
Abstract
Background
Surgical site infection (SSI) ranges from 1.9% to 5.5% in most large series. Minimally invasive surgery (MIS) has been postulated to reduce SSI rates.
Questions/purposes
(1) Is MIS associated with a lower incidence of SSI compared with open spinal surgery? (2) Are there other independent risk factors associated with SSI? (3) What bacteria are most common in spinal SSI?
Methods
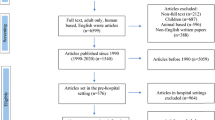
Medical records of 2299 patients who underwent transforaminal lumbar interbody fusion, laminectomy, or discectomy were analyzed and selected for a nested case-control analysis. Twenty-seven cases with SSI were matched with 162 control subjects without SSI stratified based on procedure performed within 28 days of the case’s date of surgery. Patients were identified from an institutional database at a tertiary care hospital. MIS involved spinal procedures performed through a tubular retractor system. Univariate and multivariate analyses were performed.
Results
Patients undergoing open spinal surgery were 5.77 times more likely to develop SSI compared with MIS approaches (odds ratio [OR], 5.77; 95% confidence interval [CI], 1.0–32.7; p = 0.048). Also, from the multivariate regression model, diabetes (OR, 4.7; 95% CI, 1.3–17.0; p = 0.018), number of levels operated on (OR, 3.5; 95% CI, 1.6–7.5; p = 0.001), and body mass index (OR, 1.2; 95% CI, 1.0–1.3; p = 0.010) were predictive of an increased risk in SSI. Staphylococcus aureus was most frequently identified, being present in 12 of 21 (52.4%) patients in whom positive cultures were obtained. Four of the 12 patients had methicillin-resistant S aureus infection.
Conclusions
In our series, MIS has a lower incidence of SSI. The risk factors predictive of SSI should be further evaluated in well-designed prospective trials.
Level of Evidence
Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


References
Choban PS, Heckler R, Burge JC, Flancbaum L. Increased incidence of nosocomial infections in obese surgical patients. Am Surg. 1995;61:1001–1005.
Fang A, Hu SS, Endres N, Bradford DS. Risk factors for infection after spinal surgery. Spine. 2005;30:1460–1465.
Gejo R, Matsui H, Kawaguchi Y, Ishihara H, Tsuji H. Serial changes in trunk muscle performance after posterior lumbar surgery. Spine. 1999;24:1023–1028.
Hong HS, Chang MC, Liu CL, Chen TH. Is aggressive surgery necessary for acute postoperative deep spinal wound infection? Spine. 2008;33:2473–2478.
Kabon B, Nagele A, Reddy D, Eagon C, Fleshman JW, Sessler DI, Kurz A. Obesity decreases perioperative tissue oxygenation. Anesthesiology. 2004;100:274–280.
Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior lumbar spine surgery. A histologic and enzymatic analysis. Spine. 1996;21:941–944.
Koutsoumbelis S, Hughes AP, Girardi FP, Cammisa FP Jr, Finerty EA, Nguyen JT, Gausden E, Sama AA. Risk factors for postoperative infection following posterior lumbar instrumented arthrodesis. J Bone Joint Surg Am. 2011;93:1627–1633.
LaVan FB, Hunt TK. Oxygen and wound healing. Clin Plast Surg. 1990;17:463–472.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27:97–132; quiz 133–134; discussion 196.
O’Toole JE, Eichholz KM, Fessler RG. Surgical site infection rates after minimally invasive spinal surgery. J Neurosurg. 2009;11:471–476.
Olsen MA, Nepple JJ, Riew KD, Lenke LG, Bridwell KH, Mayfield J, Fraser VJ. Risk factors for surgical site infection following orthopaedic spinal operations. J Bone Joint Surg Am. 2008;90:62–69.
Parker SL, Adogwa O, Witham TF, Aaronson OS, Cheng J, McGirt MJ. Post-operative infection after minimally invasive versus open transforaminal lumbar interbody fusion (TLIF): literature review and cost analysis. Minim Invasive Neurosurg. 2011;54:33–37.
Picada R, Winter RB, Lonstein JE, Denis F, Pinto MR, Smith MD, Perra JH. Postoperative deep wound infection in adults after posterior lumbosacral spine fusion with instrumentation: incidence and management. J Spinal Disord. 2000;13:42–45.
Pullter Gunne AF, Cohen DB. Incidence, prevalence, and analysis of risk factors for surgical site infection following adult spinal surgery. Spine. 2009;34:1422–1428.
Schimmel JJ, Horsting PP, de Kleuver M, Wonders G, van Limbeek J. Risk factors for deep surgical site infections after spinal fusion. Eur Spine J. 2010;19:1711–1719.
Schuster JM, Rechtine G, Norvell DC, Dettori JR. The influence of perioperative risk factors and therapeutic interventions on infection rates after spine surgery: a systematic review. Spine. 2010;35:S125–137.
Schwender JD, Foley KT, Holly LT, Transfeldt EE. Minimally invasive posterior surgical approaches to the lumbar spine. In: Rothman RH, Simeone FA, Herkowitz HN, eds. The Spine. 5th ed. Philadelphia, PA, USA: Saunders/Elsevier; 2006:333–341.
Sihvonen T, Herno A, Paljarvi L, Airaksinen O, Partanen J, Tapaninaho A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine. 1993;18:575–581.
Smith JS, Shaffrey CI, Sansur CA, Berven SH, Fu KM, Broadstone PA, Choma TJ, Goytan MJ, Noordeen HH, Knapp DR Jr, Hart RA, Donaldson WF 3rd, Polly DW Jr, Perra JH, Boachie-Adjei O. Rates of infection after spine surgery based on 108,419 procedures: a report from the Scoliosis Research Society Morbidity and Mortality Committee. Spine. 2011;36:556–563.
Steyerberg EW, Eijkemans MJ, Harrell FE Jr, Habbema JD. Prognostic modeling with logistic regression analysis: in search of a sensible strategy in small data sets. Med Decis Making. 2001;21:45–56.
Wacholder S, Silverman DT, McLaughlin JK, Mandel JS. Selection of controls in case-control studies. II. Types of controls. Am J Epidemiol. 1992;135:1029–1041.
Weinstein MA, McCabe JP, Cammisa FP Jr. Postoperative spinal wound infection: a review of 2,391 consecutive index procedures. J Spinal Disord. 2000;13:422–426.
Acknowledgments
We thank Bennet Ong, Dr Vinaykumar M. Siddaraju, and Dr Ian Cheung for their assistance in data acquisition.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (WMY) certifies that he is a consultant to Medtronic (Singapore) and has received payment of benefits during the study period an amount of USD 10,000 to USD 100,000. Also he is a consultant to DePuy-Synthes (Singapore) and has received payment of benefits during the study period, an amount of less than USD 10,000. In addition, he receives fellowship support from Medtronic of an amount of USD 10,000 to USD 100,000 and fellow support from Depuy-Synthes of an amount of USD 10,000 to USD 100,000. Also, he has received a research grant from Medtronic for an unrelated topic of an amount of USD 10,000 to USD 100,000.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Ee, W.W.G., Lau, W.L.J., Yeo, W. et al. Does Minimally Invasive Surgery Have a Lower Risk of Surgical Site Infections Compared With Open Spinal Surgery?. Clin Orthop Relat Res 472, 1718–1724 (2014). https://doi.org/10.1007/s11999-013-3158-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-3158-5