
Abstract
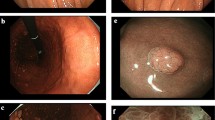
We experienced two cases of adenocarcinoma coexisting with a hyperplastic polyp arising from Helicobacter pylori-negative normal gastric mucosa. The first case was of a 59-year-old man. Esophagogastroduodenoscopy revealed a protruding lesion measuring 4 mm in diameter on the greater curvature of the middle gastric body. The second case was of a 47-year-old man. Esophagogastroduodenoscopy showed a protruding lesion measuring 5 mm located at the greater curvature of the upper gastric body. The absence of atrophic changes in the entire gastric mucosa was confirmed endoscopically in both cases. Multiple H. pylori tests were all negative. Endoscopically, these protruding lesions appeared as reddish, semipedunculated polyps. Hyperplastic polyps were suspected based on white light endoscopic findings. Magnified endoscopy with narrow band imaging could not predict the coexistence of cancer. However, histopathological examination of the resected specimen revealed focal cancer at the surface of the gastric hyperplastic polyps. Considering the possibility that cancer may be coexisting in polyps, when reddish polyps are detected in H. pylori-negative normal gastric mucosa, it is important to perform a biopsy, or a careful follow-up endoscopy.




Similar content being viewed by others


References
Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, Lyon, 7–14 June 1994. IARC Monogr Eval Carcinog Risks Hum. 1994;61:1–241.
Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345:784–9.
Shiota S, Murakawi K, Suzuki R, et al. Helicobacter pylori infection in Japan. Expert Rev Gastroenterol Hepatol. 2013;7:35–40.
Kitahara F, Kobayashi K, Sato T, et al. Accuracy of screening for gastric cancer using serum pepsinogen concentrations. Gut. 1999;44:693–7.
Yagi K, Nakamura A, Sekine A. Characteristic endoscopic and magnified endoscopic findings in the normal stomach without Helicobacter pylori infection. J Gastroenterol Hepatol. 2002;17:39–45.
Yagi K, Nozawa Y, Endou S, et al. Diagnosis of early gastric cancer by magnifying endoscopy with NBI from viewpoint of histological imaging: mucosal patterning in terms of white zone visibility and its relationship to histology. Diagn Ther Endosc. 2012;2012:954809. https://doi.org/10.1155/2012/954809.
Yamada A, Kaise M, Inoshita N, et al. Characterization of Helicobacter pylori-naïve early gastric cancers. Digestion. 2018;98:127–34.
Ono S, Kato M, Suzuki M, et al. Frequency of Helicobacter pylori-negative gastric cancer and gastric mucosal atrophy in a Japanese endoscopic submucosal dissection series including histological, endoscopic and serological atrophy. Digestion. 2012;86:59–65.
Matsuo T, Ito M, Takata S, et al. Low prevalence of Helicobacter pylori-negative gastric cancer among Japanese. Helicobacter. 2011;16:415–9.
Kakinoki R, Kushima R, Matsubara A, et al. Re-evaluation of histogenesis of gastric carcinomas: a comparative histopathological study between Helicobacter pylori-negative and H. pylori-positive cases. Dig Dis Sci. 2009;54:614–20.
Yamamoto Y, Fujisaki J, Omae M, et al. Helicobacter pylori-negative gastric cancer: characteristics and endoscopic findings. Dig Endosc. 2015;27:551–61.
Ueyama H, Yao T, Nakashima Y, et al. Gastric adenocarcinoma of fundic gland type (chief cell predominant type): proposal for a new entity of gastric adenocarcinoma. Am J Surg Pathol. 2010;34:609–19.
Yoshii S, Hayashi Y, Takehara T. Helicobacter pylori-negative early gastric adenocarcinoma with complete intestinal mucus phenotype mimicking verrucous gastritis. Dig Endosc. 2017;29:235–6.
Ozaki Y, Suto H, Nosaka T, et al. A case of Helicobacter pylori-negative intramucosal well-differentiated gastric adenocarcinoma with intestinal phenotype. Clin J Gastroenterol. 2015;8:18–21.
Jain R, Chetty R. Gastric hyperplastic polyps: a review. Dig Dis Sci. 2009;54:1839–46.
Miyamoto S, Kato M, Matsuda K, et al. Gastric hyperplastic polyps associated with proton pump inhibitor use in a case without a history of Helicobacter pylori infection. Intern Med. 2017;56:1825–29.
Markowski AR, Markowska A, Guzinska-Ustymowicz K. Pathophysiological and clinical aspects of gastric hyperplastic polyps. World J Gastroenterol. 2016;22:8883–91.
Coati I, Fassan M, Farinati F, et al. Autoimmune gastritis: pathologist’s viewpoint. World J Gastroenterol. 2015;21:12179–89.
Daibo M, Itabashi M, Hirota T. Malignant transformation of gastric hyperplastic polyps. Am J Gastroenterol. 1987;82:1016–25.
Zea-Iriarte WL, Sekine I, Itsuno M, et al. Carcinoma in gastric hyperplastic polyps. A phenotypic study. Dig Dis Sci. 1996;41:377–86.
Togo K, Ueo T, Yonemasu H, et al. Two cases of adenocarcinoma occurring in sporadic fundic gland polyps observed by magnifying endoscopy with narrow band imaging. World J Gastroenterol. 2016;22:9028–34.
Horiuchi H, Kaise M, Inomata H, et al. Magnifying endoscopy combined with narrow band imaging may help to predict neoplasia coexisting with gastric hyperplastic polyps. Scand J Gastroenterol. 2013;48:626–32.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human/animal rights
All procedures followed have been performed in accordance with the ethical standards laid down in the 1964 of Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from all patients being included in the study.
Rights and permissions
About this article

Cite this article
Isono, Y., Baba, Y., Mukai, K. et al. Gastric adenocarcinoma coexisting with a reddish semipedunculated polyp arising from Helicobacter pylori-negative normal gastric mucosa: a report of two cases. Clin J Gastroenterol 11, 481–486 (2018). https://doi.org/10.1007/s12328-018-0887-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-018-0887-8