
Abstract
Aims and objectives
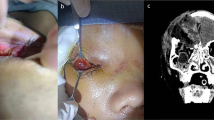
Diplopia in children is uncommon. However a small group of patients present with diplopia and severe restriction of upward globe movement which requires early diagnosis and prompt intervention. This study aims to evaluate the timing of intervention and functional outcome in the management of white-eyed blowout fractures.
Methodology
The study was conducted in a tertiary level trauma center. There were a total of 46 orbital floor injuries over a period of 2 years out of which 4 patients with white-eyed blowout fractures were identified. Details of each case were entered on a standard data base and analysed with respect to age, mode of injury, extent of limitation of gaze, timing of intervention, pre and post-operative diplopia. Minimum follow up period for every case was 1year.
Results
All of them had sports related injuries. Three of the four patients had complete recovery from diplopia with full range of eye movements. However one child with delayed presentation didn’t recover fully and had persistence of symptoms within the functional range.
Conclusion
White-eyed orbital blowout fracture in kids though uncommon need prompt diagnosis and management for complete recovery. The initial clinical presentation mimics that of head injury and hence can be missed, leading to a delay in diagnosis resulting in incomplete recovery.




Similar content being viewed by others


References
Zimmermann CE, Troulis MJ, Kaban LB (2006) Pediatric facial fractures: recent advances in prevention, diagnosis and management. Int J Oral Maxillofac Surg 35(1):2–13
Jordan DR, Allen LH, White J, Harvey J, Pashby R, Esmaeli B (1998) Intervention within days for some orbital floor fractures: the white-eyed blowout. Ophthalmic Plast Reconstr Surg 14(6):379–390
Kwon JH, Moon JH, Kwon MS, Cho JH (2005) The differences of blowout fracture of the inferior orbital wall between children and adults. Arch Otolaryngol Head Neck Surg 131:723–727
Ashurst J (1864) Injuries of the head. Am J Med Sci
Smith B, Regan WF Jr (1957) Blow-out fracture of the orbit: mechanism and correction of internal orbital fracture. Am J Ophthalmol 44(6):733–739
Nagasao T, Miyamoto J, Shimizu Y, Jiang H, Nakajima T (2010) What happens between pure hydraulic and buckling mechanisms of blowout fractures? J Craniomaxillofac Surg 38(4):306–313
Neinstein RM, Phillips JH, Forrest CR (2012) Pediatric orbital floor trapdoor fractures: outcomes and CT-based morphologic assessment of the inferior rectus muscle. J Plast Reconstr Aesthet Surg 65(7):869–874
Hammond D, Grew N, Khan Z (2013) The white-eyed blowout fracture in the child: beware of distractions. J Surg Case Rep 7:rjt54
Egbert JE, May K, Kersten RC, Kulwin DR (2000) Pediatric orbital floor fracture: direct extraocular muscle involvement. Ophthalmology 107(10):1875–1879
Smith B, Lisman RD, Simonton J, Della RR (1984) Volkmann’s contracture of the extraocular muscles following blowout fracture. Plast Reconstr Surg 74(2):200–216
Cope MR, Moos KF, Speculand B (1999) Does diplopia persist after blow-out fractures of the orbital floor in children? Br J Oral Maxillofac Surg 37(1):46–51
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Balaraman, K., Patnaik, J.S.S., Ramani, V. et al. Management of White-Eyed Blowout Fracture in the Pediatric Population. J. Maxillofac. Oral Surg. 20, 37–41 (2021). https://doi.org/10.1007/s12663-020-01393-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12663-020-01393-0