
Abstract
Background
Reporting of complications after total hip arthroplasty (THA) is not standardized, and it is done inconsistently across various studies on the topic. Advantages of standardizing complications include improved patient safety and outcomes and better reporting in comparative studies.
Questions/purposes
The purpose of this project was to develop a standardized list of complications and adverse events associated with THA, develop standardized definitions for each complication, and stratify the complications. A further purpose was to validate these standardized THA complications.
Methods
The Hip Society THA Complications Workgroup proposed a list of THA complications, definitions for each complication, and a stratification scheme for the complications. The stratification system was developed from a previously validated grading system for complications of hip preservation surgery. The proposed complications, definitions, and stratification were validated with an expert opinion survey of members of The Hip Society, a case study evaluation, and analysis of a large administrative hospital system database with a focus on readmissions.
Results
One hundred five clinical members (100%) of The Hip Society responded to the THA complications survey. Initially, 21 THA complications were proposed. The validation process reduced the 21 proposed complications to 19 THA complications with definitions and stratification that were endorsed by The Hip Society (bleeding, wound complication, thromboembolic disease, neural deficit, vascular injury, dislocation/instability, periprosthetic fracture, abductor muscle disruption, deep periprosthetic joint infection, heterotopic ossification, bearing surface wear, osteolysis, implant loosening, cup-liner dissociation, implant fracture, reoperation, revision, readmission, death).
Conclusions
Acceptance and use of these standardized, stratified, and validated THA complications and adverse events could advance reporting of outcomes of THA and improve assessment of THA by clinical investigators.
Level of Evidence
Level V, therapeutic study.
Similar content being viewed by others


Introduction
THA is one of the most clinically successful and cost-effective medical procedures developed during the last century. In 2007, The Lancet called THA “the operation of the century” [9]. The use and total expenditure of THA is increasing [8], and THA is one of the largest line item costs for the Centers of Medicare & Medicaid Services [2]. Such growth in demand comes with increased scrutiny from many sources, and numerous stakeholders seek to better measure outcomes in THA, including device-related complications, adverse events, and complications surrounding the surgical procedure and the perioperative time period.
Patients, health plans, and government entities are demanding increased accountability in health care, and complication rates are often used as a proxy for quality. Peer exercises such as morbidity and mortality conferences have a long tradition, but public reporting of complications requires a consistent methodology, standardized reporting, and validated evaluation instruments. Unfortunately, complication reporting in most medical and surgical specialties is not standardized or validated. Goldhahn et al. [5] performed a systematic review of randomized controlled clinical trials in the orthopaedic literature, and they determined there was no consistent, standard, universal reporting of complications in orthopaedic surgery.
The purpose of this Hip Society project is to improve complication reporting for THA by developing a standardized list of THA complications. This follows an analogous set of projects done by The Knee Society in 2013 and 2014 for complications after TKA [6, 7]. We sought to create standardized definitions for THA complications and stratify those complications according to severity and impact of the complication on patient outcome.
Materials and Methods
The Hip Society (http://www.hipsoc.org/web/goals.html) is an orthopaedic specialty organization based in the United States whose mission is “to advance knowledge of hip disorders, promote evidence based treatment, and refine surgery of the hip in order to improve the lives of patients.” The Hip Society is a selective professional organization composed of orthopaedic surgeons and researchers who have made substantial contributions to advancing knowledge and improving treatment of hip disorders through writing, lecturing, and teaching others. Members of The Hip Society are generally acknowledged as experts regarding THA.
In 2011 The Hip Society Board of Directors established a Total Hip Arthroplasty Complications Workgroup consisting of the authors of this article. The work began with a goal of developing a standardized list of the “minimum necessary” complications and adverse events required for accurate reporting of outcomes of THA. Further goals were to create standardized definitions for these THA complications and to develop a system for stratification and validation of the THA complications.
The THA Complications Workgroup reviewed the orthopaedic literature on THA outcomes and surveyed the medical and surgical literature on complication reporting. The Workgroup developed a list of THA complications with a definition for each complication, and they correlated the THA complications with International Classification of Diseases, 9th Revision codes. Conditions that could not be clearly defined as complications or adverse events directly related to the THA operation were not included on the list; eg, medical complications (cardiac, pulmonary, renal, etc), anesthetic issues (nausea, arrhythmias, memory loss, etc), and poor functional outcomes were not included.
An expert opinion survey of members of The Hip Society was conducted to test the reasonableness and general applicability of the proposed THA complications. For each proposed complication or adverse event, members of The Hip Society were asked, “Do you agree with the inclusion of the complication as among the minimum necessary for reporting outcomes of total hip arthroplasty?” and “Do you agree with this definition?” In addition, Hip Society members were asked for comments and suggestions regarding additional complications to add to the list, complications to delete from the list, and revisions of the proposed definitions. One hundred five clinical members (100%) of The Hip Society responded to the survey, and members provided a total of 568 comments and suggestions.
Responses to the yes/no questions were evaluated with chi-square tests. We determined that an item (complication) was acceptable if at least 60% of the respondents/members responded with an affirmative response “yes.”
The THA Complications Workgroup also reviewed literature regarding stratification of surgical complications. The Workgroup specifically focused on reports from Clavien et al. [3] and Dindo et al. [4] regarding general surgery complications and Sink et al. [11] regarding hip preservation surgery. In addition, the Workgroup evaluated the work of The Knee Society regarding TKA complications and stratification of TKA complications [6, 7]. Based on this literature review, a scheme was developed for stratifying THA complications (Table 1).
Validity and reasonableness of the THA complications and adverse events were assessed three ways. First, members of The Hip Society were asked to endorse the THA complications and definitions with an expert opinion survey. Second, a clinical case evaluation method was used to validate this work. Clinical case examples with clinical and radiographic data were developed for each of the proposed THA complications. One case example was developed for each proposed complication. The case examples were evaluated by 61 orthopaedic surgeons with subspecialty expertise in adult reconstruction and 15 adult reconstruction postgraduate fellows (typically Postgraduate Year 6). For the clinical case evaluation, agreement of 80% was deemed necessary to validate the proposed definitions and stratification. This is a higher bar of concordance than was suggested by our statistician for analysis of The Hip Society expert opinion survey. Third, in an effort to further validate this project, an administrative database of Medicare readmissions at New York University Langone Medical Center was used to analyze the THA complications. Readmitted patients enrolled in the New York University Langone Medical Center–Hospital for Joint Diseases Bundled Payment Care Initiative during 2013 were examined. This readmitted population included 53 patients readmitted within 90 days of their index THA.
Results
Based on this work from the THA Complications Workgroup, 19 THA complications/adverse events and their definitions were endorsed by The Hip Society including: bleeding, wound complication, thromboembolic disease, neural deficit, vascular injury, dislocation/instability, periprosthetic fracture, abductor muscle disruption, deep periprosthetic joint infection, heterotopic ossification, bearing surface wear, osteolysis, implant loosening, cup-liner dissociation, implant fracture, reoperation, revision, readmission, and death (Table 2). This list evolved from the following process.
Initially, 21 “minimum necessary” THA complications and adverse events with 21 specific definitions were proposed by the THA Complications Workgroup. These proposed THA complications were then evaluated by the expert opinion survey of members of The Hip Society. The workgroup addressed the comments and suggestions from the survey and revised the list and the definitions of the THA complications. Twenty of the 21 proposed complications and associated definitions were initially endorsed by The Hip Society survey.
The second methodology used to analyze the proposed complications was clinical case evaluations. This process validated 13 of the 20 proposed THA complications (bleeding, wound complication, thromboembolic disease, neural deficit, vascular injury, dislocation/instability, periprosthetic fracture, abductor muscle disruption, deep periprosthetic joint infection, heterotopic ossification, implant loosening, cup liner dissociation, and implant fracture) (Table 3).
Bearing surface wear and osteolysis did not achieve 80% concurrence from the clinical case evaluators. The bearing surface wear case achieved 77% agreement. Alternative assignments for this case include osteolysis (17%) and implant loosening (3%). Based on the fact that bearing surface wear, osteolysis, and implant loosening are intimately related in the interpretation of this clinical scenario, bearing surface wear was validated as a THA complication. The osteolysis case also achieved 77% concurrence from the clinical case evaluators. Eighteen percent of the evaluators assigned this case to implant loosening. Based on the fact that osteolysis and implant loosening are intimately related in the interpretation of this clinical scenario, osteolysis was validated as a THA complication (Table 3).
The leg length discrepancy case achieved only 71% agreement from the clinical case evaluators in the validation process. Alternative assignments for this case included dislocation (11%) and revision (9%). Neither of these alternative conditions is related to leg length discrepancy. Furthermore, leg length discrepancy was initially endorsed by only 73% of members of The Hip Society in the expert opinion survey, and several comments from the expert opinion survey recommended omitting this condition from the list of complications. Based on underwhelming endorsement by members of The Hip Society, a clear recommendation to not include this condition, lack of an accepted formal definition, and failure to achieve 80% agreement in the clinical case validation process, leg length discrepancy was deleted from the list of proposed THA complications.
Four of the THA complications (reoperation, revision, readmission, and death) are required objective outcome data points that did not require validation (Table 3).
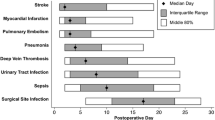
The third method chosen to analyze the proposed complications, review of readmissions in an administrative database, showed that the most common reason for readmission was for a general, nonsurgical intervention (51%): postsurgical pain, bacteremia/sepsis, gastrointestinal complications, pulmonary disease, genitourinary complications, and endocrine disturbances. Eight unique THA complications were observed in this cohort: bleeding, wound complication, thromboembolic disease, dislocation/instability, periprosthetic fracture, deep periprosthetic joint infection, readmission, and revision, all of which are included in the proposed THA complications.
The 19 THA complications endorsed by The Hip Society were stratified for severity using a modification of the Sink classification of complications associated with hip preservation surgery [11] (Table 1). This stratification scheme was used previously for stratifying TKA complications [7] and progresses from complications requiring no treatment and having no clinical relevance to death (Table 1).
Discussion
Complications and adverse events after THA can compromise patient outcomes, increase hospital readmissions, decrease patient satisfaction, and increase healthcare cost. Despite the clinical success of THA [9], complications after THA can be expected despite reasonable and safe care, and rates of complications after total joint arthroplasty can vary considerably among hospitals [1]. Complication reporting can identify potential problems with patient selection, surgical techniques, joint implants, and postoperative care regimens [10]. It has also been suggested that standardized reporting of THA complications can improve patient safety and outcomes along with standardizing research assessments [5].
In general, reporting of THA complications and adverse events is not standardized. Different investigators report different complications with different definitions. Furthermore, all THA complications are not equal. Stratification of complications can increase clinical applicability and improve the clarity of research. The goal of the THA Complications Workgroup was to identify, define, and stratify THA complications. Previously, standardized complications for TKA were reported by The Knee Society [6, 7].
This report has several important limitations, which the reader should consider when interpreting and/or implementing our work. First, the orthopaedic literature does not have consensus definitions for many of the conditions proposed. Second, information regarding THA complications was collected from surgeon- and researcher-generated publications. Patient input was not solicited or used in this project, which may have altered this list of complications and adverse events. Third, the project relies on an expert opinion review for validation of the THA complications, which by definition is Level V evidence. The THA Complications Workgroup believes that the expert opinion survey of members of The Hip Society is valid because members of The Hip Society are generally considered experts and teachers regarding THA, and thousands of THA operations delivered over several decades provide the foundation for their opinions. Fourth, the validation process includes clinical scenarios, which can be interpreted differently by different clinicians, and many of the conditions described are a continuum of outcomes without clearcut boundaries of an adverse event or complication. A fifth and important limitation of this project and report is the fact that this article is not a legal document, and it does not intend to define a standard of care.
Nineteen THA complications with definitions and stratification are endorsed by The Hip Society as a result of this project (Table 1). This list of THA complications excluded several conditions and adverse events associated with hip arthroplasty because they were difficult to define; they may have been preexisting conditions; they were difficult to associate with the index THA; they were not endorsed by the expert opinion survey; and/or they were not validated by the validation process. Adverse events that were excluded include hypotension related to polymethylmethacrylate, pressure sores, leg length discrepancy, persistent hip pain after THA, and patient dissatisfaction with the procedure. Pressure sores were excluded by the expert opinion survey. Leg length discrepancy was excluded for lack of a consensus definition, minimal support in the expert opinion survey, and failure to be validated in the clinical case evaluation. Leg length discrepancy was excluded despite the fact that this condition is a frequent cause of patient dissatisfaction and litigation. Medical complications such as cardiac events, pulmonary compromise, renal failure, change in mental status, etc, can compromise the outcome after hip arthroplasty, but they were not included as specific complications after THA because these conditions may or may not be associated with the operation and perioperative care.
All conditions included in this list of THA complications and adverse events affect patient outcome. However, all of these conditions, and all of the stratified grades of these conditions, are not true complications of the operation or postoperative care. Some of the conditions are adverse events. For example, suture or staple erythema is not a wound complication, and all THAs have some blood loss without being labeled a bleeding complication. Additionally, an infection 2 years after the index THA is not defined as a perioperative periprosthetic infection, but it is clearly an adverse event for the patient. Furthermore, bearing surface wear can lead to osteolysis and a revision operation, but it is not a complication of the original THA. However, bearing surface wear can be an adverse event for the patient, and it is important in evaluating patient outcome. Several conditions were included as complications with a provision in the definition that the condition is “symptomatic” for the patient. For example, some wear of the bearing surface is normal and expected with any hip arthroplasty. However, wear that leads to reoperation or revision must be considered at least an adverse event for the patient. Hence, both complications and adverse events provide valuable information when evaluating patient outcome.
Complications and adverse events are associated with all medical and surgical treatments. By identifying and defining complications and adverse events associated with THA, this project intended to improve quality and safety for THA. This article is intended to assist surgeons, researchers, health plans, and government officials in evaluating the surgical results and patient outcomes after hip arthroplasties. This project did not intend to identify problems that suggest a hip arthroplasty was not planned or performed correctly. This article is not intended as a legal document, and the authors specifically reject the notion that these THA complications and adverse events define substandard care. As noted earlier, and again emphasized, complications can be associated with medical treatments and surgical procedures despite the delivery of reasonable and safe care.
We believe this standardized list of 19 THA complications with standardized definitions and stratification endorsed by The Hip Society will improve reporting of THA outcomes if they are endorsed and adopted by orthopaedic surgeons, orthopaedic professional societies, orthopaedic investigators, and orthopaedic journals. We suggest that clinical trials and THA outcome studies will be enhanced if these complications and their definitions and stratifications are used. Ultimately, standardization of reporting of THA outcomes and complications could lead to improved patient selection, surgical procedures, clinical protocols, hip implants, and patient outcomes for THA. It is clear in the evolving world of healthcare accountability that it is preferable for hip surgeons themselves to define THA complications and adverse events rather than be forced to accept the suggestions of others.
References
Bozic KJ, Grosso LM, Lin Z, Parzynski CS, Suter LG, Krumholz HM, Lieberman JR, Berry DJ, Bucholz R, Han L, Rapp MT, Bernheim S, Drye EE. Variation in hospital-level risk-standardized complication rates following elective primary total hip and knee arthroplasty. J Bone Joint Surg Am. 2014;96:640–647.
Centers for Medicare & Medicaid Services. Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Inpatient.html. Accessed April 27, 2015.
Clavien PA, Barkun J, deOliveira ML, Vauthey JN, Dindo D, Schulick RD, deSantibanes E, Peckolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Markuuchi M. The Clavien-Dindo classification of surgical complications: 5 year experience. Ann Surg. 2009;205:187–196.
Dindo D, DeMartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6,336 patients and results of a survey. Ann Surg. 2004;240:205–213.
Goldhahn S, Sawaguchi T, Audije L, Mund R, Hanson B, Bahandari M, Goldhahn J. Complication reporting in orthopedic trials: a systematic review of randomized controlled trials. J Bone Joint Surg Am. 2009;91:1847–1853.
Healy WL, DellaValle CJ, Iorio R, Berend KR, Cushner FD, Dalury DF, Lonner JH. Complications of total knee arthroplasty: standardized list and definitions of The Knee Society. Clin Orthop Relat Res. 2013;471:215–220.
Iorio R, DellaValle CJ, Healy WL, Berend KR, Cushner FD, Delury DF, Lonner JH. Stratification of standardized TKA complications and adverse events: a brief communication. Clin Orthop Relat Res. 2014;472:194–205.
Kurtz SM, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005–2030. J Bone Joint Surg Am. 2007;89:781–785.
Learmonth I. The operation of the century: total hip replacement. Lancet. 2007;370:1508–1519.
Robertsson O, Dunbar MJ. Patient satisfaction compared with general health and disease-specific questionnaires in knee arthroplasty patients. J Arthroplasty. 2001;16:476–482.
Sink EL, Leunig M, Zaltz I, Gilbert JC, Clohisy J. Reliability of a complication classification system for orthopedic surgery. Clin Orthop Relat Res. 2012;470:2220–2226.
Acknowledgments
We thank Joann Lee NP, for her assistance with the preparation of this manuscript, and we thank the members of The Hip Society for participating in the project and endorsing the work product.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (WLH) certifies that he receives royalties from DePuy Orthopaedics (Warsaw, IN, USA) in an amount of USD 10,000 to USD 1,000,000. One of the authors (RI) certifies that he has a product development agreement with IMDS Kyocera (Kyoto, Japan); is on the boards of The Knee Society, The Hip Society, and the New England Orthopaedic Society; and is a reviewer/editor for the Journal of Bone and Joint Surgery, Clinical Orthopaedics and Related Research ®, the Journal of Arthroplasty, and the Journal of the American Academy of Orthopaedic Surgeons. One of the authors (VDP) certifies that he receives royalties from DePuy Orthopaedics in an amount of USD 10,000 to USD 1,000,000 and is on the board of The Hip Society. One of the authors (CJDV) certifies that he receives research support from Biomet (Warsaw, IN, USA), CD Diagnostics (Wynnewood, PA, USA), Smith & Nephew (Memphis, TN, USA), and Stryker (Mahwah, NJ, USA) in amounts of USD 10,000 to USD 1,000,000; is a consultant for Biomet, DePuy Orthopaedics, and Smith & Nephew and receives USD 10,000 to USD 1,000,000; and has investments in CD Diagnostics (Wynnewood, PA, USA). One of the authors (KRB) certifies that he receives royalties from, is a consultant for, and receives research support from Biomet; receives institutional research support from Biomet, Stryker (Mahwah, NJ, USA), Kinamed (Camarillo, CA, USA), Pacira (Parsippany, NJ, USA), and Piedmont Orthopaedic Society; has investments in VuMedi; is a reviewer/editor for Clinical Orthopaedics and Related Research ®, the Journal of Arthroplasty, Journal of Bone and Joint Surgeons, Orthopedics, and Reconstructive Review; and is on the boards of The Knee Society, American Association of Hip and Knee Surgeons, and Board of Specialties.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Healy, W.L., Iorio, R., Clair, A.J. et al. Complications of Total Hip Arthroplasty: Standardized List, Definitions, and Stratification Developed by The Hip Society. Clin Orthop Relat Res 474, 357–364 (2016). https://doi.org/10.1007/s11999-015-4341-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4341-7