
Abstract
Purpose of review
Therapeutic options for the management of lower urinary tract symptoms (LUTS) secondary to benign prostatic enlargement (BPE) have considerably increased in recent years. However, the ideal timing to initiate medical treatment of LUTS/BPE has not been fully established. The aim of this review was to systematically collect available evidence on the influence of early treatment on the natural history of LUTS/BPE patients.
Recent Findings
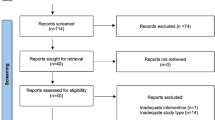
A systematic literature search from January 1996 until April 2018 was performed by combining the following MESH terms: Lower Urinary Tract Symptoms, Benign Prostatic Enlargement, male, medical treatment, surgical treatment, early treatment/intervention, and early intervention/treatment. The Medline, PubMed, and Scopus databases were searched. Each article title and abstract was reviewed for relevance and appropriateness with regard to the topic of this review. In recent years, the medical armamentarium for the management of LUTS secondary to BPE has been extensively implemented, significantly improving treatment outcomes and markedly reducing the need for BPE surgery. Early intervention in patients at risk for disease progression may offer better clinical outcomes compared to a deferred approach. However, evidences supporting early treatment are scarce, and criteria to discriminate patients that could mostly benefit from immediate treatment remain poorly defined. Moreover, as a result of delayed surgery after prolonged medical treatment, patients undergoing surgical relief show larger prostates, older age, and comorbidities. Nevertheless, technological advancements in surgical techniques have largely counterweighed this critical scenario, and commonly, a non-pejorative trend has been reported in perioperative complications.
Summary
The timeliest moment to start a medical treatment in LUTS/BPE patients is still undefined, and unexpectedly, peer-reviewed evidence remains scarce. Further studies are awaited to better discriminate patients who mostly benefit from early treatment of LUTS/BPE.
Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major Importance
De Nunzio C, Presicce F, Tubaro A. Combination therapies for improved management of lower urinary tract symptoms/benign prostatic hyperplasia. Drugs Today (Barc). 2016;52(9):501–17.
AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: diagnosis and treatment recommendations. J Urol. 2003;170:530–47.
De Nunzio C, Presicce F, Pirozzi L, Castellan P, Schips L, Cindolo L, et al. The current indications and the benefits of combining a β3-agonist with an anticholinergic for the treatment of OAB. Curr Drug Targets. 2015;16:1198–206.
Pirozzi L, Sountoulides P, Castellan P, Presicce F, Lombardo R, Romero M, et al. Current pharmacological treatment for male LUTS due to BPH: dutasteride or finasteride? Curr Drug Targets. 2015;16:1165–71.
Krambeck AE, Jacobson DJ, McGree ME, Lightner DJ, Lieber MM, Jacobsen SJ, et al. Effectiveness of medical and surgical therapies for lower urinary tract symptoms in the community setting. BJU Int. 2012;110(9):1332–7.
Crawford ED, Wilson SS, McConnell JD, Slawin KM, Lieber MC, Smith JA, et al. Baseline factors as predictors of clinical progression of benign prostatic hyperplasia in men treated with placebo. J Urol. 2006;175(4):1422–7.
Roehrborn CG, Barkin J, Siami P, Tubaro A, Wilson TH, Morrill BB, et al. Clinical outcomes after combined therapy with dutasteride plus tamsulosin or either monotherapy in men with benign prostatic hyperplasia (BPH) by baseline characteristics: 4-year results from the randomized, double-blind Combination of Avodart and Tamsulosin (CombAT) trial. BJU Int. 2011;107(6):946–54.
Roehrborn CG, Oyarzabal Perez I, Roos EP, Calomfirescu N, Brotherton B, Wang F, et al. Efficacy and safety of a fixed-dose combination of dutasteride and tamsulosin treatment (Duodart(®) ) compared with watchful waiting with initiation of tamsulosin therapy if symptoms do not improve, both provided with lifestyle advice, in the management of treatment-naïve men with moderately symptomatic benign prostatic hyperplasia: 2-year CONDUCT study results. BJU Int. 2015;116(3):450–9.
•• Roehrborn CG, Oyarzabal Perez I, Roos EP, Calomfirescu N, Brotherton B, Palacios JM, et al. Can we use baseline characteristics to assess which men with moderately symptomatic benign prostatic hyperplasia at risk of progression will benefit from treatment? A post hoc analysis of data from the 2-year CONDUCT study. World J Urol. 2017;35(3):421–7. Although this is just a subanalysis, it provides evidence that no treatment is necessary in patient with mild LUTS and no bother.
Souverein PC, Erkens JA, de la Rosette JJ, Leufkens HG, Herings RM. Drug treatment of benign prostatic hyperplasia and hospital admission for BPH-related surgery. Eur Urol. 2003;43:528–34.
Malaeb BS, Yu X, McBean AM, Elliott SP. National trends in surgical therapy for benign prostatic hyperplasia in the United States (2000-2008). Urology. 2012;79:1111–6.
Vela-Navarrete R, Gonzalez-Enguita C, Garcia-Cardoso JV, Manzarbeitia F, Sarasa-Corral JL, Granizo JJ. The impact of medical therapy on surgery for benign prostatic hyperplasia: a study comparing changes in a decade (1992-2002). BJU Int. 2005;96:1045–8.
Izard J, Nickel JC. Impact of medical therapy on transurethral resection of the prostate: two decades of change. BJU Int. 2011;108:89–93.
• Cindolo L, Pirozzi L, Fanizza C, Romero M, Sountoulides P, Roehrborn CG, et al. Actual medical management of lower urinary tract symptoms related to benign prostatic hyperplasia: temporal trends of prescription and hospitalization rates over 5 years in a large population of Italian men. Int Urol Nephrol. 2014;46:695–701. This paper provides evidence that lack of adherence to pharmacological treatment of BPH results in a higher risk of hospital admission for patients with BPH.
Choi SY, Kim TH, Myung SC, Moon YT, Kim KD, Kim YS, et al. Impact of changing trends in medical therapy on surgery for benign prostatic hyperplasia over two decades. Korean J Urol. 2012;53:23–8.
Elkoushy MA, Elshal AM, Elhilali MM. Changing patients’ profile presenting for surgical management of benign prostatic hyperplasia over the past 16 years: a single-centre perspective. Can Urol Assoc J. 2015;9:372–8.
Mayer EK, Kroeze SG, Chopra S, Bottle A, Patel A. Examining the ‘gold standard’: a comparative critical analysis of three consecutive decades of monopolar transurethral resection of the prostate (TURP) outcomes. BJU Int. 2012;110(11):1595–601.
Borth CS, Beiko DT, Nickel JC. Impact of medical therapy on transurethral resection of the prostate: a decade of change. Urology. 2001;57:1082–6.
• Flanigan RC, Reda DJ, Wasson JH, Anderson RJ, Abdellatif M, Bruskewitz RC. 5-year outcome of surgical resection and watchful waiting for men with moderately symptomatic benign prostatic hyperplasia: a Department of Veterans Affairs cooperative study. J Urol. 1998;160:12–7. A unique study of immediate versus delayed surgery for BPH.
He LY, Zhang YC, He JL, Li LX, Wang Y, Tang J, et al. The effect of immediate surgical bipolar plasmakinetic transurethral resection of the prostate on prostatic hyperplasia with acute urinary retention. Asian J Androl. 2016;18:134–9.
Reich O, Gratzke C, Bachmann A, Seitz M, Schlenker B, Hermanek P, et al. Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. J Urol. 2008;180:246–9.
Djavan B, Madersbacher S, Klingler C, Marberger M. Urodynamic assessment of patients with acute urinary retention: is treatment failure after prostatectomy predictable? J Urol. 1997;158:1829–33.
Negro CL, Muir GH. Chronic urinary retention in men: how we define it, and how does it affect treatment outcome. BJU Int. 2012;110:1590–4.
Van Koeveringe GA, Rademakers KL. Factors impacting bladder underactivity and clinical implications. Minerva Urol Nefrol. 2015;67:139–48.
Blatt AH, Brammah S, Tse V, Chan L. Transurethral prostate resection in patients with hypocontractile detrusor—what is the predictive value of ultrastructural detrusor changes? J Urol. 2012;188:2294–9.
Oelke M, Kirschner-Hermanns R, Thiruchelvam N, Heesakkers J. Can we identify men who will have complications from benign prostatic obstruction (BPO)? ICI-RS 2011. Neurourol Urodyn. 2012;31:322–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Fabrizio Presicce, Cosimo De Nunzio, and Andrea Tubaro each declare no potential conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Benign Prostatic Hyperplasia
Rights and permissions
About this article

Cite this article
Presicce, F., De Nunzio, C. & Tubaro, A. Clinical Implications for the Early Treatment of Benign Prostatic Enlargement (BPE): a Systematic Review. Curr Urol Rep 19, 70 (2018). https://doi.org/10.1007/s11934-018-0823-y
Published:
DOI: https://doi.org/10.1007/s11934-018-0823-y