
Opinion statement
In ST-segment elevation myocardial infarction (STEMI), interventional cardiologists must move quickly to safely re-establish blood flow while choosing an antithrombotic to preclude wire thrombosis, aid in the restoration of flow, minimize thrombus propagation, and reduce the risk of stent thrombosis. Currently, operators have a choice between heparin and bivalirudin with the possible addition of glycoprotein IIb/IIIa inhibitors (GPIs). Prior studies have shown that bivalirudin use lowers rates of bleeding, but with a clear risk of acute stent thrombosis. Recent studies have examined this question in the modern era of radial access and newer antiplatelet agents. Despite these studies, there remains a question regarding which antithrombotic agent is to be selected in STEMI.
Similar content being viewed by others

References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance
Bittl JA et al. Treatment with bivalirudin (hirulog) as compared with heparin during coronary angioplasty for unstable or postinfarction angina. Hirulog angioplasty study investigators. N Engl J Med. 1995;333(12):764–9.
Lincoff AM et al. Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention: REPLACE-2 randomized trial. JAMA. 2003;289(7):853–63.
Stone GW et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med. 2008;358(21):2218–30.
Stone GW et al. Heparin plus a glycoprotein IIb/IIIa inhibitor versus bivalirudin monotherapy and paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction (HORIZONS-AMI): final 3-year results from a multicentre, randomised controlled trial. Lancet. 2011;377(9784):2193–204.
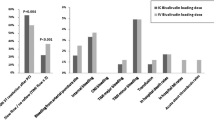
Han Y et al. Bivalirudin vs heparin with or without tirofiban during primary percutaneous coronary intervention in acute myocardial infarction: the BRIGHT randomized clinical trial. JAMA. 2015;313(13):1336–46. This well-designed landmark randomized controlled trial stands out in the published literature as being the only STEMI-focused trial that evaluates both the use of bivalirudin versus heparin, as well as the use of a glycoprotein IIb/IIIa inhibitor (tirofiban).
Schulz S et al. Prasugrel plus bivalirudin vs. clopidogrel plus heparin in patients with ST-segment elevation myocardial infarction. Eur Heart J. 2014;35(34):2285–94.
Shahzad A et al. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. Lancet. 2014;384(9957):1849–58.
Valgimigli M et al. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385(9986):2465–76.
Valgimigli M et al. Scientific foundation and possible implications for practice of the minimizing adverse haemorrhagic events by transradial access site and Systemic implementation of AngioX (MATRIX) trial. J Cardiovasc Transl Res. 2014;7(1):101–11.
Valgimigli M et al. Bivalirudin or unfractionated heparin in acute coronary syndromes. N Engl J Med. 2015;373(11):997–1009. Landmark study investigating bivalirudin versus heparin in acute coronary syndromes that demonstrated that the rate of MACE was not significantly lower with bivalirudin versus heparin, nor was the rate of net adverse clinical events. Post-PCI bivalirudin infusion, as compared with no infusion, did not significantly decrease the rate of urgent target-vessel revascularization, definite stent thrombosis, or net adverse clinical events.
Cavender MA, Faxon DP. Can BRIGHT restore the glow of bivalirudin? JAMA. 2015;313(13):1323–4. A well-written editorial that simultaneously questions and demonstrates to the reader the importance of the BRIGHT trial in light of the already-published literature on antithrombotic selection when treating STEMI and acute coronary syndrome as a whole.
Bavry AA et al. Critical appraisal of bivalirudin versus heparin for percutaneous coronary intervention: a meta-analysis of randomized trials. PLoS One. 2015;10(5):e0127832.
Stone GW et al. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary percutaneous coronary intervention: pooled patient-level analysis from the HORIZONS-AMI and EUROMAX trials. J Am Coll Cardiol. 2015;65(1):27–38.
Kaul S. Choice of optimal anticoagulant to support primary PCI: out with the new, in with the old. J Am Coll Cardiol. 2015;65(1):39–42.
Capodanno D, et al. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary PCI: an updated meta-analysis of 10,350 patients from five randomized clinical trials. Eur Heart J Acute Cardiovasc Care. 2015. A recent meta-analysis of 5 large trials aimed to examine the impact of bailout versus routine GPI use in STEMI.
Cassese S et al. Bivalirudin versus heparin in patients treated with percutaneous coronary intervention: a meta-analysis of randomised trials. EuroIntervention. 2015;11(2):196–203.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Jad Raffoul, Ammar Nasir, and Andrew J. P. Klein each declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Coronary Artery Disease
Rights and permissions
About this article

Cite this article
Raffoul, J., Nasir, A. & Klein, A.J.P. Antithrombotic Selection in ST-Segment Elevation Myocardial Infarction: a Year in Review. Curr Treat Options Cardio Med 18, 53 (2016). https://doi.org/10.1007/s11936-016-0473-7
Published:
DOI: https://doi.org/10.1007/s11936-016-0473-7