
Abstract
Purpose of Review
As adjuvant therapy for early-stage, hormone receptor-positive breast cancer has improved, late recurrences have become a significant issue. Endocrine therapies such as tamoxifen and aromatase inhibitors play a central role in reducing the risk of recurrence of hormone-positive breast cancers. However, the continued risk of breast cancer recurrence even with 5 years of adjuvant AI therapy has led to interest in extended therapy. This review intends to discuss and analyze recent trials that have reported results with extending AI therapy beyond 5 years of treatment.
Recent Findings
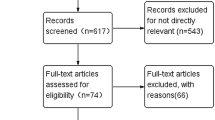
The IDEAL, DATA, and NSABP B-42 were unable to demonstrate a significant benefit in disease-free survival for extending aromatase inhibitor therapy beyond 5 years. They collectively demonstrate a decreased risk for contralateral breast cancers, as well as an increased risk for bone-related and cardiovascular toxicity.
Summary
There continues to be a lack of definitive evidence on the ideal length of adjuvant AI therapy. As certain subgroups may benefit more and experience less toxicity, selecting future patients based on clinicopathologic and genomic factors may maximize the benefit of extended adjuvant aromatase inhibitor therapy while minimizing harms.
Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
Stockwell S. Classics in oncology: George Thomas beatson m.d.(1848-1933). CA Cancer J Clin. 1983;33(2):105–7. doi:10.3322/canjclin.33.2.105.
Saphner T, Tormey DC, Gray R. Annual hazard rates of recurrence for breast cancer after primary therapy. J Clin Oncol. 1996;14(10):2738–46. doi:10.1200/JCO.1996.14.10.2738.
Colleoni M, Sun Z, Price KN, et al. Annual hazard rates of recurrence for breast cancer during 24 years of follow-up: results from the international breast cancer study group trials I to V. J Clin Oncol. 2016;34(9):927–35. doi:10.1200/JCO.2015.62.3504.
Fisher B, Dignam J, Bryant J, et al. Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor-positive tumors. J Natl Cancer Inst. 1996;88(21):1529–42.
Fisher B, Dignam J, Bryant J, Wolmark N. Five versus more than five years of tamoxifen for lymph node-negative breast cancer: updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J Natl Cancer Inst. 2001;93(9):684–90.
Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–16. doi:10.1016/S0140-6736(12)61963-1.
Goss PE, Strasser K. Aromatase inhibitors in the treatment and prevention of breast cancer. J Clin Oncol Off J Am Soc Clin Oncol. 2001;19(3):881–94. doi:10.1200/JCO.2001.19.3.881.
Hamilton A, Piccart M. The third-generation non-steroidal aromatase inhibitors: a review of their clinical benefits in the second-line hormonal treatment of advanced breast cancer. Ann Oncol. 1999;10(4):377–84. doi:10.1023/A:1008368300827.
Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet. 2002;359(9324):2131–9. doi:10.1016/S0140-6736(02)09088-8.
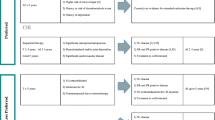
•• Goss PE, Ingle JN, Pritchard KI, et al. Extending aromatase-inhibitor adjuvant therapy to 10 years. N Engl J Med. 2016;375(3):209–19. doi:10.1056/NEJMoa1604700. The MA.17R trial randomized 1918 women who had completed about 5 years of AI therapy to 5 more years of AI vs. placebo. This trial was the first published major trial examining extended AI therapy and it demonstrated a significant improvement in DFS.
•• Mamounas EP, Bandos H, Lembersky BC, et al. A randomized, double-blinded, placebo-controlled clinical trial of extended adjuvant endocrine therapy with letrozole in postmenopausal women with hormone-receptor-positive breast cancer who have completed previous adjuvant treatment with an aromatase inhibitor. 2016 San Antonio Breast Cancer Symposium. Abstract S1-05. Presented December 7, 2016. The NSABP B-42 trial randomized 3923 women who had received 5 years of hormonal therapy to receive 5 years of AI or placebo and found no significant benefit in DFS or OS between the two arms.
•• Tjan-Heijnen VC, Van Hellemond IE, Peer PG, et al. First results from the multicenter phase III DATA study comparing 3 versus 6 years of anastrozole after 2–3 years of tamoxifen in postmenopausal women with hormone receptor-positive early breast cancer. 2016 San Antonio Breast Cancer Symposium. Abstract S1–03. Presented December 7, 2016. The DATA trial randomized 1912 women who had received 2–3 years of tamoxifen to receive either 3 or 6 years of AI therapy and found no significant benefit to doing so.
•• Blok EJ, Van de Velde CJH, Meershoek-Klein Kranenbarg EM, et al. Optimal duration of extended letrozole treatment after 5 years of adjuvant endocrine therapy. 2016 San Antonio Breast Cancer Symposium. Abstract S1-04. Presented December 7, 2016. The IDEAL trial randomized 1824 women who had received 5 years of any prior endocrine therapy to receive 2.5 years or 5 years of extended AI therapy and did not find a significant difference in DFS between the two arms.
Perez EA, Josse RG, Pritchard KI, et al. Effect of Letrozole versus placebo on bone mineral density in women with primary breast cancer completing 5 or more years of adjuvant Tamoxifen: a companion study to NCIC CTG MA.17. J Clin Oncol. 2006;24(22):3629–35. doi:10.1200/JCO.2005.05.4882.
Blok EJ. Poster P2-09-08: Safety assessment of extended adjuvant endocrine therapy with letrozole; results of the randomized phase III IDEAL trial (BOOG 2006–05). Poster presented at: 39th Annual San Antonio Breast Cancer Symposium; December 6–10, 2016; San Antonio, TX.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of Tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–26. doi:10.1056/NEJMoa041588.
Sestak I, Cuzick J, Dowsett M, et al. Prediction of late distant recurrence after 5 years of endocrine treatment: a combined analysis of patients from the Austrian breast and colorectal cancer study group 8 and Arimidex, Tamoxifen alone or in combination randomized trials using the PAM50 risk of recurrence score. J Clin Oncol. 2015;33(8):916–22. doi:10.1200/JCO.2014.55.6894.
Zhang Y, Schnabel CA, Schroeder BE, et al. Breast cancer index identifies early-stage estrogen receptor–positive breast cancer patients at risk for early- and late-distant recurrence. Clin Cancer Res. 2013;19(15):4196–205. doi:10.1158/1078-0432.CCR-13-0804.
Sgroi DC, Carney E, Zarrella E, et al. Prediction of late disease recurrence and extended adjuvant letrozole benefit by the HOXB13/IL17BR biomarker. JNCI J Natl Cancer Inst. 2013;105(14):1036–42. doi:10.1093/jnci/djt146.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Ojas H. Vyas declares that she has no conflict of interest.
Virginia Kaklamani has received personal fees from Novartis and Pfizer.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Clinical Trials
Rights and permissions
About this article

Cite this article
Vyas, O.H., Kaklamani, V.G. Evaluating the Role of Extended Aromatase Inhibitor Therapy in Early Hormone-Positive Breast Cancer. Curr Breast Cancer Rep 9, 183–187 (2017). https://doi.org/10.1007/s12609-017-0250-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12609-017-0250-y