapping technique in an interdisciplinary approach in order to visualize, better understand, and efficiently organize percutaneous transluminal angioplasty (PTA) and stent placement procedures in a university hospital’s interventional radiology department.
Methods
After providing an overview of seven established mapping techniques for medical professionals, the process mapping technique was chosen and applied in an interdisciplinary approach including referrers (physicians, nurses, and other staff in referring departments, e.g., vascular surgery), providers (interventional radiologists, nurses, technicians, and staff of the angiography suite), and specialists of the hospital’s controlling department.
Results
A generally binding and standardized process map was created, describing the entire procedure for a patient in whom the radiological intervention of PTA or stent treatment is contemplated from admission to the department of vascular surgery until discharge after successful treatment. This visualization tool assists in better understanding (especially given natural staff fluctuation over time) and efficiently organizing PTA and stent procedures.
Conclusion
Process mapping can be applied for streamlining workflow in healthcare, especially in interdisciplinary settings. By defining exactly what a business entity does, who is responsible, to what standard a process should be completed, and how the success can be assessed, this technique can be used to eliminate waste and inefficiencies from the workplace while providing high-quality goods and services easily, quickly, and inexpensively.
Main Messages
• Process mapping can be used in a university hospital’s interventional radiology department.
• Process mapping can describe the patient’s entire process from admission to PTA/stent placement until discharge.
• Process mapping can be used in interdisciplinary teams (e.g., referrers, providers, and controlling specialists).
• Process mapping can be used in order to more efficiently organize PTA and stent placement procedures.
• Process mapping can assist in better understanding and efficiently organizing procedures in standardized fashion.
Similar content being viewed by others

Introduction
Processes of patient care have become increasingly complex and interdisciplinary. This may be especially attributed to advances in technology—including diagnosis as well as treatment—but also because of advances in regulation and continuous diversification of medical specialties. However, while healthcare itself has advanced in technology and understanding of disease, its business and management models have hardly changed since the 1950s [1]. This is surprising since both innovative and well-established economic tools are widely applied in other industries and in fact available to be applied in the healthcare sector with moderate effort as well.
It is mainly in the last 2 decades that economic tools, including, among others, process management and manufacturing systems such as the Toyota Production System (TPS) [2], Lean Manufacturing, and Six Sigma, but also learning systems and other quality control initiatives, have been increasingly applied in healthcare settings: these approaches have been used to eliminate excess clinic inventory, better synchronize office supplies with patient demand, and of course reduce costs and wastes [3]. Economic learning and management systems [4] aim at achieving sustainable improvements in efficiency and productivity, staff and patient satisfaction, and of course quality outcomes [5], while reducing medical errors and costs. The latter seems especially noteworthy since one major reason for rising healthcare costs is in fact medical errors—the majority of which again result from faulty systems and processes [6]. From a controlling perspective, it is a challenging task to integrally control ever more complex processes to the outmost extent possible: Proactive quality management tools, including process mapping, value stream mapping (VSM), fault tree analysis, and failure mode and effects analysis [7], can help in achieving continuous efficiency improvement [8], especially in well-defined procedures.
Also in radiology departments and practices, Lean and Six Sigma process improvement methodologies [9] as well as numerous other industrial engineering practices [10] including TPS have recently been implemented and have since been widely applied to better control processes. This includes implementation of speech recognition reporting [11] as well as observations of electronic medical record usage during computed tomography (CT) and magnetic resonance imaging (MRI) interpretation for evaluating frequency of use and impact on workflow [12].
The purpose of this study was to apply the process mapping technique in an interdisciplinary approach in order to visualize, better understand, and efficiently organize percutaneous transluminal angioplasty (PTA) and stent placement procedures in a university hospital’s interventional radiology department.
Materials and methods
In a first step, seven well-established economic mapping techniques for visualizing and controlling processes were introduced to an interdisciplinary group in charge of providing interventional radiology services in a university hospital. The interdisciplinary group included referrers (physicians, nurses, and other staff in referring departments, e.g., vascular surgery), providers (interventional radiologists, nurses, technicians, and staff of the angiography suite), and specialists of the hospital’s controlling department. In a further step, one mapping technique (process mapping) was selected and applied to percutaneous transluminal angioplasty (PTA) and stent placement procedures in order to better visualize, better understand, and efficiently organize workflow.
Value stream mapping techniques
There are different sets and subsets of value stream mapping (VSM) techniques. These are often techniques individually adapted to specific problems. In general, authors have viewed their creations as answers to their specific problem rather than as generally applicable tools. Hines and Rich identified and characterized a total of seven different value stream mapping tools [13] that served as possible candidates for ameliorating percutaneous transluminal angioplasty (PTA) and stent placement procedures in the university hospital’s interventional radiology department:
-
1.
Process (activity) mapping
-
2.
Supply chain response matrix
-
3.
Production variety funnel
-
4.
Quality filter mapping
-
5.
Demand amplification mapping/Forrester effect mapping
-
6.
Decision point analysis
-
7.
Overall (physical) structure mapping (by volume or value)
The industrial origins of these tools (see Table 1) include engineering (1 and 5), action research/logistics (2 and 6), operations management (3), and two relatively contemporary tools (4 and 7). None of the tools was specifically developed for the hospital environment [13].
Process activity mapping
Process activity mapping (sometimes also more generally referred to as process mapping) is a technique for streamlining workflow. Process mapping in general refers to activities involved in defining exactly what a business entity does, who is responsible, to what standard a process should be completed, and how the success of a business process can be assessed. After successful process mapping there should be no uncertainty regarding the process.
This technique can be used to eliminate waste, inconsistencies, and irrationalities from the workplace while providing high-quality goods and services easily, quickly, and inexpensively. It is a general approach that includes five stages:
-
1.
Study of process flow
-
2.
Identification of waste
-
3.
Consideration of a better flow pattern
-
4.
Consideration of whether the process can be rearranged in a more efficient sequence
-
5.
Consideration of whether everything that is being done at each stage is really necessary (and what would happen if superfluous tasks were removed?)
Supply chain response matrix
This tool was first developed and applied in the time compression and logistics industry and is also known by a variety of different names (e.g., time-based process mapping). In the past decades it has gained increasing importance in the globalized textile supply chain industry. This mapping approach seeks to emphasize in a simple diagram the critical lead-time constraints for a particular process. In a horizontal plot the measurements of the product are shown both internally and externally. The vertical plot depicts the average amount of standing inventory at specific points in the supply chain. From supply chain response matrices individual lead times and inventory amounts can be identified and targeted for improvement activity.
Production variety funnel
This approach originates from operations management. The production variety funnel is also called IVAT analysis, which regards internal operations as conforming to I, V, A, or T shapes:
I plants consist of unidirectional, unvarying production of multiple identical items such as a chemical plant.
V plants consist of a limited number of raw materials processed into a wide variety of finished products in a generally diverging pattern. V plants are typical in textiles and metal fabrication industries.
A plants need many raw materials and have a rather limited range of finished products with different streams of raw materials using different facilities; these plants are commonly observed in the aerospace industry or in other major assembly industries.
T plants produce a rather large variety and combination of products from a rather restricted volume of components and resources. Semi-processing parts are often held ready for a wide range of customer-demanded final versions. T plants are characteristic of electronics and household appliance industries.
A graphical delineation using the production variety funnel allows the creator to understand how the company or the specific supply chain operates and how the accompanying complexity can be managed. In addition, production variety funnels can be used in inter-industry research to better understand similarities and differences or to transpose knowledge from one industry (where more research is conducted) to another with rather scarce research.
Quality filter mapping
This mapping technique is a rather new tool designed to identify where quality problems exist within a supply chain. The resulting map depicts three possible types of defects:
The first type is the “product defect.” Product defects are defined as defects in goods produced that are not caught by in-line or end-of-line inspections and are therefore passed on to customers.
The second type of quality defect can be termed “service defect.” Service defects are forwarded to a customer but they are not directly related to the product itself. The defect is rather the result of the accompanying level of service: major service defects can include inappropriate delivery (late or early) and incorrect documentation (e.g., instruction manuals). In general service defects summarize any problems customers may experience that are not due to production faults.
The third type of defect is often called “internal scrap.” Internal scrap refers to defects produced in a company that have been identified by in-line or end-of-line inspection. The inspection methods will vary and can include traditional product inspection, statistical process control, or poka-yoke (ポカヨケ, Japanese; method of preventing errors by putting limits on how an operation can be performed to force the correct completion of the operation).
Each type of defect can be mapped along the supply chain. The rate of defects is usually given on a vertical plot in parts per million (PPM) on an exponential scale.
Demand amplification mapping/Forrester effect mapping
This technique originates from the systems dynamics work of Forrester and Burbidge: The “Forrester effect” was first described in a Harvard Business Review article in 1958 [14]. This effect is linked primarily to delays and poor decision-making concerning information and material flow. The “Burbidge effect” is linked to what is now usually known as the “law of industrial dynamics,” which states:
“ …if demand for products is transmitted along a series of inventories using stock control ordering, then the demand variation will increase with each transfer” [15].
As a result, excess inventory, production, and capacity can generally be detected in unmodified supply chains. Furthermore, it is a known shortcoming of everyday business life that manufacturers are sometimes unable to satisfy retail demand even though on average they may produce more goods than they sell. In a supply chain setting it is therefore known that manufacturers seek to hold—in some cases voluminous—stocks to avoid this dilemma. The use of various mapping techniques loosely based on Forrester and Burbidge’s pioneering work is now quite common to overcome this shortcoming.
This simple analytic tool can be used to demonstrate how demand changes along the supply chain respective to time and procedural steps. This information can then be used for decision-making and further analysis to redesign the value stream configuration, manage and reduce fluctuation, or set up dual-mode solutions, where regular demand can be managed in one way and exceptional or promotional demand can be managed in a separate response pattern.
Decision point analysis
Decision point analysis is of particular use for “T” plants and for supply chains and industries that exhibit similar features. The decision point in the supply chain occurs where actual demand pull gives way to forecast-driven push. At this point, production is no longer related to forecasts.
Gaining an understanding of where in a supply chain this point may be located can be useful for two reasons:
-
1.
It is possible to access the processes that operate both downstream and upstream. Thus, one can ensure and control that they are adequately aligned with the relevant pull or push philosophy.
-
2.
From a long-term perspective, it is possible to design various “what if” scenarios to view the operation of the value stream if the decision point is moved. This allows a better design of the process itself.
Physical structure mapping
This rather new tool has been developed to elucidate what a particular supply chain looks like at an overview or industry level. This knowledge assists in appreciating industry-specific characteristics of processes in general and their realization in a business entity in particular.
Physical structure maps are widely applied in the automotive industry and are often a combination of two diagrams:
-
The first diagram depicts the structure of the industry according to the various ties that exist in both the supplier and the distribution area, with the assembler located in the center. This physical structure map provides an ample industry map that captures most firms involved, with the area of each part of the diagram proportional to the number of firms in each set.
-
The second diagram visualizes the industry in a similar way with the same sets of organizations. However, instead of linking the area of the diagram to the number of firms involved, it is directly linked to the value adding (VA) process (or more strictly to the cost-adding process).
Thus, physical structure analysis can be focused at the complete industry or supply chain structure. Analysis may result in a redesign of how the industry itself works. Attempts can be made to eliminate unnecessary activities, simplify or combine necessary but non-value-adding activities, and seek sequence changes that will reduce waste.
Applying the process mapping technique
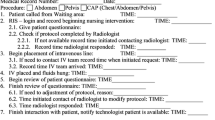
Two interdisciplinary meetings were conducted. Attendees included referrers (physicians, nurses, and other staff in referring departments, e.g., vascular surgery), providers (interventional radiologists, nurses, technicians, and staff of the angio suite), and specialists of the hospital’s controlling department. The staff involved chose to pursue the process activity mapping technique by reaching a consensus and agreeing that it would in their opinion be most suitable for the respective process analysis of treating peripheral arterial disease (PAD) patients with percutaneous transluminal angioplasty (PTA) and stent placement. In a first step, all participants provided information on the status quo process from patient admission to the hospital until discharge and final report generation. The unstructured information compiled on flip charts was then assembled chronologically and by executing staff (physicians, technicians, nurses, transportation). Each step was evaluated and discussed by the whole team, making suggestions on how to reduce waste and inefficiencies. Finally, the strived for ideal process of PTA and stent placement were created and visualized using the process mapping technique (Fig. 1).

Process map of PTA and stent placement in patients with PAD from admission to discharge. See glossary of icons for explanation of pictogram geometry
Results
The process map depicted in Fig. 1 describes the entire process for a patient who is a candidate for radiological intervention of PTA or stent treatment from admission to the department of vascular surgery until discharge after successful treatment. Henceforth, this visualization tool assists in better understanding (especially given natural staff fluctuation over time) and efficiently organizing the procedure in a generally binding and standardized fashion.
After admission of a patient with known or suspected PAD to the surgical ward, it is the responsibility of the university’s interdisciplinary vascular team (consisting of vascular surgeons, internists, and interventional radiologists as well as physicians of referring departments) to decide—after initial diagnostic angiography and other vascular examinations such as ultrasound, CT, and MRI—whether the patient qualifies for surgery or a PTA/stent procedure. In the latter case, it is the responsibility of the interventionalists of the angio suite to obtain patient consent 24 h in advance (unless emergency) and check all relevant medical data (patient identification, laboratory values, etc.). Technicians operating the angio suite are instructed by the interventionalists about all patients scheduled for the next day, schedules and priorities, and organize timely transportation (via an external in-house transportation service) to and from the angio suite accordingly, with the aim to ensure efficient workflow and maximum capacity utilization. The interventional radiologist performing the intervention determines how a patient is positioned (in relation to the preferred access) on the angiography table in advance, if possible. Upon arrival in the angio suite, the patient is transferred from the mobile bed onto the angiography table by nurses, technicians, and/or physicians. Nurses prepare the patient and the planned intervention including instrumentation and room requirements. Nurses and physicians independently identify the patient before the procedure. The medical procedure (PTA and/or stent implantation) is performed according to international medical standards. Hemostasis is achieved either by manual compression of the puncture site or by vascular closure devices. After treatment, patients are transported back to their referring wards. If wound check-up—generally 5 h (depending on puncture lumen) after the procedure—is unremarkable, the pressure bandage will be removed in the ward, a further clinical examination will take place, Doppler ultrasound will be performed, and the patient will receive lifelong anticoagulation prescription according to international medical standards before he or she is ready for hospital discharge. The interventionalist himself or herself usually informs the patient personally and the referring physician by digital enhanced cordless telecommunications (DECT) right after the procedure. If he or she has not generated a written medical report immediately after PTA/stent treatment, a medical resident can generate a central digital report. After supervision by the interventionalist, the digital written report is transmitted to the referring physician and ward, where it is accessible within the hospital’s IT system.
Apart from the advantage of visualizing the ideal process of PTA and stent placement, the interdisciplinary meeting assisted in stratifying common misconceptions and eradicating misunderstandings and miscommunications concerning steps carried out, especially by other staff involved in the process: By better understanding everybody else’s responsibilities in the process we were able to organize the process itself more efficiently.
Discussion
Process mapping is a structured activity modeling technique focused on defining the various decisions made and activities performed in the creation of an organization’s products or services. It is essential in identifying "what" work is being done and "how" that work is performed in order to successfully reduce waste.
To determine which tool is appropriate in a hospital’s environment it is important first to identify the specific processes to be reviewed. Second, through a series of preliminary interviews with clinicians and managers, one may identify various wastes and decide together which could and should be primarily targeted. In addition, it is useful to gain an economic understanding on the importance of the underlying industry structure, irrespective of the kind of wastes to be removed. This may be especially true in complex scenarios such as hospital organizations: to conceive an external supplier as an integral part of a value stream map may be especially challenging to understand for clinicians. It may be useful to reword the classic seven wastes identified by Toyota (waste of overproducing, waste of waiting, waste of transport, waste of processing, waste of inventory, waste of motion, waste of defects and spoilage) in more appropriate terminology for clinical use. For instance, in the healthcare industry the concept of industrial overproduction may not be exactly transferable. However, in calling this potential waste “doing things too early” this may assist in getting clinicians to relate the concept to their specific situation.
Table 2 depicts mapping tools and their estimated correlation and usefulness to the seven wastes in the Toyota production system as proposed by Hines and Rich [13]. In this regard the initial choice of the staff to pursue the process activity mapping technique to be suitable for the respective process analysis may be emphasized and regarded reasonable as probable clinical wastes like “waiting,” “transport,” “inappropriate processing,” and “unnecessary motion” all yield high correlation and usefulness in this scheme, whereas hardly controllable clinical wastes (by the group) yield medium (“unnecessary inventory”) or low correlation and usefulness (“overproduction” and “defects”).
While economic concepts, including Six Sigma and Lean Manufacturing, are increasingly applied in healthcare settings, some authors argue that there are significant gaps in the healthcare quality improvement literature and also only weak evidence that these tools actually and validly improve healthcare quality [16]. This is especially true because outcome is often difficult to measure due to many factors/variables that are being changed at the same time along with ever-changing sequences inside processes and staff fluctuation in every day practice. On the other hand, incremental changes in workflow processes can indeed have a significant impact on efficiency [17], and efforts should be undertaken to create smooth and efficient processes in healthcare whenever possible.
Limitations
This manuscript describes the implementation of a process mapping technique; it does not provide quantifiable data or an analysis of how the process mapping implementation affected interventions or patient care. Future work should concentrate on a before-and-after analysis of various quality measures using the process mapping technique for this clinical condition (PAD) in order to demonstrate an improvement in quality measures such as mortality, waiting times, and length of hospital stay.
References
Kaplan GS, Patterson SH (2008) Seeking perfection in healthcare. A case study in adopting Toyota Production System methods. Healthc Exec 23(16–8):20–1
Burkitt KH, Mor MK, Jain R et al (2009) Toyota production system quality improvement initiative improves perioperative antibiotic therapy. Am J Manag Care 15:633–42
Casey JT, Brinton TS, Gonzalez CM (2009) Utilization of lean management principles in the ambulatory clinic setting. Nat Clin Pract Urol 6:146–53
Pittsburgh regional healthcare initiative puts new spin on improving healthcare quality. Qual Lett Healthc Lead. 2002, Nov;14(11):2–11
Braaten JS, Bellhouse DE (2007) Improving patient care by making small sustainable changes: a cardiac telemetry unit’s experience. Nurs Econ 25:162–6
Printezis A, Gopalakrishnan M (2007) Current pulse: can a production system reduce medical errors in health care? Qual Manag Health Care 16:226–38
Rath F (2008) Tools for developing a quality management program: proactive tools (process mapping, value stream mapping, fault tree analysis, and failure mode and effects analysis). Int J Radiat Oncol Biol Phys 71:S187–90
Bertholey F, Bourniquel P, Rivery E, Coudurier N, Follea G (2009) [Work organisation improvement methods applied to activities of Blood Transfusion Establishments (BTE): Lean Manufacturing, VSM, 5S]. Transfus Clin Biol 16:93–100
Aakre KT, Valley TB, O’Connor MK (2010) Quality initiatives: improving patient flow for a bone densitometry practice: results from a Mayo Clinic radiology quality initiative. Radiographics 30:309–15
Rosen L (2004) Applying industrial engineering practices to radiology. Radiol Manage 26:32–5
Hart JL, McBride A, Blunt D, Gishen P, Strickland N (2010) Immediate and sustained benefits of a "total" implementation of speech recognition reporting. Br J Radiol 83:424–7
Lin A, Harris M, Zalis M (2010) Initial observations of electronic medical record usage during CT and MRI interpretation: Frequency of use and impact on workflow. AJR Am J Roentgenol 195:188–93
Hines P, Rich N (1997) The seven value stream mapping tools. Int J Op Prod Management 17:46–64
Forrester JW (1958) Industrial dynamics: a major breakthrough for decision makers. Harv Bus Rev 36:37–66
Burbidge JL (1984) Automated production control with a simulation capability; In: Proceedings of IFIP Conference WG
Dellifraine JL, Langabeer JR, Nembhard IM (2010) Assessing the evidence of six sigma and lean in the health care industry. Qual Manag Health Care 19:211–25
Fischman D (2010) Applying lean six sigma methodologies to improve efficiency, timeliness of care, and quality of care in an internal medicine residency clinic. Qual Manag Health Care 19:201–10
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Glossary of Icons
Pictograms Used for Process Mapping

Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
de Bucourt, M., Busse, R., Güttler, F. et al. Process mapping of PTA and stent placement in a university hospital interventional radiology department. Insights Imaging 3, 329–336 (2012). https://doi.org/10.1007/s13244-012-0147-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13244-012-0147-2