
Abstract
Introduction
Postoperative infectious complications are commonly encountered in open reduction and internal fixation (ORIF) of maxillofacial fractures. An early diagnosis of infectious processes is the key in preventing morbidity/mortality which could be in the form of loss of hardware and sepsis. To prevent these, various markers of inflammation have been studied in different disciplines of surgery but are found scarce in maxillofacial practice.
Material and method
The present study was designed to evaluate the perioperative variations in the levels of inflammatory markers. We analysed temperature, TLC, DLC, ALT, AST and CRP in 50 patients of ORIF. Their values were recorded preoperatively as well as at 24 h, 48 h, third day and seventh day postoperatively. The correlation of inflammatory markers with the type of anaesthesia and length of surgery were also analysed.
Results
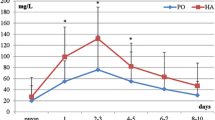
The ranges of various markers in the perioperative phase were: temperature (97.6 ºF–99.2 ºF), TLC (5100/mm3–18200/mm3), neutrophils (51–91%), AST (12–86 IU/L), ALT (12–96 IU/L) and CRP (1.2–150 mg/L). Mean values of all the inflammatory markers achieved their peak values within 24 h postoperatively. These values showed a decline thereafter, with the day 3 and day 7 values being even lower than their preoperative values. This fall in the values was highly significant (p < 0.001) except ALT where the fall was significant (p < 0.05). The data obtained could be used as a reference range by the surgeons for monitoring the recovery of the patient. It could also help in timely interception and expeditious management of an infectious episode in the postoperative phase.
Similar content being viewed by others


Change history
08 June 2020
The article Evaluation of the Variations in the Levels of Perioperative Inflammatory Markers After Open Reduction and Internal Fixation of Maxillofacial Fractures, written by Parveen Sharma, Rishi Kumar Bali, Avneet Kaur, Shivani Gaba and Guneet Dhillon.
References
Colley CM, Feleck A, Goode AW, Muller BR, Myers MA (1983) Early time course of the acute phase protein response in man. J Clin Pathol 36:203–207
Aono H, Ohwada T, Kaneko N, Fuji T, Iwasaki M (2007) The post-operative changes in the level of inflammatory markers after posterior lumbar interbody fusion. J Bone Jt Surg 89(11):1478–1481
Neumaier M, Scherer MA (2008) C-reactive protein levels for early detection of postoperative infection after fracture surgery in 787 patients. Acta Orthop 79(6):428–432
Niskanen RO, Korkala O, Pammo O (1996) Serum C-reactive protein after total hip and knee arthroplasty. J Bone Jt Surg 78-B:431–433
Durila M, Bronsky J, Harustiak T, Pazdro A, Pechova M, Cvachovec K (2012) Early diagnostic markers of sepsis after oesophagectomy (including thromboelastography). BMC Anaesthesiol 12:12
Giannoudis PV, Smith RM, Banks RE, Windsor AC, Dickson RA, Guillou PJ (1998) Stimulation of inflammatory response after blunt trauma. Br J Surg 85(7):986–990
Hussain M, Kim H (2002) C-reative protein and erythrocyte sedimentation rate in orthopaedics. Univ Penn Orthop J 15:13–16
Abtullah M, Olzem K, Polat G, Baddatodlu C, Colak M, Kuyuratar F (2004) Acute phase proteins after orthopaedic surgery. Clin Res 15:85–89
Aminzadeh A, Parsa E (2011) Relationship between age and peripheral white blood cell count in patients with sepsis. Int J Prev Med 2(4):238–242
Santucci A, Purcell T, Mejia C (2008) Leukocytosis as a predictor of severe injury in blunt trauma. West J Emerg Med 9(2):81–85
Milani TA, Rodrigues L, Chiattone C, Luz JG (2012) Changes in complete blood count in patients with surgically treated facial fractures. J Craniofac Surg 23(6):e587–e591. https://doi.org/10.1097/SCS.0b013e31826bf030
Deodhar SD (1989) C-reactive protein: the best laboratory indicator available for monitoring disease activity. Clevel Clin J Med 56(2):126–130
Fischer CL, Gill CW (1975) Acute-phase proteins. In: Ritzmann SE, Daniels JC (eds) Serum protein abnormalities: diagnostic and clinical aspects. Little, Brown and Co., Boston, pp 331–350
Morley JJ, Kushner I (1982) Serum C-reactive protein levels in disease. Ann N Y Acad Sci 389:406–417
Povoa P (2002) C-reactive protein: a valuable marker of sepsis. Int Care Med 28(3):235–243. https://doi.org/10.1007/s00134-002-1209-6
Barreto VT, Isaac A, Bhimidi P, Nguyen C, Jones G (2013) Trends of C-reactive protein laboratory values with white blood cell count levels in maxillofacial infections. Anesth Infect Pathol Med 71:e31
Kiran DN, Rajendra D (2012) Estimation of CRP associated with mandibular fracture. J Maxillofac Oral Surg 11(1):67–71
Gwak JM, Kim CH, Kim KW (2006) The changes of c-reactive prothin in the patients associated with mandibular fracture. Korean Assoc Maxillofac Plast Reconstr Surg 28(1):35–41
Gupta R, Singh R, Soni M (2002) C-reactive protein as an indicator of sepsis in orthopaedic trauma. Indian J Med Sci 56(10):501–507
Aalto K, Osterman K, Peltola H, Rasanen J (1984) Changes in erythrocyte sedimentation rate and C-reactive protein after total hip arthroplasty. Clin Orthop Relat Res 184:118–120
Larsson S, Thelander U, Friberg S (1992) C-reactive protein (CRP) levels after elective orthopedic surgery. Clin Orthop Relat Res 275:237–242
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethics Statement
The study design was approved by the Board of Studies of the University. An informed consent was obtained from all the patients.
Rights and permissions
About this article

Cite this article
Sharma, P., Bali, R.K., Kaur, A. et al. Evaluation of the Variations in the Levels of Perioperative Inflammatory Markers After Open Reduction and Internal Fixation of Maxillofacial Fractures. J. Maxillofac. Oral Surg. 20, 138–143 (2021). https://doi.org/10.1007/s12663-018-1174-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12663-018-1174-4