
Abstract
In healthcare industry, the phenomenon of Industry 4.0 is popular as Health 4.0 where the modern technologies are integrated with available data along with the use of artificial intelligence. The main objective of this paper is to explore the barriers of Health 4.0 application in healthcare sector in India. Fifteen barriers which can affect the adoption of Health 4.0 in the Indian healthcare sector have been identified through extensive literature review and opinions of healthcare industry and academic experts. A TISM (Total Interpretive Structural Modelling) model has been developed to extract the key barriers influencing Health 4.0 adoption which will guide the healthcare managers and decision makers to explore the effect of each barrier on other barriers as well as the degree of relationships among them. The result shows that lack of top management support, exclusive and skilled workforce requirement, inadequate maintenance support systems and political support are the major barriers as they have strong driving power. Timely action taken by the management to remove these hurdles will not only reduce the cost of medical procedures but also improve the quality of treatment so that the true potential of Health 4.0 can be utilized.
Similar content being viewed by others



1 Introduction
The Industrial Revolution is considered to be one of the most significant landmark in the history which impacted all the aspects of life in one way or the other. Technological advancements and industrialization led to the development of highly automated and motorized manufacturing processes giving rise to evolution of factory system Kamble et al. (2018). The first industrial revolution occurred with the invention of steam engine by Thomas Newcomen in the late eighteenth century which led to the use of steam to make machines causing the development of textile, coal and iron industry. This resulted in urbanization and increased communications and people moved to those cities where they could work as operators in factories. To provide accommodation to these people, houses of cheaper quality were built and community wells were the only source of drinking water. Facilities for sewage removal were hardly present. This led to the deterioration of health and spread of diseases like typhoid, cholera, tuberculosis, fever, smallpox and plague etc. Side by side many medical innovations were made due to advancement in science and technology and scientific causes of some diseases were explored. In 1796, Edward Jenner was successful in developing smallpox vaccination. Before this, there was no awareness about the causes of spread of diseases and remedies were dependent upon several superstitions and speculations. In the 1850s, Louis Pasteur discovered that the causes of disease were microorganisms. Healthcare industry in that era witnessed the inception of modular information system technologies and that period was known as Health 1.0 (Bodenheimer 1995; Thuemmler and Bai 2017). Second industrial revolution was another transition in technology focussing on the extensive use of electrical energy, petroleum and steel for creating mass production. Improved factories and contemporary technologies gave rise to the discovery of microscopes and other medical equipment. Simple networking was introduced in healthcare industry with the evolution of Electronic Health Records (EHR) which were integrated with medical imaging techniques providing better diagnosis of diseases. This was termed as Health 2.0 (Thuemmler and Bai 2017). During third industrial revolution, there was intensive computerization and digitalization. Digitalization was a major driver for healthcare industry with the capacity to restructure patient landscape. There was emergence of new business models in healthcare where healthcare managers used to collect data from various sources and relevant and significant information was extracted. This decade observed the use of genetic information and development of implants and wearables. The integration and networking of this data with EHR processes was marked as Health 3.0 (Bodenheimer 1995; Gray 2008; Thuemmler and Bai 2017). The fourth industrial revolution (identified as Industry 4.0) is characterized by amalgamation of technologies from physics, biology and information technology (Acemoglu 2002; Von Tunzelmann 2003). Industry 4.0 initially took place in Germany with a mission to create smart industries with the use of new advanced IT technologies such as big data analytics, cloud computing, virtual reality, internet of things, additive manufacturing and robotics etc. to create cyber-physical systems (CPS) in different sectors including healthcare. This is attained with the interaction and networking of various components of the processes and practically generate value reinforced by cyber physical technology, human-equipment interaction and novel business frameworks. In healthcare industry, this phenomenon of Industry 4.0 is also popular as Health 4.0 where all modern technologies described above are integrated with available data along with the use of artificial intelligence (Thuemmler and Bai 2017). Health 4.0 have made healthcare sector more collaborative, convergent and predictive. Now large amount of information is available to the doctors online which allows easy portability of data which can be accessed anywhere anytime by the healthcare professionals. Industry 4.0 is basically based upon nine pillars which are described in Table 1 (Qin et al. 2016; Rüßmann et al. 2015).
Industry 4.0 can point out the areas where there is scope for improvement thereby making decision process more informative and innovative. It has the ability to transform healthcare sector from a focussed and compassionate system to a value oriented system which can ensure proactive preventive measures. Department of Health has already started implementing Industry 4.0 concept in United States, where it has been declared that within a year 90% of Medicare would be converted into value based framework. Though the Indian healthcare sector is expanding rapidly and is expected to reach 280 billion US Dollars by the year 2020, yet it is highly fragmented (Raghupathi and Raghupathi 2014). A detailed comparison between Indian Healthcare industry today and by 2020 is depicted in the Fig. 1.

Indian Healthcare industry today and by 2020 Rudrappa et al. (2019)
Industry 4.0 is the most advanced concept that has the capability to change the future of Indian healthcare sector if implemented judiciously and cautiously.
2 Review of literature
Literature review is divided into two sections. In the first section, literature on Industry 4.0 and its technologies in different industries are presented. In the second section, researches regarding the application of Industry 4.0 in healthcare industry are reviewed.
2.1 Industry 4.0 and its technologies
Industry 4.0 technologies are being widely used in manufacturing and automation sector. Kagermann et al. (2011) firstly explained the elementary concepts of Industry 4.0 and laid the basis of this emerging phenomenon. Authors identified Germany as a leading country in manufacturing sector where Industry 4.0 can be best implemented and physical world is blended with virtual world creating smart factories. In 2018, Kamble et al. identified twelve barriers which can hamper the manufacturing industries to implement Industry 4.0. Interpretive Structural Modelling approach was used to identify the interactive relationships among these barriers and a framework was developed so that Industry 4.0 can be implemented successfully (Kamble et al. 2018). Cao et al. in 2017 established the use of cloud computing in supply chain management (Cao et al. 2017). Holmstrom et al. indicated in their research that 3D printing offers a number of opportunities for innovations in products and processes and has revolutionized manufacturing industry along with their supply chains structures (Holmström et al. 2016). In 2016, Harrison et al. reviewed certain engineering techniques adopted for Industry 4.0. Authors conducted a case study on the applications of cyber physical system toolkit innovated at a university in United Kingdom that how it can support automation systems (Harrison et al. 2016). Also, Bahrin et al. reviewed the role of robotic and automation technologies in attaining Industry 4.0 (Bahrin et al. 2016). Bagheri et al. in their study constructed a model where CPS can be integrated in the manufacturing sector. It was stated that CPS are aimed to detect the information and explained “adaptive cluster” in detail for data analysis (Bagheri et al. 2015). Zhou et al. in their research introduced important technologies and several opportunities and challenges of Industry 4.0 in China. The study shows that for Industry 4.0 to be successful, China requires innovations in technology, knowledge and management with regard to manufacturing sector (Zhou et al. 2015). In 2015, Shafiq et al. defined cyber physical systems as “the conjunction of the physical and digital worlds by creating global networks for businesses that integrate their technology, warehousing systems, and production facilities”. Digitization of physical systems is done to manage their operations (Shafiq et al. 2015). Deane et al. in 2009 discussed about management of supply chains risks and disruptions from IT security incidents (Deane et al. 2009). Besides this other industries have also started adopting Industry 4.0 technologies. In 2014 Lasi et al. discussed different key technologies and explored various driving forces for the Industry 4.0 concept (Lasi et al. 2014). Mueller et al. discussed the requirement and challenges of implementation of Industry 4.0 with special emphasis on cyber physical systems. The paper helps in understanding the theoretical concepts of Industry 4.0. Results of the study show that frameworks based on CPS help the industries to attain proper control over smart machineries. On the other hand, there are some challenges like data security, maintenance issues which need to be overcome (Mueller et al. 2017). In 2016, Harrison et al. reviewed certain engineering techniques adopted for Industry 4.0. Authors conducted a case study on the applications of cyber physical system toolkit innovated at a university in United Kingdom that how it can support automation systems (Harrison et al. 2016).
2.2 Literature review on health 4.0
In 2017 Thuemmler and Bai described in their book how advanced digital services and big data analytics are having a significant impact on healthcare industry and the fourth industrial revolution in healthcare is called as Health 4.0. The authors have narrated that the technological drivers of Industry 4.0 i.e. artificial intelligence, cloud computing, automated robots and cyber physical systems are bringing a major change in working style of industrial systems which is also affecting healthcare domain due to which even clinical care can be provided virtually outside the hospitals. Now patients can also keep a track of their health conditions with the help of smart devices based on data analytics (Thuemmler and Bai 2017). Manogaran et al. explored the role of sensor tailored wearable medical devices in providing information about our physical and psychological health. These sensors generate extensive data which is commonly called as Big data. A new and secure “Cloud- Redirection (MC-R) architecture” has been proposed to analyse the data generated by the sensors like heart rate, blood pressure, blood sugar level and pulse rate for healthcare processes. If any of these parameters exceeds its normal value, a warning message is sent to the physician with the help of wireless networks (Manogaran et al. 2017). Filipe et al. reviewed the contributions of “Wireless Body Area Networks (WBANs)” for various healthcare applications to monitor clinical parameters (Filipe et al. 2015). In 2014, Bates et al. analysed the role of big data analytics for the management of high cost and high risk patients. The authors discussed how different data analytical techniques like algorithms and monitoring systems can reduce costs and improve clinical outcomes (Bates et al. 2014). Chawla and Davis 2013 presented a framework with the help of which Big data can be utilized for patient oriented outcomes so that patient readmission rates can be reduced (Chawla and Davis 2013). Jee and Kim conducted a study to explore how big data applications can be used for reshaping the healthcare sector. Various opportunities and challenges brought about by big data are also discussed. The study concludes that data security is one of the major challenge which should be handled with utmost care and a structured approach is required for the management and integration of big data (Jee and Kim 2013). In 2011, Kumar and Lee conducted a survey to explore the critical issues like data security and confidentiality in healthcare programs using “Wireless Medical Sensor Networks (WSMNs)”. They highlighted security issues in some well-known projects which were using WSMN technology. It was concluded that a well-designed security system is required for successful implementation of these wireless technologies and people will believe in a technology only if it is feasible, safe and practical (Kumar and Lee 2011). Lorincz et al. also explored the use of sensor networking technology in emergency clinical and disaster responses. The authors brought about certain challenges faced by the healthcare managers and concluded that a common digitized framework is required for integrating different devices so that better response can be provided for medical emergency and disaster management (Lorincz et al. 2004).
All the studies stated above show that though Industry 4.0 applications are being used in healthcare sector, still in India, only few large super speciality healthcare chains are trying to adopt Industry 4.0. Majority of healthcare organizations are still doubtful about its implementation because of excess investment in terms of infrastructure, training and policies (Kagermann 2015). Therefore, it is very important to explore the barriers of Industry 4.0 implementation in healthcare industry in India so that it can be implemented successfully and organizations can avail maximum benefit of this emerging phenomenon.
The objectives of this paper are as under:
-
1.
To explore the barriers of Industry 4.0 application in healthcare sector in India and to identify mutual relationship among these barriers.
-
2.
To compute the driving power and dependence power of these barriers using MICMAC i.e.
Matrice d’Impacts croises-multipication applique´ an classment (Impact Matrix Cross-Reference Multiplication Applied to Classification) analysis in order to rank them in order of priority so that they can be handled successfully.
-
3.
To develop a comprehensive structured model using TISM (Total Interpretive Structural Modelling) methodology to overcome these barriers.
3 Research methodology
3.1 Delphi technique to identify the barriers to adoption of health 4.0
Health 4.0 is an advanced concept where large number of elements incorporating industrial processes are amalgamated with internet networking technologies resulting in smart hospitals ahead. New innovations in healthcare industry and Industry 4.0 technologies promise to generate value added services. In a developing country like India, there is extensive digital divide between urban and rural areas and rural population is devoid of even basic healthcare facilities. Health 4.0 technologies like telemedicine, robotics can resolve this issue. But in India this revolution is still in its nascent stage. Health 4.0 has the potential to change the future of Indian healthcare industry. But there are certain barriers like cybersecurity, legal implications, non-standardized data which need to be addressed cautiously, otherwise real potential of Health 4.0 can never be attained. In order to identify the barriers which can affect the implementation of Health 4.0 in India we adopted an extensive review of existing literature and viewpoints of experts from healthcare and academic sector. Initially, articles published on Health 4.0, Industry 4.0 in healthcare and technologies of Industry 4.0 in peer reviewed journals, reports from the industry, newspaper and magazine articles were explored and 20 barriers were identified. After this, Delphi technique was performed in which a team of fifteen experts from the relevant areas were taken for validation of the barriers. Six doctors, five healthcare IT experts and four academicians having knowledge of Industry 4.0 applications were selected for this purpose from the hospitals of Delhi and NCR (Near Capital Regions). Previous researches show that ten to thirty experts are appropriate for carrying out Delphi technique in qualitative studies (Murry Jr and Hammons 1995). Finally after few rounds of Delphi, fifteen barriers appropriate for Indian healthcare sector were selected. These fifteen barriers are described in Table 2.
3.2 TISM methodology
TISM starts with establishing contextual relationships among different factors explored from the review of literature and expert’s perspective (Jain and Raj 2016). TISM methodology was defined by Sushil (Sushil 2012a) and is derived from the concept of ISM methodology which was suggested by Warfield in 1973 (Warfield 1973). In TISM, complicated systems are interpreted and represented graphically (Sushil 2012b). ISM proposes the interrelationships among different factors which is further depicted in the form of a diagraph. TISM may also be referred as the advanced version of ISM and some studies have been conducted using this technology (Ajmera and Jain 2019a; Dubey and Ali 2014; Jain and Ajmera 2018; Jain and Raj 2014; Nasim 2011). TISM expresses direct and transitive relationships among different elements so that structured model can be interpreted also. TISM has been used in various areas like e-governance (Nasim 2011), Flexibility dimensions (Dubey and Ali 2014), education (Mahajan et al. 2016), performance management (Yadav 2014; Yadav et al. 2015), flexible manufacturing systems (Jain and Raj 2015; Jain and Soni 2019), organization excellence (Agarwal and Vrat 2015), quality of life in diabetic patients in India (Ajmera and Jain 2019b) and supply chain (Dubey et al. 2017). TISM has been used in higher private technical education (Prasad and Suri 2011) to analyze the relationships among different strategic performance management factors for exploring the best strategy (Kumar Srivastava and Sushil 2014). TISM has been used to identify various enablers in order to enhance sustainability of integrated logistics in an environment having uncertainty (Mohanty and Shankar 2017). Khatwani et al. also suggested TISM methodology for group decision making process (Khatwani et al. 2015).
Subsequent steps of TISM methodology are explained below: (Flow diagram is shown in Fig. 2)
-
1.
Identify the barriers.
-
2.
Interpret the interrelationships between the barriers. Apart from indicating whether ‘element A will influence/ enhance element B’ or not, it also explains ‘how and in what way they will influence/ enhance each other’. It is depicted in Table 3.
-
3.
Construction of Structural self-interaction (SSIM) matrix:

Flow diagram of TISM Methodology
Taking into account the circumstantial relationships, the interaction between two elements (i and j) is determined by relevant experts. The symbols used to determine the interaction between any two factors are V, A, X, and O.
The use of symbols in SSIM has been explained in the Table 4.
-
4.
Development of Reachability Matrix (RM):
This is established by converting information within SSIM into binary digits of 1 and 0 criteria which is also depicted in Table 4 above.
-
5.
Transitivity Check
Transitivity is checked in the matrix rule and incorporated wherever required.
-
6.
Reachability Matrix Partition
The partitioning of reachability matrix is performed on different sets and subsets of the elements. A conical matrix is developed from final reachability matrix. The drive power of a barrier is derived by summing up the number of ones in the rows and its dependence power by summing up the number of ones in the columns. Clusters of barriers affecting the barriers of healthcare 4.0 is developed from the conical matrix.
-
7.
Developing Digraph and TISM model
After checking for transitivity, digraph is created by identifying different levels of elements. This diagraph depicts hierarchy barriers. After this, final TISM model is constructed where all transitive and the direct influencing links are incorporated. Besides this, interpretation of relationships is also included to provide a proper explanation about the impact of one barrier on other.
4 Modelling the barriers to the adoption of health 4.0 by TISM
Different steps to do the modelling of barriers to the adoption of Health 4.0 by TISM are given below:
-
1.
Delphi technique - In the present research, the viewpoints of 15 professional experts (10 from healthcare industry and 5 from academia) were considered for analysis of relationship among criteria.
-
2.
Selection of the barriers of Health 4.0 in the healthcare industry in India. Fifteen barriers were selected as described in the previous section.
-
3.
Collection of responses and development of SSIM Matrix
In the present work, opinions of fifteen experts who have thorough understanding of the problem and have adequate experience in handling such problems were taken. Initial SSIM matrices were developed taking into account responses of all the experts based on the degree of interrelationship between the criteria.
-
4.
Computation of SSIM and Final Reachability Matrix
Table 5 Depicts the values of SSIM matrix. SSIM is converted into binary digits of 1 and 0 criteria as shown below
Symbol | Illustration | Binary digit in initial RM | ||
(i,j) entry in matrix | (j,i) entry in the matrix | |||
V | If factor i influences or reaches to factor j | 1 | 0 | |
A | If factor j influences or reaches to factor i | 0 | 1 | |
X | If both factors i and j influence each other | 1 | 1 | |
O | For no relation between two factors | 0 | 0 | |
Initial reachability matrix is shown in Table 6.
-
5.
The matrix is reviewed for the transitivity links as depicted in Table 7 as final reachability matrix.
The matrix is then partitioned and the levels of different iterations are presented in Table 8.
A conical matrix is developed from final reachability matrix. It is shown in Table 9. Clusters of barriers affecting the barriers of healthcare 4.0 is developed from the conical matrix and shown in Fig. 3.
-
6.
Graphical representation of the barriers in different levels is done and the directed links are introduced taking into account the interrelationships according to the reachability matrix. The significant transitive mutual relationships are shown in Fig. 4.
-
7.
The final digraph is transformed into a binary interaction matrix and interpretive matrix and the interpretations of the barriers demonstrated in Tables 10 and 11.
-
8.
TISM is derived from the connective and interpretive information demonstrated in the interpretive direct interaction matrix and digraph which is displayed in Fig. 5. Interpretations of the barriers are discussed in Table 11.
Table 9 Conical matrix Fig. 3 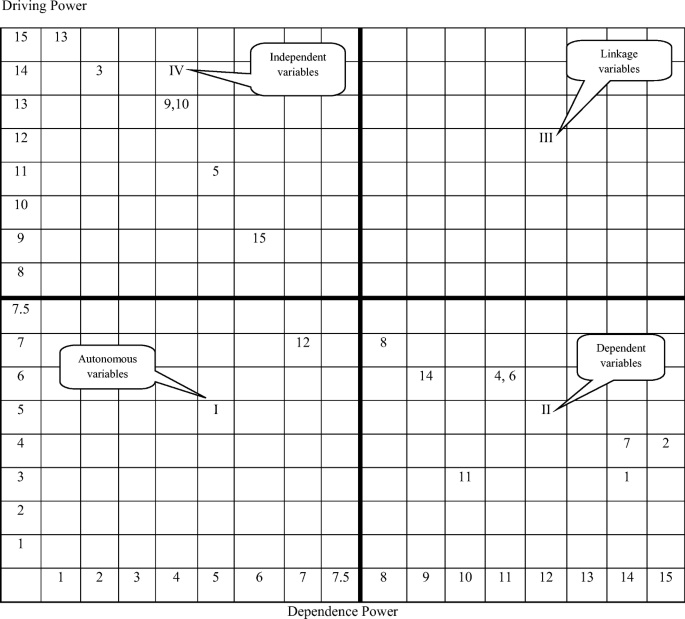
Clusters of barriers affecting the barriers of healthcare 4.0
Fig. 4 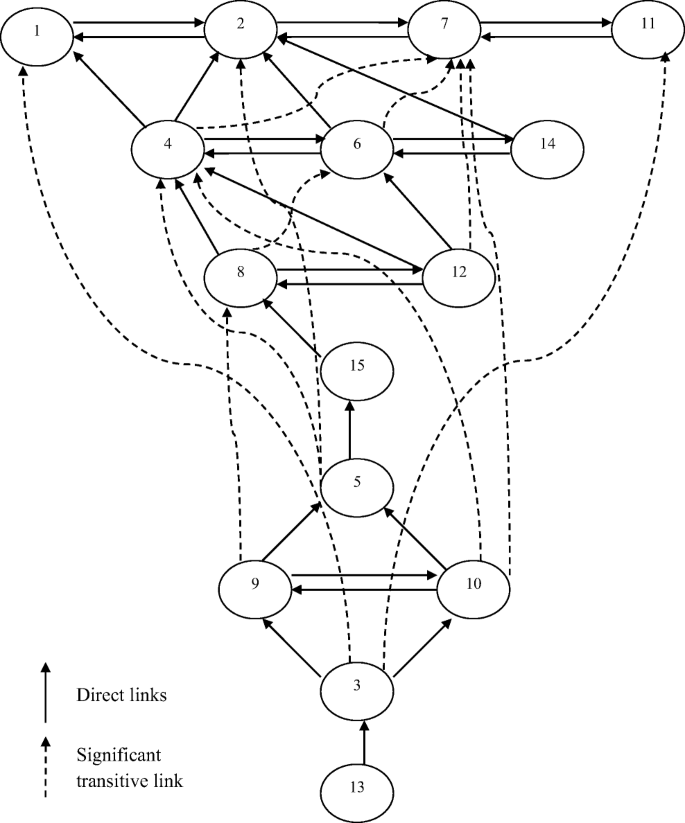
Diagraph with significant transitive links
Table 10 Interaction matrix Table 11 Barriers contextual relationship with interpretation Fig. 5 
Total interpretive structural model showing the levels of barriers



5 Data analysis and results
MICMAC analysis is conducted to explore and map the barriers of Health 4.0 in the Indian healthcare sector according to their drive and dependence powers shown in Table 8 as a conical matrix. These barriers are then classified into four groups i.e. autonomous, dependent, linkage and independent using MICMAC analysis.
-
(a)
Group 1 barriers (Autonomous): These barriers are placed in the first quadrant and have weak drive and dependence powers. In the present work, “Lack of digital strategy and resource scarcity (BH 12)” lie in this quadrant.
-
(b)
Group 2 barriers (Dependent): These barriers have strong dependence power but weak driving power. They lie in the second quadrant and are influenced by various other barriers. In this research, “Job disruption risk (BH1), Extensive capital requirement (BH2), Cybersecurity and privacy issues (BH4), Intellectual property issues (BH 6), Non uniform regulations for clinical information exchange (BH7), Legal Implications regarding external data use (BH8), Lack of R & D clusters (BH11) and Fragmented and non- standardized clinical data (BH14)” represent this quadrant.
-
(c)
Group 3 barriers (Linkage): These barriers possess strong driving as well as dependence power. They are unsteady and very important and any activity with them will have a direct influence on others and also have feedback effect upon them. In this research no barrier lies in this quadrant.
-
(d)
Group 4 Barriers (Independent): They lie in fourth quadrant and have strong driving power but weak dependence power. “Exclusive and skilled workforce requirement (BH3), Insufficient compendious IT infrastructure (BH5), Inadequate maintenance support system (BH9), Political support (BH 10), Lack of top management support (BH13), Apprehension about IoT use (BH15)” lie in this quadrant.
Results of the present work depict that “Lack of top management support” is the major barrier to the successful adoption of Health 4.0 in Indian healthcare industry as this barrier has very high driving power. Successful adoption of Health 4.0 in in India depends upon top management support to a large extent as this barrier has very high driving power. Health 4.0 requires extensive initial investment to develop and maintain appropriate infrastructure in the organizations. Also, additional cost is required for the training of the workforce and maintenance of support systems. All the major decisions are taken by top management. If top management is not supportive, Health 4.0 adoption will not be successful. Therefore it is essential for the top management to first understand the importance of technologies of Health 4.0 so that it can be implemented with high priority in the organizations. Another important barriers are exclusive and skilled workforce requirement, political support and inadequate maintenance support systems. Specialized technical and operational skills in handling the wide variety of clinical and non-clinical data in healthcare is the major requirement for Health 4.0. Digitization will change the specifications of the employees in all the phases of clinical chain i.e. from patient admission to discharge. All the medical processes will become more data driven requiring a completely new workforce expert in automation and software development. A similar study conducted by Koch et al. also concludes that Industry 4.0 requires employees who are expert in latest technologies of digitization (Koch et al. 2014). Health 4.0 requires substantial IT infrastructure that needs to be maintained and serviced regularly as any disturbance in the integrated process will disrupt the entire system. Therefore these issue need special attention and should be handled with utmost care. There is huge requirement for certain vocational courses like big data analytics, data science, and specialized computer courses in this growing age of digitalization. Government should support by creating the basis of these fundamental requirements for Health 4.0 adoption by laying down uniform standards at national and international levels which will help in free and secured information exchange (Bonczek et al. 2014). Large amount of sensitive and confidential clinical information is available online across the cloud computing environment. This poses data security issues as important private data may be accessed by other parties. Therefore this issue needs to be handled very diligently as digital systems are more prone to cyber-attacks. A study conducted by Pereira et al. also concludes that data security is the most serious and critical issue while implementing Industry 4.0 in the organizations (Pereira et al. 2017). Besides this, lack of uniform standards for information exchange is making it hard for smaller healthcare organizations to implement Health 4.0. It is very difficult to ensure liability and regulatory compliance as regulatory systems are not laid down properly. The important legal issues like liability, clinical data protection and security and intellectual property should be seriously taken care of (Alaba et al. 2017). In healthcare, data is huge, complicated and highly fragmented as it is evolved from diverse sources (Raghupathi and Raghupathi 2014). Clinical data includes notes written by clinicians and nurses, prescription slips, laboratory investigations, medical imaging reports, pharmacy, data generated from medical equipment like ventilator, ECGs and insurance reports etc. This huge variety of big data in healthcare industry is very difficult to be managed with available software systems.
6 Conclusion
Health 4.0 technologies have the ability to transform healthcare sector from a focussed and compassionate system to a value oriented system which can ensure proactive preventive measures. The barriers identified in this research will help the healthcare managers and policymakers to take concrete steps so that Health 4.0 can be implemented successfully in the healthcare sector in India. Also, barriers having high driving power can be identified easily so that management of healthcare organizations can develop strategies to deal with such barriers with high priority and execute Health 4.0 technologies meticulously in their organizations.
7 Implications of research, limitations and future prospects of research
Health 4.0 is a major breakaway in the healthcare industry and it has the potential to provide a new outlook to the industry by amalgamating the advanced technologies to attain utmost output with minimum usage of resources. But the review of existing literature shows that healthcare sector is facing certain barriers during the adoption of this remarkable phenomenon and despite maximum efforts fruitful results are not yet achieved in India. The results of this study presents many implications for the healthcare managers. Firstly, 15 such critical barriers with respect to Health 4.0 adoption in the Indian healthcare industry have been identified. The managers can thoroughly understand these barriers beforehand and focus towards reducing their effect so that Health 4.0 can be successfully implemented. Secondly, TISM methodology applied in the study will help to identify the interrelationships among these barriers so that the managers and decision makers can explore the effect of each barrier on other barriers as well as the degree of relationships among them. Thirdly, the model developed in the present research illustrates how various barriers affecting Health 4.0 adoption in healthcare organizations are interrelated and affect each other. Timely action taken by the management to remove these hurdles will not only reduce the cost but also improve quality of medical procedures so that true potential of Health 4.0 can be utilized.
In this research, 15 barriers affecting the Health 4.0 implementation in Indian healthcare industry have been identified. Some of the barriers were not considered which may affect Health 4.0 adoption in other countries. In future, similar researches may be carried out in many other countries as well to analyse the presence of several other barriers. Further, it is also suggested to do a comparative research regarding the existence of barriers to the adoption of Health 4.0 in the healthcare industries of other developing and developed countries to examine the significant variations if present. Also, quantification of TISM model can be done and the model can be further validated by using mathematical modeling and confirmatory factor analysis. SEM (Structural Equation Modeling) can be used to test the theoretical model.
References
Acemoglu D (2002) Technical change, inequality, and the labor market. J Econ Lit 40:7–72
Agarwal A, Vrat P (2015) A TISM based bionic model of organizational excellence. Glob J Flex Syst Manag 16:361–376
Ajmera P, Jain V (2019a) A fuzzy interpretive structural modeling approach for evaluating the factors affecting lean implementation in Indian healthcare industry. Int J Lean Six Sigma. https://doi.org/10.1108/IJLSS-02-2018-0016
Ajmera P, Jain V (2019b) Modeling the factors affecting the quality of life in diabetic patients in India using total interpretive structural modeling. Benchmarking: An Int J 26:951–970. https://doi.org/10.1108/BIJ-07-2018-0180
Alaba FA, Othman M, Hashem IAT, Alotaibi F (2017) Internet of things security: A survey. J Netw Comput Appl 88:10–28
Babiceanu RF, Seker R (2016) Big Data and virtualization for manufacturing cyber-physical systems: A survey of the current status and future outlook. Comput Ind 81:128–137
Bagheri B, Yang S, Kao H-A, Lee J (2015) Cyber-physical systems architecture for self-aware machines in industry 4.0 environment. IFAC-PapersOnLine 48:1622–1627
Bahrin MAK, Othman MF, Azli NN, Talib MF (2016) Industry 4.0: a review on industrial automation and robotic. Jurnal Teknologi 78:137–143
Bates DW, Saria S, Ohno-Machado L, Shah A, Escobar G (2014) Big data in health care: using analytics to identify and manage high-risk and high-cost patients. Health Aff 33:1123–1131
Benešová A, Tupa J (2017) Requirements for education and qualification of people in industry 4.0. Procedia Manufacturing 11:2195–2202
Bodenheimer T (1995) The industrial revolution in health care. Social Justice 22:26–42
Bonczek RH, Holsapple CW, Whinston AB (2014) Foundations of decision support systems. Academic Press, New York
Cao Q, Schniederjans DG, Schniederjans M (2017) Establishing the use of cloud computing in supply chain management. Oper Manag Res 10:47–63
Chawla NV, Davis DA (2013) Bringing big data to personalized healthcare: a patient-centered framework. J Gen Intern Med 28:660–665
Christians A, Liepin M (2017) The Consequences of digitalization for german civil law from the national legislator's point of view Zeitschrift fuer Geistiges Eigentum/Intellectual Property Journal 9:331–339
Deane JK, Ragsdale CT, Rakes TR, Rees LP (2009) Managing supply chain risk and disruption from IT security incidents. Oper Manag Res 2:4
Dubey R, Ali SS (2014) Identification of Flexible Manufacturing System Dimensions and Their Interrelationship Using Total Interpretive Structural Modelling and Fuzzy MICMAC Analysis Global Journal of Flexible Systems Management 15:131–143
Dubey R, Gunasekaran A, Papadopoulos T, Childe SJ, Shibin K, Wamba SF (2017) Sustainable supply chain management: framework and further research directions. J Clean Prod 142:1119–1130
Filipe L, Fdez-Riverola F, Costa N, Pereira A (2015) Wireless body area networks for healthcare applications: Protocol stack review International Journal of Distributed Sensor Networks 11:213705
Frey CB, Osborne MA (2017) The future of employment: how susceptible are jobs to computerisation? Technol Forecast Soc Chang 114:254–280
Gehrke L et al. (2015) A discussion of qualifications and skills in the factory of the future: a German and American perspective VDI/ASME Industry 4:1–28
Gray M (2008) Making the future of healthcare Zeitschrift für Evidenz. Fortbildung und Qualität im Gesundheitswesen 102:231–233
Harrison R, Vera D, Ahmad B (2016) Engineering methods and tools for cyber–physical automation systems. Proc IEEE 104:973–985
Hecklau F, Galeitzke M, Flachs S, Kohl H (2016) Holistic approach for human resource management in industry 4.0 Procedia CIRP 54:1-6
Holmström J, Holweg M, Khajavi SH, Partanen J (2016) The direct digital manufacturing (r) evolution: definition of a research agenda. Oper Manag Res 9:1–10
Jain V, Ajmera P (2018) Modelling the factors affecting Indian medical tourism sector using interpretive structural modeling benchmarking: An International Journal 25:1461–1479
Jain V, Raj T (2014) Modelling and analysis of FMS productivity variables by ISM. SEM and GTMA approach Frontiers of Mechanical Engineering 9:218–232. https://doi.org/10.1007/s11465-014-0309-7
Jain V, Raj T (2015) Modeling and analysis of FMS flexibility factors by TISM and fuzzy MICMAC Int J Syst Assurance Engr Manag 6:350-371 https://doi.org/10.1007/s13198-015-0368-0
Jain V, Raj T (2016) Modeling and analysis of FMS performance variables by ISM. SEM and GTMA approach International J Production Economics 171:84–96. https://doi.org/10.1016/j.ijpe.2015.10.024
Jain V, Soni VK (2019) Modeling and analysis of FMS performance variables by fuzzy TISM. J Model Manag 14:2–30. https://doi.org/10.1108/JM2-03-2018-0036
Jee K, Kim G-H (2013) Potentiality of big data in the medical sector: focus on how to reshape the healthcare system. Healthcare Informatics Research 19:79–85
Kagermann H (2015) Change through digitization—value creation in the age of industry 4.0. In: Management of permanent change. Springer, Wiesbaden, pp 23–45
Kagermann H, Lukas W-D, Wahlster W (2011) Industrie 4.0: Mit dem Internet der Dinge auf dem Weg zur 4. industriellen Revolution VDI nachrichten 13
Kamble SS, Gunasekaran A, Sharma R (2018) Analysis of the driving and dependence power of barriers to adopt industry 4.0 in Indian manufacturing industry. Comput Ind 101:107–119
Kamigaki T (2017) Object‐Oriented RFID with IoT: A Design Concept of Information Systems in Manufacturing Electronics 6:14
Khatwani G, Singh SP, Trivedi A, Chauhan A (2015) Fuzzy-TISM: A fuzzy extension of TISM for group decision making. Glob J Flex Syst Manag 16:97–112
Koch V, Kuge S, Geissbauer R, Schrauf S (2014) Industry 4.0: opportunities and challenges of the industrial internet strategy & PwC Available at: http://www.strategyand.pwc.com/reports/industry-4-0. Accessed 10 March 2017
Kumar P, Lee H-J (2011) Security issues in healthcare applications using wireless medical sensor networks: A survey Sensors 12:55–91
Kumar Srivastava A, Sushil (2014) Modelling drivers of adapt for effective strategy execution. Learn Organ 21:369–391
Lasi H, Fettke P, Kemper H-G, Feld T, Hoffmann M (2014) Industry 4.0 Business & Information Systems Engineering 6:239-242
Lee J, Kao H-A, Yang S (2014) Service innovation and smart analytics for industry 4.0 and big data environment Procedia Cirp 16:3–8
Li S, Da Xu L, Zhao S (2015) The internet of things: a survey Information Systems Frontiers 17:243-259
Lorincz K et al. (2004) Sensor networks for emergency response: challenges and opportunities IEEE pervasive Computing:16–23
Mahajan R, Agrawal R, Sharma V, Nangia V (2016) Analysis of challenges for management education in India using total interpretive structural modelling. Qual Assur Educ 24:95–122
Manogaran G, Thota C, Lopez D, Sundarasekar R (2017) Big data security intelligence for healthcare industry 4.0. In: Cybersecurity for Industry 4.0. Springer, Cham,Switzerland, pp 103–126
Mohanty M, Shankar R (2017) Modelling uncertainty in sustainable integrated logistics using Fuzzy-TISM Transportation Research Part D: Transport and Environment 53:471–491
Mueller E, Chen X-L, Riedel R (2017) Challenges and requirements for the application of industry 4.0: a special insight with the usage of cyber-physical system Chinese. J Mech Eng 30:1050
Murry JW Jr, Hammons JO (1995) Delphi: A versatile methodology for conducting qualitative research. Rev High Educ 18:423–436
Nasim S (2011) Total interpretive structural modeling of continuity and change forces in e-government. J Enterprise Transformation 1:147–168. https://doi.org/10.1080/19488289.2011.579229
Pereira T, Barreto L, Amaral A (2017) Network and information security challenges within industry 4.0 paradigm. Procedia Manufacturing 13:1253–1260
Prasad UC, Suri R (2011) Modeling of continuity and change forces in private higher technical education using total interpretive structural modeling (TISM). Glob J Flex Syst Manag 12:31–40
Qin J, Liu Y, Grosvenor R (2016) A categorical framework of manufacturing for industry 4.0 and beyond. Procedia Cirp 52:173–178
Qureshi MO, Syed RS (2014) The impact of robotics on employment and motivation of employees in the service sector, with special reference to health care safety and health at work 5:198-202
Raghupathi W, Raghupathi V (2014) Big data analytics in healthcare: promise and potential. Health Info Sci Syst 2:3
Rudrappa S, Agarkhed DV, Vaidya SS (2019) Healthcare systems: India. Quality Spine Care, Springer, Cham, Switzerland
Rüßmann M, Lorenz M, Gerbert P, Waldner M, Justus J, Engel P, Harnisch M (2015) Industry 4.0: the future of productivity and growth in manufacturing industries Boston. Consulting Group 9:54–89
Ryan PJ, Watson RB (2017) Research challenges for the internet of things: What role can OR play? Systems 5:24
Schröder C (2016) The challenges of industry 4.0 for small and medium-sized enterprises Friedrich-Ebert-Stiftung: Bonn, Germany
Shafiq SI, Sanin C, Toro C, Szczerbicki E (2015) Virtual engineering object (VEO): toward experience-based design and manufacturing for industry 4.0 cybernetics and systems 46:35-50
Shelbourn M, Hassan T, Carter C (2005) Legal and Contractual Framework for the VO. In: Virtual Organizations. Springer, Boston, MA, pp 167–176
Sushil (2012a) Flowing Stream Strategy: Managing Confluence of Continuity and Change Journal of Enterprise Transformation 2:26–49
Sushil S (2012b) Interpreting the interpretive structural model global journal of flexible systems management 13:87-106
Thuemmler C, Bai C (2017) Health 4.0: how virtualization and big data are revolutionizing healthcare. Springer, New York
Von Tunzelmann N (2003) Historical coevolution of governance and technology in the industrial revolutions. Struct Chang Econ Dyn 14:365–384
Warfield JN (1973) On arranging elements of a hierarchy in graphic form IEEE transactions on systems. Man, and Cybernetics SMC-3:121–132
Yadav N (2014) Total interpretive structural modelling (TISM) of strategic performance management for Indian telecom service providers international journal of productivity and performance management 63:421-445 https://doi.org/10.1108/IJPPM-04-2013-0081
Yadav N, Sushil, Sagar M (2015) Modeling strategic performance management of automobile manufacturing enterprises: An Indian context. J Model Manag 10:198–225
Yan Z, Zhang P, Vasilakos AV (2014) A survey on trust management for Internet of Things. J Netw Comput Appl 42:120–134
Zhou K, Liu T, Zhou L (2015) Industry 4.0: Towards future industrial opportunities and challenges. In: Fuzzy Systems and Knowledge Discovery (FSKD), 2015 12th International Conference on, 2015. IEEE, pp 2147–2152
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ajmera, P., Jain, V. Modelling the barriers of Health 4.0–the fourth healthcare industrial revolution in India by TISM. Oper Manag Res 12, 129–145 (2019). https://doi.org/10.1007/s12063-019-00143-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12063-019-00143-x