
Abstract
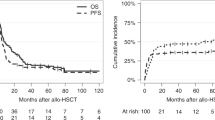
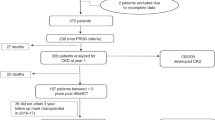
Creatinine clearance rate (Ccr) is a more accurate indicator of renal function than serum creatinine. Data are sparse regarding the prognostic value of renal impairment calculated using Ccr in patients who undergo allogeneic hematopoietic stem cell transplantation (allo-HSCT). We performed a retrospective analysis of 185 patients who underwent allo-HSCT. These patients were divided into two groups by Ccr (ml/min) before transplantation; one showed normal renal function (Ccr ≥ 60, n = 156) and the other showed mild renal dysfunction (30 ≤ Ccr < 60, n = 29), and transplant outcomes were compared between the groups. We observed no significant difference between the groups in terms of clinical characteristics other than age, estimated glomerular filtration rate, serum creatinine, Ccr predicted by Cockcroft–Gault formula, primary disease, and conditioning intensity. With respect to transplant outcomes, no significant difference was observed in overall survival, relapse, or non-relapse mortality between the two groups. Multivariate analysis demonstrated that 30 ≤ Ccr < 60 before allo-HSCT was not an independent prognostic factor for transplant outcome. In conclusion, these results suggest that patients with mild renal dysfunction, defined as 30 ≤ Ccr < 60 ml/min, can safely undergo allo-HSCT. However, a larger series of patients is needed to evaluate the impact of mild renal dysfunction before allo-HSCT in more detail.



Similar content being viewed by others
References
Yanada M. Allogeneic hematopoietic cell transplantation for acute myeloid leukemia during first complete remission: a clinical perspective. Int J Hematol. 2015;101:243–54.
Sorror ML, Maris MB, Storb R, Baron F, Sandmaier BM, Maloney DG, et al. Hematopoietic cell transplantation (HCT)-specific comorbidity index: a new tool for risk assessment before allogeneic HCT. Blood. 2005;106:2912–9.
Heher EC, Spitzer TR. Hematopoietic stem cell transplantation in patients with chronic kidney disease. Semin Nephrol. 2010;30:602–14.
Sorror ML, Giralt S, Sandmaier BM, De Lima M, Shahjahan M, Maloney DG, et al. Hematopoietic cell transplantation specific comorbidity index as an outcome predictor for patients with acute myeloid leukemia in first remission: combined FHCRC and MDACC experiences. Blood. 2007;110:4606–13.
Swedko PJ, Clark HD, Paramsothy K, Akbari A. Serum creatinine is an inadequate screening test for renal failure in elderly patients. Arch Intern Med. 2003;163:356–60.
Inoue N, Watanabe H, Okamura K, Kondo S, Kagami S. Are the equations for the creatinine-based estimated glomerular filtration rate applicable to the evaluation of renal function in Japanese children and adult patients receiving chemotherapy? Clin Exp Nephrol. 2015;19:298–308.
Oshima K, Kanda Y, Nanya Y, Tanaka M, Nakaseko C, Yano S, et al. Allogeneic hematopoietic stem cell transplantation for patients with mildly reduced renal function as defined based on creatinine clearance before transplantation. Ann Hematol. 2013;92:255–60.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, et al. 1994 Consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15:825–8.
Shingai N, Morito T, Najima Y, Kobayashi T, Doki N, Kakihana K, et al. Early-onset acute kidney injury is a poor prognostic sign for allogeneic SCT recipients. Bone Marrow Transplant. 2015;50:1557–62.
Kersting S, Verdonck LF. Successful outcome after nonmyeloablative allogeneic hematopoietic stem cell transplantation in patients with renal dysfunction. Biol Blood Marrow Transplant. 2008;14:1312–6.
de Souza JA, Saliba RM, Patah P, Rondon G, Ribeiro R, de Padua Silva L, et al. Moderate renal function impairment does not affect outcomes of reduced-intensity conditioning with fludarabine and melphalan for allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15:1094–9.
Ikegame K, Yoshida T, Yoshihara S, Daimon T, Shimizu H, Maeda Y, et al. Unmanipulated haploidentical reduced-intensity stem cell transplantation using fludarabine, busulfan, low-dose antithymocyte globulin, and steroids for patients in non-complete remission or at high risk of relapse: a prospective multicenter phase I/II study in Japan. Biol Blood Marrow Transplant. 2015;21:1495–505.
Bodge MN, Reddy S, Thompson MS, Savani BN. Preparative regimen dosing for hematopoietic stem cell transplantation in patients with chronic kidney disease: analysis of the literature and recommendations. Biol Blood Marrow Transplant. 2014;20:908–19.
Terakura S, Wake A, Inamoto Y, Murata M, Sakai R, Yamaguchi T, et al. Exploratory research for optimal GvHD prophylaxis after single unit CBT in adults: short-term methotrexate reduced the incidence of severe GvHD more than mycophenolate mofetil. Bone Marrow Transplant. 2017;52:423–30.
Lee JH, Joo YD, Kim H, Ryoo HM, Kim MK, Lee GW, et al. Randomized trial of myeloablative conditioning regimens: busulfan plus cyclophosphamide versus busulfan plus fludarabine. J Clin Oncol. 2013;31:701–9.
Jo T, Arai Y, Kondo T, Kitano T, Hishizawa M, Yamashita K, et al. Chronic kidney disease in long-term survivors after allogeneic hematopoietic stem cell transplantation: retrospective analysis at a single institute. Biol Blood Marrow Transplant. 2017;23:2159–65.
Acknowledgements
We are very grateful to the patients in the current study. The authors would like to thank the nursing staff at our institution.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
About this article

Cite this article
Ikegawa, S., Matsuoka, Ki., Inomata, T. et al. Mild renal dysfunction defined by creatinine clearance rate has limited impact on clinical outcomes after allogeneic hematopoietic stem cell transplantation. Int J Hematol 107, 568–577 (2018). https://doi.org/10.1007/s12185-017-2398-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-017-2398-7