
Abstract
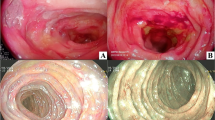
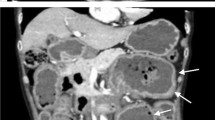
A 59-year-old woman presented to our hospital with a 6-month history of nausea, weight loss, and abdominal distension. Physical examination revealed abdominal distension without tenderness, and edema, numbness, and multiple peripheral neuropathy in the limbs. Blood test results showed anemia, hypoproteinemia, and hypoalbuminemia. Immunoelectrophoresis detected kappa-type Bence-Jones protein in both the serum and urine. Bone marrow examination did not reveal an increase of plasma cells. Computed tomography showed intestinal distension and retention of intestinal contents. No obstructive intestinal lesions were observed. Lower gastrointestinal endoscopy showed a decrease in the vascular visibility of the rectal mucosa. Histological findings showed amyloid deposition, which was positive for amyloid light-chain (AL) κ. Thus, she was diagnosed with chronic intestinal pseudo-obstruction (CIPO) due to gastrointestinal and neurological involvement of AL amyloidosis. Her abdominal symptoms were gradually improved by the insertion of an ileus tube and medication. Although we recommended chemotherapy for stopping her disease progression, she did not want to receive it. She died 1 year later because of her pneumonia. We should keep in mind that amyloidosis is an important cause of CIPO. Histopathological examination by endoscopic biopsy is required for exact diagnosis and appropriate treatment for CIPO due to amyloidosis.




Similar content being viewed by others

References
Dudley HA, Sinclair IS, McLaren IF, et al. Intestinal pseudo-obstruction. J R Coll Surg Edinb. 1958;3:206–17.
Stanghellini V, Cogliandro RF, de Giorgio R, et al. Chronic intestinal pseudo-obstruction; manifestations, natural history and management. Neurogastroenterol Motil. 2007;19:440–52.
Connor FL, Di Lorenzo C. Chronic intestinal pseudo-obstruction: assessment and management. Gastroenterology. 2006;130:29–36.
Sipe JD, Benson MD, Buxbaum JN, et al. Nomenclature 2014: amyloid fibril proteins and clinical classification of the amyloidosis. Amyloid. 2014;21:221–4.
Iida T, Yamano H, Nakase H. Systemic amyloidosis with gastrointestinal involvement: diagnosis from endoscopic and histological views. J Gastroenterol Hepatol. 2018;33:583–90.
Tada S, Iida M, Iwashita A, et al. Endoscopic and biopsy findings of the upper digestive tract in patients with amyloidosis. Gastrointest Endosc. 1990;36:10–4.
Lim AY, Lee JH, Jung KS, et al. Clinical features and outcomes of systemic amyloidosis with gastrointestinal involvement: a single-center experience. Korean J Intern Med. 2015;30:496–505.
Freudenthaler S, Hegenbart U, Schönland S, et al. Amyloid in biopsies of the gastrointestinal tract—a retrospective observational study on 542 patients. Virchows Arch. 2016;468:569–77.
Briggs GW. Amyloidosis. Ann Intern Med. 1961;55:943–57.
Yilmaz M, Unsal A, Sokmen M, et al. Duodenal biopsy for diagnosis of renal involvement in amyloidosis. Clin Nephrol. 2012;77:114–8.
Hayman SR, Lacy MQ, Kyle RA, et al. Primary systemic amyloidosis: a cause of malabsorption syndrome. Am J Med. 2001;111:535–40.
Milivojevic V, Stojanovic M, Rankovic I, et al. Multiple myeloma associated intestinal amyloidosis: intestinal pseudoobstruction falsely considered as an ascites. Rev Recent Clin Trials. 2018;13:79–81.
Leong RY, Nio K, Plumley L, et al. Systemic amyloidosis causing intestinal hemorrhage and pseudo-obstruction. J Surg Case Rep. 2014. https://doi.org/10.1093/jscr/rju087
Kim YJ, Kim HS, Park SY, et al. Intestinal amyloidosis with intractable diarrhea and intestinal pseudo-obstruction. Korean J Gastroenterol. 2012;60:172–6.
Liapis K, Michelis FV, Delimpasi S, et al. Intestinal pseudo-obstruction associated with amyloidosis. Amyloid. 2011;18:76–8.
Fonnesu C, Giovinale M, Verrecchia E, et al. Gastrointestinal amyloidosis: a case of chronic diarrhoea. Eur Rev Med Pharmacol Sci. 2009;13:45–50.
Hurlstone DP. Iron-deficiency anemia complicating AL amyloidosis with recurrent small bowel pseudo-obstruction and hindgut sparing. J Gastroenterol Hepatol. 2002;17:623–4.
Deguchi M, Shiraki K, Okano H, et al. Primary localized amyloidosis of the small intestine presenting as an intestinal pseudo-obstruction: report of a case. Surg Today. 2001;31:1091–3.
Kanai H, Kashiwagi M, Hirakata H, et al. Chronic intestinal pseudo-obstruction due to dialysis-related amyloid deposition in the propria muscularis in a hemodialysis patient. Clin Nephrol. 2000;53:394–9.
Hiramatsu K, Kaneko S, Shirota Y, et al. Gastrointestinal amyloidosis secondary to hypersensitivity vasculitis presenting with intestinal pseudoobstruction. Dig Dis Sci. 1998;43:1824–30.
Borczuk A, Mannion C, Dickson D, et al. Intestinal pseudo-obstruction and ischemia secondary to both beta 2-microglobulin and serum A amyloid deposition. Mod Pathol. 1995;8:577–82.
Fraser AG, Arthur JF, Hamilton I. Intestinal pseudoobstruction secondary to amyloidosis responsive to cisapride. Dig Dis Sci. 1991;36:532–5.
Tada S, Iida M, Yao T, et al. Intestinal pseudo-obstruction in patients with amyloidosis: clinicopathologic differences between chemical types of amyloid protein. Gut. 1993;34:1412–7.
Gertz MA. Immunoglobulin light chain amyloidosis diagnosis and treatment algorithm 2018. Blood Cancer J. 2018;8:44.
Westermark GT, Fändrich M, Westermark P. AA amyloidosis: pathogenesis and targeted therapy. Annu Rev Pathol. 2015;10:321–44.
Amiot A, Jolly F, Alves A, et al. Long-term outcome of chronic intestinal pseudo-obstruction adult patients requiring home parenteral nutrition. Am J Gastroenterol. 2009;104:1262–70.
Pironi L, Joly F, Forbes A, et al. Long-term follow-up of patients on home parenteral nutrition in Europe: implication for intestinal transplantation. Gut. 2011;60:17–25.
Rao AS, Camilleri M. Metoclopramide and tardive dyskinesia. Aliment Pharmacol Ther. 2010;31:11–9.
Emmanuel AV, Shand AG, Kamm MA. Erythromycin for the treatment of chronic intestinal pseudo-obstruction: description of six cases with a positive response. Aliment Pharmacol Ther. 2004;19:687–94.
O’Dea CJ, Brookes JH, Wattchow DA. The efficacy of treatment of patients with severe constipation or recurrent pseudo-obstruction with pyridostigmine. Colorectal Dis. 2010;12:540–8.
Emmanuel AV, Kamm MA, Roy AJ, et al. Randomised clinical trial: the efficacy of prucalopride in patients with chronic intestinal pseudo-obstruction—a double-blind, placebo-controlled, cross-over, multiple n = 1 study. Aliment Pharmacol Ther. 2012;35:48–55.
Ohkubo H, Fuyuki A, Arimoto J, et al. Efficacy of percutaneous endoscopic gastro-jejunostomy (PEG-J) decompression therapy for patients with chronic intestinal pseudo-obstruction (CIPO). Neurogastroenterol Motil. 2017. https://doi.org/10.1111/nmo.13127.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Tomoya Iida, Daisuke Hirayama, Gota Sudo, Kei Mitsuhashi, Hisayoshi Igarashi, Kentaro Yamashita, Hiroo Yamano, and Hiroshi Nakase declare that they have no conflict of interest.
Research involving human and/or animal participants
All procedures followed have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from this patient for being described in this case report.
Rights and permissions
About this article

Cite this article
Iida, T., Hirayama, D., Sudo, G. et al. Chronic intestinal pseudo-obstruction due to al amyloidosis: a case report and literature review. Clin J Gastroenterol 12, 176–181 (2019). https://doi.org/10.1007/s12328-018-0909-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-018-0909-6