
Abstract
Background
Patients with neuromuscular disease reportedly have a higher incidence of postoperative dislocation after bipolar hemiarthroplasty. Although the literature has focused on a high prevalence of preoperative neurologic conditions in patients who had dislocations after bipolar hemiarthroplasties, the relative incidence of dislocation in patients with neuromuscular disease and without is unclear.
Questions/purposes
We therefore (1) asked whether the incidence of postoperative dislocation after bipolar hemiarthroplasty was greater in patients with neuromuscular disease than for those without, and (2) whether function differed between the two groups, and (3) explored potential risk factors for dislocation in two groups.
Methods
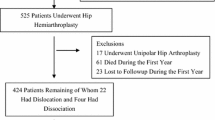
We retrospectively reviewed 190 patients who underwent bipolar hemiarthroplasties for fracture of the femoral neck between 1996 and 2008. Of the 190 patients, 42 had various neuromuscular diseases and 148 had no history of neuromuscular disease. Intraoperative stability was tested and posterior soft tissue repair was performed in all patients. We determined the incidence of dislocation, postoperative leg length discrepancy, and femoral offset in patients with or without neuromuscular disease.
Results
The incidence of dislocation was 2.6% in all patients. We observed similar rates of dislocation in the two groups: 4.8% (two of 42 hips) in patients with neuromuscular disease and 2.0% (three of 148 hips) in patients without neuromuscular disease.
Conclusions
In femoral neck fractures in patients with neuromuscular disease, careful preoperative management and operative technique such as a posterior soft tissue repair might decrease the risk of postoperative dislocation; therefore, we consider the bipolar hemiarthroplasty a reasonable treatment option.
Level of Evidence
Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.


Similar content being viewed by others

References
Barnes CL, Berry DJ, Sledge CB. Dislocation after bipolar hemiarthroplasty of the hip. J Arthroplasty. 1995;10:667–669.
Bhuller GS. Use of Giliberty bipolar endoprosthesis in femoral neck fractures. Clin Orthop Relat Res.1982;162:165–169.
Blewitt N, Mortimore S. Outcome of dislocation after hemiarthroplasty for fractured neck of the femur. Injury. 1992;23:320–322.
Bloem BR, Grimbergen YA, Cramer M, Willemsen M, Zwinderman AH. Prospective assessment of falls in Parkinson’s disease. J Neurol. 2001;248:950–958.
Bochner RM, Pellicci PM, Lyden JP. Bipolar hemiarthroplasty for fracture of the femoral neck: clinical review with special emphasis on prosthetic motion. J Bone Joint Surg Am. 1988;70:1001–1010.
Bush JB, Wilson MR. Dislocation after hip hemiarthroplasty: anterior versus posterior capsular approach. Orthopedics. 2007;30:138–144.
Cabanela ME, Weber M. Total hip arthroplasty in patients with neuromuscular disease. Instr Course Lect. 2000;49:163–168.
Clubb VJ, Clubb SE, Buckley S. Parkinson’s disease patients who fracture their neck of femur: a review of outcome data. Injury. 2006;37:929–934.
Coughlin L, Templeton J. Hip fractures in patients with Parkinson’s disease. Clin Orthop Relat Res. 1980;148:192–195.
Eiskjaer S, Ostgard SE. Risk factors influencing mortality after bipolar hemiarthroplasty in the treatment of fracture of the femoral neck. Clin Orthop Relat Res. 1991;270:295–300.
Eventov I, Moreno M, Geller E, Tardiman R, Salama R. Hip fractures in patients with Parkinson’s syndrome. J Trauma. 1983;23:98–101.
Georgiou G, Siapkara A, Dimitrakopoulou A, Provelengios S, Dounis E. Dissociation of bipolar hemiarthroplasty of the hip after dislocation: a report of five different cases and review of literature. Injury. 2006;37:162–168.
Haidukewych GJ, Israel TA, Berry DJ. Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res. 2002;403:118–126.
Hedlundh U, Karlsson M, Ringsberg K, Besjakov J, Fredin H. Muscular and neurologic function in patients with recurrent dislocation after total hip arthroplasty: a matched controlled study of 65 patients using dual-energy X-ray absorptiometry and postural stability tests. J Arthroplasty. 1999;14:319–325.
Iorio R, Healy WL, Lemos DW, Appleby D, Lucchesi CA, Saleh KJ. Displaced femoral neck fractures in the elderly: outcomes and cost effectiveness. Clin Orthop Relat Res. 2001;383:229–242.
Iorio R, Specht LM, Healy WL, Tilzey JF, Presutti AH. The effect of EPSTR and minimal incision surgery on dislocation after THA. Clin Orthop Relat Res. 2006;447:39–42.
Kao CH, Chen CC, Wang SJ, Chia LG, Yeh SH. Bone mineral density in patients with Parkinson’s disease measured by dual photon absorptiometry. Nucl Med Commun. 1994;15:173–177.
Ko CK, Law SW, Chiu KH. Enhanced soft tissue repair using locking loop stitch after posterior approach for hip hemiarthroplasty. J Arthroplasty. 2001;16:207–211.
Kwon MS, Kuskowski M, Mulhall KJ, Macaulay W, Brown TE, Saleh KJ. Does surgical approach affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res. 2006;447:34–38.
Pajarinen J, Savolainen V, Tulikoura I, Lindahl J, Hirvensalo E. Factors predisposing to dislocation of the Thompson hemiarthroplasty: 22 dislocations in 338 patients. Acta Orthop Scand. 2003;74:45–48.
Paterno SA, Lachiewicz PF, Kelley SS. The influence of patient-related factors and the position of the acetabular component on the rate of dislocation after total hip replacement. J Bone Joint Surg Am. 1997;79:1202–1210.
Paton RW, Hirst P. Hemiarthroplasty of the hip and dislocation. Injury. 1989;20:167–169.
Queally JM, Abdulkarim A, Mulhall KJ. Total hip replacement in patients with neurological conditions. J Bone Joint Surg Br. 2009;91:1267–1273.
Rao JP, Vernoy TA, Allegra MP, DiPaolo D. A comparative analysis of Giliberty, Bateman, and Universal femoral head prostheses: a long-term follow-up evaluation. Clin Orthop Relat Res. 1991;268:188–196.
Sierra RJ, Schleck CD, Cabanela ME. Dislocation of bipolar hemiarthroplasty: rate, contributing factors, and outcome. Clin Orthop Relat Res. 2006;442:230–238.
Sioen W, Simon JP, Labey L, Van Audekercke R. Posterior transosseous capsulotendinous repair in total hip arthroplasty: a cadaver study. J Bone Joint Surg Am. 2002;84:1793–1798.
Star MJ, Colwell CW Jr, Donaldson WF 3rd, Walker RH. Dissociation of modular hip arthroplasty components after dislocation: a report of three cases at differing dissociation levels. Clin Orthop Relat Res. 1992;278:111–115.
Suh KT, Moon KP, Lee HS, Lee CK, Lee JS. Consideration of the femoral head cartilage thickness in preoperative planning in bipolar hemiarthroplasty. Arch Orthop Trauma Surg. 2009;129:1309–1315.
Suh KT, Park BG, Choi YJ. A posterior approach to primary total hip arthroplasty with soft tissue repair. Clin Orthop Relat Res. 2004;418:162–167.
Suh KT, Roh HL, Moon KP, Shin JK, Lee JS. Posterior approach with posterior soft tissue repair in revision total hip arthroplasty. J Arthroplasty. 2008;23:1197–1203.
Turcotte R, Godin C, Duchesne R, Jodoin A. Hip fractures and Parkinson’s disease: a clinical review of 94 fractures treated surgically. Clin Orthop Relat Res. 1990;256:132–136.
Varley J, Parker MJ. Stability of hip hemiarthroplasties. Int Orthop. 2004;28:274–277.
Woolson ST, Rahimtoola ZO. Risk factors for dislocation during the first 3 months after primary total hip replacement. J Arthroplasty. 1999;14:662–668.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he has no commercial association (eg, consultancies, stock ownership, equity interest, patent, licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his institution has approved the human use protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for clinical participation in the study was obtained.
About this article
Cite this article
Suh, K.T., Kim, D.W., Lee, H.S. et al. Is the Dislocation Rate Higher after Bipolar Hemiarthroplasty in Patients with Neuromuscular Diseases?. Clin Orthop Relat Res 470, 1158–1164 (2012). https://doi.org/10.1007/s11999-011-2139-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-2139-9