
Abstract
Purpose of Review
In this review, we examine the central role of echocardiography in the diagnosis, prognosis, and management of infective endocarditis (IE).
Recent Findings
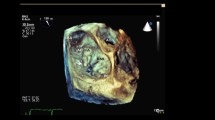
2D transthoracic echocardiography (TTE) and transesophageal echocardiography TEE have complementary roles and are unequivocally the mainstay of diagnostic imaging in IE. The advent of 3D and multiplanar imaging have greatly enhanced the ability of the imager to evaluate cardiac structure and function. Technologic advances in 3D imaging allow for the reconstruction of realistic anatomic images that in turn have positively impacted IE-related surgical planning and intervention. CT and metabolic imaging appear to be emerging as promising ancillary diagnostic tools that could be deployed in select scenarios to circumvent some of the limitations of echocardiography.
Summary
Our review summarizes the indispensable and central role of various echocardiographic modalities in the management of infective endocarditis. The complementary role of 2D TTE and TEE are discussed and areas where 3D TEE offers incremental value highlighted. An algorithm summarizing a contemporary approach to the workup of endocarditis is provided and major societal guidelines for timing of surgery are reviewed.






Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Pant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. 2015;65(19):2070–6.
Bor DH, Woolhandler S, Nardin R, Brusch J, Himmelstein DU. Infective endocarditis in the U.S., 1998-2009: a nationwide study. PLoS One. 2013;8(3):e60033.
Cahill TJ, Baddour LM, Habib G, Hoen B, Salaun E, Pettersson GB, et al. Challenges in infective endocarditis. J Am Coll Cardiol. 2017;69(3):325–44.
Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633–8.
Chirillo F, Pedrocco A, De Leo A, Bruni A, Totis O, Meneghetti P, et al. Impact of harmonic imaging on transthoracic echocardiographic identification of infective endocarditis and its complications. Heart. 2005;91(3):329–33.
Jassal DS, Aminbakhsh A, Fang T, Shaikh N, Embil JM, Mackenzie GS, et al. Diagnostic value of harmonic transthoracic echocardiography in native valve infective endocarditis: comparison with transesophageal echocardiography. Cardiovasc Ultrasound. 2007;5:20.
•• Pfister R, Betton Y, Freyhaus HT, Jung N, Baldus S, Michels G. Three-dimensional compared to two-dimensional transesophageal echocardiography for diagnosis of infective endocarditis. Infection. 2016;44(6):725–31. This study helped illustrate the incremental benefit of 3D TEE in cases of prosthetic heart valve endocarditis.
Perez-Vazquez A, Farinas MC, Garcia-Palomo JD, Bernal JM, Revuelta JM, Gonzalez-Macias J. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved? Arch Intern Med. 2000;160(8):1185–91.
•• Habets J, Tanis W, Reitsma JB, van den Brink RB, Mali WP, Chamuleau SA, et al. Are novel non-invasive imaging techniques needed in patients with suspected prosthetic heart valve endocarditis? A systematic review and meta-analysis. Eur Radiol. 2015;25(7):2125–33. This meta-analysis and review helped guide us through a basic question, the role of 3D TEE and other new imaging modalities in prosthetic heart valve endocarditis.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57–185.
• Tanis W, Teske AJ, van Herwerden LA, Chamuleau S, Meijboom F, Budde RP, et al. The additional value of three-dimensional transesophageal echocardiography in complex aortic prosthetic heart valve endocarditis. Echocardiography. 2015;32(1):114–25. This study helped assess the importance of 3D TEE in the setting of prosthetic heart valves.
San Roman JA, Vilacosta I, Lopez J, Revilla A, Arnold R, Sevilla T, et al. Role of transthoracic and transesophageal echocardiography in right-sided endocarditis: one echocardiographic modality does not fit all. J Am Soc Echocardiogr. 2012;25(8):807–14.
Grammes JA, Schulze CM, Al-Bataineh M, Yesenosky GA, Saari CS, Vrabel MJ, et al. Percutaneous pacemaker and implantable cardioverter-defibrillator lead extraction in 100 patients with intracardiac vegetations defined by transesophageal echocardiogram. J Am Coll Cardiol. 2010;55(9):886–94.
Vilacosta I, Olmos C, de Agustin A, Lopez J, Islas F, Sarria C, et al. The diagnostic ability of echocardiography for infective endocarditis and its associated complications. Expert Rev Cardiovasc Ther. 2015;13(11):1225–36.
Vilacosta I, Sarria C, San Roman JA, Jimenez J, Castillo JA, Iturralde E, et al. Usefulness of transesophageal echocardiography for diagnosis of infected transvenous permanent pacemakers. Circulation. 1994;89(6):2684–7.
Xie J, Liu S, Yang J, Xu J, Zhu G. Inaccuracy of transthoracic echocardiography for the identification of right-sided vegetation in patients with no history of intravenous drug abuse or cardiac device insertion. J Int Med Res. 2014;42(3):837–48.
Naqvi TZ, Rafie R, Ghalichi M. Real-time 3D TEE for the diagnosis of right-sided endocarditis in patients with prosthetic devices. JACC Cardiovasc Imaging. 2010;3(3):325–7.
Sungur A, Hsiung MC, Meggo Quiroz LD, Oz TK, Haj Asaad A, Joshi D, et al. The advantages of live/real time three-dimensional transesophageal echocardiography in the assessment of tricuspid valve infective endocarditis. Echocardiography. 2014;31(10):1293–309.
Anwar AM, Nosir YF, Alasnag M, Chamsi-Pasha H. Real time three-dimensional transesophageal echocardiography: a novel approach for the assessment of prosthetic heart valves. Echocardiography. 2014;31(2):188–96.
Tanis W, Budde RP, van der Bilt IA, Delemarre B, Hoohenkerk G, van Rooden JK, et al. Novel imaging strategies for the detection of prosthetic heart valve obstruction and endocarditis. Neth Hear J. 2016;24(2):96–107.
Barbetseas J, Nagueh SF, Pitsavos C, Toutouzas PK, Quinones MA, Zoghbi WA. Differentiating thrombus from pannus formation in obstructed mechanical prosthetic valves: an evaluation of clinical, transthoracic and transesophageal echocardiographic parameters. J Am Coll Cardiol. 1998;32(5):1410–7.
Teshima H, Hayashida N, Yano H, Nishimi M, Tayama E, Fukunaga S, et al. Obstruction of St Jude Medical valves in the aortic position: histology and immunohistochemistry of pannus. J Thorac Cardiovasc Surg. 2003;126(2):401–7.
Huang G, Schaff HV, Sundt TM, Rahimtoola SH. Treatment of obstructive thrombosed prosthetic heart valve. J Am Coll Cardiol. 2013;62(19):1731–6.
Gursoy OM, Karakoyun S, Kalcik M, Ozkan M. The incremental value of RT three-dimensional TEE in the evaluation of prosthetic mitral valve ring thrombosis complicated with thromboembolism. Echocardiography. 2013;30(7):E198–201.
Bonnichsen CR, Pellikka PA. Prosthetic valve thrombus versus pannus: progress with imaging. Circ Cardiovasc Imaging. 2015;8(12):e004283.
Saby L, Laas O, Habib G, Cammilleri S, Mancini J, Tessonnier L, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol. 2013;61(23):2374–82.
Latib A, Naim C, De Bonis M, Sinning JM, Maisano F, Barbanti M, et al. TAVR-associated prosthetic valve infective endocarditis: results of a large, multicenter registry. J Am Coll Cardiol. 2014;64(20):2176–8.
Cacoub P, Leprince P, Nataf P, Hausfater P, Dorent R, Wechsler B, et al. Pacemaker infective endocarditis. Am J Cardiol. 1998;82(4):480–4.
Massoure PL, Reuter S, Lafitte S, Laborderie J, Bordachard P, Clementy J, et al. Pacemaker endocarditis: clinical features and management of 60 consecutive cases. Pacing Clin Electrophysiol. 2007;30(1):12–9.
Victor F, De Place C, Camus C, Le Breton H, Leclercq C, Pavin D, et al. Pacemaker lead infection: echocardiographic features, management, and outcome. Heart. 1999;81(1):82–7.
Klug D, Lacroix D, Savoye C, Goullard L, Grandmougin D, Hennequin JL, et al. Systemic infection related to endocarditis on pacemaker leads: clinical presentation and management. Circulation. 1997;95(8):2098–107.
Korkeila PJ, Saraste MK, Nyman KM, Koistinen J, Lund J, Juhani Airaksinen KE. Transesophageal echocardiography in the diagnosis of thrombosis associated with permanent transvenous pacemaker electrodes. Pacing Clin Electrophysiol. 2006;29(11):1245–50.
Schnabel R, Khaw AV, von Bardeleben RS, Strasser C, Kramm T, Meyer J, et al. Assessment of the tricuspid valve morphology by transthoracic real-time-3D-echocardiography. Echocardiography. 2005;22(1):15–23.
Seo Y, Ishizu T, Nakajima H, Sekiguchi Y, Watanabe S, Aonuma K. Clinical utility of 3-dimensional echocardiography in the evaluation of tricuspid regurgitation caused by pacemaker leads. Circ J. 2008;72(9):1465–70.
Mihl C, Geyik Z, Cheriex EC, van Opstal JM. A challenging lead endocarditis. Eur J Echocardiogr. 2010;11(2):E1.
Gersony WM, Hayes CJ, Driscoll DJ, Keane JF, Kidd L, O'Fallon WM, et al. Bacterial endocarditis in patients with aortic stenosis, pulmonary stenosis, or ventricular septal defect. Circulation. 1993;87(2 Suppl):I121–6.
Holzer R, de Giovanni J, Walsh KP, Tometzki A, Goh T, Hakim F, et al. Transcatheter closure of perimembranous ventricular septal defects using the amplatzer membranous VSD occluder: immediate and midterm results of an international registry. Catheter Cardiovasc Interv. 2006;68(4):620–8.
Wang J, Zuo J, Yu S, Yi D, Yang X, Zhu X, et al. Effectiveness and safety of transcatheter closure of perimembranous ventricular septal defects in adults. Am J Cardiol. 2016;117(6):980–7.
Wang L, Cao S, Li J, Yang L, Liu Y, Ren J, et al. Transcatheter closure of congenital perimembranous ventricular septal defect in children using symmetric occluders: an 8-year multiinstitutional experience. Ann Thorac Surg. 2012;94(2):592–8.
Edwards AD, Vickers MA, Morgan CJ. Infective endocarditis affecting the eustachian valve. Br Heart J. 1986;56(6):561–2.
Sawhney N, Palakodeti V, Raisinghani A, Rickman LS, DeMaria AN, Blanchard DG. Eustachian valve endocarditis: a case series and analysis of the literature. J Am Soc Echocardiogr. 2001;14(11):1139–42.
San Roman JA, Vilacosta I, Sarria C, Garcimartin I, Rollan MJ, Fernandez-Aviles F. Eustachian valve endocarditis: is it worth searching for? Am Heart J. 2001;142(6):1037–40.
Kottam A, Kaur R, Bhandare D, Zmily H, Bheemreddy S, Brar H, et al. Actinomycotic endocarditis of the eustachian valve: a rare case and a review of the literature. Tex Heart Inst J. 2015;42(1):44–9.
Kumar KR, Haider S, Sood A, Mahmoud KA, Mostafa A, Afonso LC, et al. Right-sided endocarditis: eustachian valve and coronary sinus involvement. Echocardiography. 2017;34(1):143–4.
Pellicelli AM, Pino P, Terranova A, D'Ambrosio C, Soccorsi F. Eustachian valve endocarditis: a rare localization of right side endocarditis. A case report and review of the literature. Cardiovasc Ultrasound. 2005;3:30.
Pasha AK, Snyder BA, Zangeneh TT, Thompson JL, Sobonya RE, Abidov A. A distinctly rare case of candida endocarditis involving the bioprosthetic pulmonary and the Eustachian valve diagnosed on 3D transesophageal echocardiography. Echocardiography. 2015;32(3):607–9.
Kearney RA, Eisen HJ, Wolf JE. Nonvalvular infections of the cardiovascular system. Ann Intern Med. 1994;121(3):219–30.
Tahara M, Nagai T, Takase Y, Takiguchi S, Tanaka Y, Kunihara T, et al. Primary mural endocarditis without valvular involvement. J Ultrasound Med. 2017;36(3):659–64.
Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2017;30(4):303–71.
Zoghbi WA, Chambers JB, Dumesnil JG, Foster E, Gottdiener JS, Grayburn PA, et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2009;22(9):975–1014. quiz 82-4
Daniel WG, Mugge A, Martin RP, Lindert O, Hausmann D, Nonnast-Daniel B, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med. 1991;324(12):795–800.
Thomas D, Desruennes M, Jault F, Isnard R, Gandjbakhch I. Cardiac and extracardiac abscesses in bacterial endocarditis. Arch Mal Coeur Vaiss. 1993;86(12 Suppl):1825–35.
Murdoch DR, Corey GR, Hoen B, Miro JM, Fowler VG Jr, Bayer AS, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the international collaboration on endocarditis-prospective cohort study. Arch Intern Med. 2009;169(5):463–73.
Cosmi JE, Tunick PA, Kronzon I. Mortality in patients with paravalvular abscess diagnosed by transesophageal echocardiography. J Am Soc Echocardiogr. 2004;17(7):766–8.
Penugonda N, Duncan K, Afonso L. Complex endocarditis in an immunocompromised host: the role of three-dimensional echocardiography. J Am Soc Echocardiogr. 2007;20(11):1314 e9-11.
Walker N, Bhan A, Desai J, Monaghan MJ. Myocardial abscess: a rare complication of valvular endocarditis demonstrated by 3D contrast echocardiography. Eur J Echocardiogr. 2010;11(10):E37.
Chakrabarti J. Diagnostic evaluation of myocardial abscesses. A new look at an old problem. Int J Cardiol. 1995;52(3):189–96.
Bachour K, Zmily H, Kizilbash M, Awad K, Hourani R, Hammad H, et al. Valvular perforation in left-sided native valve infective endocarditis. Clin Cardiol. 2009;32(12):E55–62.
De Castro S, Cartoni D, d'Amati G, Beni S, Yao J, Fiorell M, et al. Diagnostic accuracy of transthoracic and multiplane transesophageal echocardiography for valvular perforation in acute infective endocarditis: correlation with anatomic findings. Clin Infect Dis. 2000;30(5):825–6.
Thompson KA, Shiota T, Tolstrup K, Gurudevan SV, Siegel RJ. Utility of three-dimensional transesophageal echocardiography in the diagnosis of valvular perforations. Am J Cardiol. 2011;107(1):100–2.
Azevedo O, Ferreira F, Guardado J, Duraes C, Quelhas I, Pereira A, et al. Mitral and aortic valve aneurysms secondary to infective endocarditis: impressive images of a rare echocardiographic finding. Eur J Echocardiogr. 2010;11(7):E28.
Hotchi J, Hoshiga M, Okabe T, Nakakoji T, Ishihara T, Katsumata T, et al. Impressive echocardiographic images of a mitral valve aneurysm. Circulation. 2011;123(14):e400–2.
Kawai S, Oigawa T, Sunayama S, Yamaguchi H, Okada R, Hosoda Y, et al. Mitral valve aneurysm as a sequela of infective endocarditis: review of pathologic findings in Japanese cases. J Cardiol. 1998;31(Suppl 1):19–33. discussion 4-6
Vilacosta I, San Roman JA, Sarria C, Iturralde E, Graupner C, Batlle E, et al. Clinical, anatomic, and echocardiographic characteristics of aneurysms of the mitral valve. Am J Cardiol. 1999;84(1):110–3. A9
Vijay SK, Tiwari BC, Misra M, Dwivedi SK. Incremental value of three-dimensional transthoracic echocardiography in the assessment of ruptured aneurysm of anterior mitral leaflet. Echocardiography. 2014;31(1):E24–6.
Silbiger JJ, Krasner A, Chikwe J, Marino T, Mathewkutty S, Marcali M, et al. Pseudoaneurysm formation in infective endocarditis. Echocardiography. 2013;30(10):E319–21.
Sudhakar S, Sewani A, Agrawal M, Uretsky BF. Pseudoaneurysm of the mitral-aortic intervalvular fibrosa (MAIVF): a comprehensive review. J Am Soc Echocardiogr. 2010;23(10):1009–18.
Afridi I, Apostolidou MA, Saad RM, Zoghbi WA. Pseudoaneurysms of the mitral-aortic intervalvular fibrosa: dynamic characterization using transesophageal echocardiographic and Doppler techniques. J Am Coll Cardiol. 1995;25(1):137–45.
Kassim TA, Lowery RC, Nasur A, Corrielus S, Weissman G, Sears-Rogan P, et al. Pseudoaneurysm of mitral-aortic intervalvular fibrosa: two case reports and review of literature. Eur J Echocardiogr. 2010;11(3):E7.
Anguera I, Miro JM, San Roman JA, de Alarcon A, Anguita M, Almirante B, et al. Periannular complications in infective endocarditis involving prosthetic aortic valves. Am J Cardiol. 2006;98(9):1261–8.
Yared K, Solis J, Passeri J, King ME, Levine RA. Three-dimensional echocardiographic assessment of acquired left ventricular to right atrial shunt (Gerbode defect). J Am Soc Echocardiogr. 2009;22(4):435.e1-3.
Thuny F, Grisoli D, Collart F, Habib G, Raoult D. Management of infective endocarditis: challenges and perspectives. Lancet. 2012;379(9819):965–75.
Taskesen T, Goldberg SL, Gill EA. Role of three-dimensional echocardiography in management of acquired intracardiac shunts. Echocardiography. 2014;31(8):E250–3.
Saric M, Armour AC, Arnaout MS, Chaudhry FA, Grimm RA, Kronzon I, et al. Guidelines for the use of echocardiography in the evaluation of a cardiac source of embolism. J Am Soc Echocardiogr. 2016;29(1):1–42.
Edoute Y, Haim N, Rinkevich D, Brenner B, Reisner SA. Cardiac valvular vegetations in cancer patients: a prospective echocardiographic study of 200 patients. Am J Med. 1997;102(3):252–8.
Roldan CA, Shively BK, Crawford MH. An echocardiographic study of valvular heart disease associated with systemic lupus erythematosus. N Engl J Med. 1996;335(19):1424–30.
Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. 2016;387(10021):882–93.
Deprele C, Berthelot P, Lemetayer F, Comtet C, Fresard A, Cazorla C, et al. Risk factors for systemic emboli in infective endocarditis. Clin Microbiol Infect. 2004;10(1):46–53.
• Berdejo J, Shibayama K, Harada K, Tanaka J, Mihara H, Gurudevan SV, et al. Evaluation of vegetation size and its relationship with embolism in infective endocarditis: a real-time 3-dimensional transesophageal echocardiography study. Circ Cardiovasc Imaging. 2014;7(1):149–54. The evaluation of vegetation size and its importance in embolic risk was underscored in this study. Incremental value of 3D TEE was highlighted.
• Utsunomiya H, Berdejo J, Kobayashi S, Mihara H, Itabashi Y, Shiota T. Evaluation of vegetation size and its relationship with septic pulmonary embolism in tricuspid valve infective endocarditis: a real time 3DTEE study. Echocardiography. 2017;34(4):549–56. This recent study helped illustrate the incremental role of 3D TEE even in cases of RSE, in this case for the assesment of risk of pulmonary thromboembolic events.
Kang DH. Timing of surgery in infective endocarditis. Heart. 2015;101(22):1786–91.
•• Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC guidelines for the management of infective endocarditis. The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). G Ital Cardiol (Rome). 2016;17(4):277–319. The role of surgery in infective endocarditis was underscored and how it differs from the ACC/AHA.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):2438–88.
Fagman E, Perrotta S, Bech-Hanssen O, Flinck A, Lamm C, Olaison L, et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur Radiol. 2012;22(11):2407–14.
Feuchtner GM, Stolzmann P, Dichtl W, Schertler T, Bonatti J, Scheffel H, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol. 2009;53(5):436–44.
Habets J, Tanis W, van Herwerden LA, van den Brink RB, Mali WP, de Mol BA, et al. Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis. Int J Cardiovasc Imaging. 2014;30(2):377–87.
Erba PA, Conti U, Lazzeri E, Sollini M, Doria R, De Tommasi SM, et al. Added value of 99mTc-HMPAO-labeled leukocyte SPECT/CT in the characterization and management of patients with infectious endocarditis. J Nucl Med. 2012;53(8):1235–43.
Pizzi MN, Roque A, Fernandez-Hidalgo N, Cuellar-Calabria H, Ferreira-Gonzalez I, Gonzalez-Alujas MT, et al. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-fluordeoxyglucose positron emission tomography/computed tomography angiography: initial results at an infective endocarditis referral center. Circulation. 2015;132(12):1113–26.
Rouzet F, Chequer R, Benali K, Lepage L, Ghodbane W, Duval X, et al. Respective performance of 18F-FDG PET and radiolabeled leukocyte scintigraphy for the diagnosis of prosthetic valve endocarditis. J Nucl Med. 2014;55(12):1980–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Luis Afonso, Anupama Kottam, Vivek Reddy, and Anirudh Penumetcha declare that they have no conflict of interest.
Human and Animal Rights Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Echocardiography
Electronic Supplementary Material
Fig. S1
Mural endocarditis. Transesophageal echocardiogram bicaval view at 100 degrees showing a large vegetation attached to the right atrial endocardium at the junction of the free wall and right atrial appendage. No valvular vegetations were seen in this patient. Blood culture grew MRSA bacteremia. RAA- right atrial appendage. (JPEG 47 kb)
Fig. S2
Mural Endocarditis. Transesophageal echocardiogram at mid esophageal short axis view showing a thin layer of mural endocarditis along the left atrial wall extending to the interatrial septum. Blood culture grew MRSA bacteremia. (JPEG 41 kb)
Fig. S3
Mitral valve regurgitation. a. Transesophageal echocardiogram in 0 degrees, 4-chamber view at mid esophageal level showing destructive mitral endocarditis. Note flail anterior mitral leaflet and significant malcoaptation. b. Color Doppler shows severe eccentric mitral regurgitation. LA, Left atrium; LV, Left ventricle (JPEG 49 kb)
Fig. S4
Pseudoaneurysm. a. Transesophageal echocardiogram at 170 degrees mid esophageal level showing a large pseudoaneurysm of the mitral-aortic intervalvular fibrosa with arrow present. Echogenicity within the pseudoaneurysm suggests an abscess. b. Communication of pseudoaneurysm with the left ventricular cavity is noted on color Doppler. Also note collapse of aneurysm during diastole and expansion during systole in Fig. A. BPAV, Bioprosthetic aortic valve; LA Left atrium; LV Left ventricle; MAIF Mitral-aortic interannular fibrosa. Blood culture grew MRSA (JPEG 101 kb)
Fig. S5
Marantic endocarditis. a. Transesophageal echocardiogram at 120 degrees mid esophageal left ventricular outflow tract view showing a globular lesion attached to the aortic valve non-coronary cusp b. Similar lesion is found attached to the mitral leaflet tip at 0 degrees with arrow present. AV, Aortic valve; LA, Left atrium; LV, Left ventricle. (JPEG 60 kb)
Fig. S6
Marantic endocarditis. Transthoracic parasternal long axis view showing an echogenic mass attached to the aortic valve. Histopathology suggestive of non-bacterial endocarditis/ marantic endocarditis. LVOT Left ventricular outflow tract. (JPEG 20 kb)
Video 9
Mitral valve perforation. Transesophageal echocardiogram mid esophageal 4 chamber view at 0 degrees showing a large globular vegetation of the posterior mitral leaflet. Color Doppler in systole demonstrates a regurgitant jet through the posterior leaflet suggestive of perforation. (AVI 792 kb)
Video 10
Marantic endocarditis video. Transthoracic parasternal long axis view in Live 3D showing an echogenic mass attached to the aortic valve. Histopathology confirmed non-bacterial endocarditis/ marantic endocarditis. (AVI 260 kb)
Video 1
Prosthetic heart valve endocarditis. Transesophageal echocardiogram, mid esophageal view with biplane imaging showing vegetations of the bioprosthetic mitral valve. Dehiscience of the prosthetic valve with excessive mobility or “rocking” of prosthesis is noted in the orthogonal plane. (AVI 475 kb)
Video 2
Lead endocarditis. Transesophageal echocardiogram; Real time 3D off -axis bicaval view showing multiple mobile vegetations attached to the right atrial portion of the right ventricular lead. Right atrial lead was free of vegetations. Blood culture was positive for vancomycin resistant enterococci (VRE). (AVI 246 kb)
Video 3
Mural endocarditis video. Tranthoracic Real time 3D image of a massive pedunculated vegetation attached to the superior right atrial wall. The lesion prolapses through the tricuspid valve in diastole. Blood cultures grew MRSA. Complete resolution of the vegetation occurred after a course of antibiotics. (AVI 468 kb)
Video 4
Tricuspid valve endocarditis: Tranthoracic parasternal short axis view at the level of aortic valve showing small vegetation attached to the septal tricuspid leaflet. An echolucent area within the septal tricuspid leaflet suggests an area of perforation with resultant severe tricuspid regurgitation. Blood culture grew MRSA. (AVI 1080 kb)
Video 5
Prosthetic valve endocarditis video. Transesophageal echocardiogram at mid esophageal level showing biplane imaging of transcatheter bioprothetic aortic valve (CoreValve). Long axis plane demonstrates a mobile vegetation attached to the prosthetic leaflet. Blood culture grew Vancomycin resistant enterococci. (AVI 1126 kb)
Video 6
Endocarditis of ASD closure device. Transesophageal echocardiogram in bicaval view. Biplane imaging shows an ASD occluder device. Contrast imaging outlines a hypoechoic, gelatinous phlegmon (abscess) attached to the left atrial aspect of the device. Blood culture grew Morganella morganii. (AVI 931 kb)
Video 7
Coronary sinus endocarditis video. Transesophageal echocardiogram at 180 degrees lower esophageal view. Note a long vegetation seated deep in the coronary sinus. (AVI 1115 kb)
Video 8
Aortic valve perforation video. Transesophageal echocardiogram mid esophageal left ventricular outflow tract view at 130 degrees showing aortic valve vegetations involving the right and non-coronary cusps. A small area of perforation is noted in the non-coronary cusp. Two distinct jets of aortic regurgitation through both the commissure and the perforation are noted. Blood culture grew Enterococcus fecalis. (AVI 996 kb)
Marantic endocarditis. Transesophageal echocardiogram at 120 degrees mid esophageal left ventricular outflow tract view showing a globular lesion attached to the aortic valve non-coronary cusp. (AVI 781 kb)
Rights and permissions
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Afonso, L., Kottam, A., Reddy, V. et al. Echocardiography in Infective Endocarditis: State of the Art. Curr Cardiol Rep 19, 127 (2017). https://doi.org/10.1007/s11886-017-0928-9
Published:
DOI: https://doi.org/10.1007/s11886-017-0928-9