
Abstract
Background
Rigid bronchoscopy may be used to relieve acute airway obstruction following induction of anaesthesia and is a recommended option for management of the difficult airway. The ability of anaesthetists to perform rigid bronchoscopy has not been reported. We sought to explore the acquisition of procedural skill in rigid bronchoscopy by anaesthesiologists in a manikin.
Methods
In a prospective interventional study, participants were asked to perform 40 rigid bronchoscopies in a TruCorp AirSim Advance airway manikin, configured to a randomised sequence of easy or difficult laryngoscopic grades to which the participants were blinded. The primary outcome was stabilisation (the attempt after which no further reduction in procedural time occurred). Dental injury and oesophageal intubation were also recorded. Forty anaesthesiologists and 40 unskilled controls (without laryngoscopic skills) participated.
Results
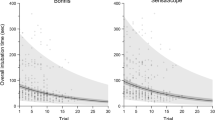
In the easy model, stabilisation occurred at attempt 8 in the anaesthesiology group and 10 in the unskilled controls. In the difficult model, stabilisation occurred at attempt 10 in both groups. Dental injury was less common in the anaesthesiology group. The proportion of participants achieving procedural competency did not differ between groups in either the easy (35/40 vs. 30/40) or difficult model (32/40 vs. 25/40).
Conclusions
This study shows that the technical skill of rigid bronchoscopy can be acquired within 10 repetitions in a manikin model. As procedural competence and complication frequency vary with the laryngoscopic grade of the model, both easy and difficult configurations should be used for training. Advanced laryngoscopic skills are not required prior to training in this technique.





Similar content being viewed by others


Abbreviations
- C&L:
-
Cormack and Lehane
- CUSUM:
-
Cumulative sum method
- SD:
-
Standard deviation
- SEM:
-
Standard error of mean
References
Gardner JC, Royster RL (2011) Airway collapse with an anterior mediastinal mass despite spontaneous ventilation in an adult. Anesth Analg 113(2):239–242
Béchard P, Létourneau L, Lacasse Y, Côté D, Bussières JS (2004) Perioperative cardiorespiratory complications in adults with mediastinal MassIncidence and risk factors. J Am Soc Anesthesiol 100(4):826–834
Erdös G, Tzanova I (2009) Perioperative anaesthetic management of mediastinal mass in adults. Eur J Anaesthesiol (EJA) 26(8):627–632
Blank RS, de Souza DG (2011) Anesthetic management of patients with an anterior mediastinal mass: continuing professional development. Can J Anesth 58(9):853–867
Cook T, Woodall N, Frerk C (2011) Major complications of airway management in the UK: results of the fourth National Audit Project of the Royal College of Anaesthetists and the difficult airway society. Part 1: anaesthesia. Br J Anaesth 106(5):617–631
Cook T, Morgan P, Hersch P (2011) Equal and opposite expert opinion. Airway obstruction caused by a retrosternal thyroid mass: management and prospective international expert opinion. Anaesthesia 66(9):828–836
Ferrari LR, Bedford RF (1990) General anesthesia prior to treatment of anterior mediastinal masses in pediatric cancer patients. Anesthesiology 72(6):991–995
Ernst A, Wahidi MM, Read CA, Buckley JD, Addrizzo-Harris DJ, Shah PL, Herth FJ, de Hoyos Parra A, Ornelas J, Yarmus L, Silvestri GA (2015) Adult bronchoscopy training: current state and suggestions for the future: CHEST expert panel report. Chest 148(2):321–332. https://doi.org/10.1378/chest.14-0678
McNarry A, Dovell T, Dancey F, Pead M (2007) Perception of training needs and opportunities in advanced airway skills: a survey of British and Irish trainees. Eur J Anaesthesiol 24(06):498–504
Marshall S, Chrimes N (2016) Time for a breath of fresh air: rethinking training in airway management. Anaesthesia 71(11):1259–1264
Ramaswamy AH, Kurdi MS, Shaikh SI, Deva RS, Raza SU (2014) Awake rigid bronchoscopy for post intubation tracheal stenosis. Anaesth Pain Intensive Care 18:299–301
Wong DT, Prabhu AJ, Coloma M, Imasogie N, Chung FF (2003) What is the minimum training required for successful cricothyroidotomy?: a study in mannequins. Anesthesiology 98(2):349–353
de Oliveira Filho GR (2002) The construction of learning curves for basic skills in anesthetic procedures: an application for the cumulative sum method. Anesth Analg 95(2):411–416
Bould MD, Crabtree NA, Naik VN (2009) Assessment of procedural skills in anaesthesia. Br J Anaesth 103(4):472–483. https://doi.org/10.1093/bja/aep241
Salud LH, Peniche AR, Salud JC, de Hoyos AL, Pugh CM (2011) Toward a simulation and assessment method for the practice of camera-guided rigid bronchoscopy. Stud Health Technol Inform 163:535–541
Salah N, Mhuircheartaigh RN, Hayes N, McCaul C (2010) A comparison of four techniques of emergency transcricoid oxygenation in a manikin. Anesth Analg 110(4):1083–1085. https://doi.org/10.1213/ANE.0b013e3181d27eb2
Margarido CB, Arzola C, Balki M, Carvalho JC (2010) Anesthesiologists’ learning curves for ultrasound assessment of the lumbar spine. Can J Anesth 57(2):120–126
Ku CM (2011) Anesthesia for patients with mediastinal masses. In: Principles and practice of anesthesia for thoracic surgery. Springer, pp 201–210
Mahmood K, Wahidi MM, Osann KE, Coles K, Shofer SL, Volker EE, Davoudi M (2016) Development of a tool to assess basic competency in the performance of rigid bronchoscopy. Ann Am Thorac Soc 13(4):502–511. https://doi.org/10.1513/AnnalsATS.201509-593OC
Ishman SL, Brown DJ, Boss EF, Skinner ML, Tunkel DE, Stavinoha R, Lin SY (2010) Development and pilot testing of an operative competency assessment tool for pediatric direct laryngoscopy and rigid bronchoscopy. Laryngoscope 120(11):2294–2300. https://doi.org/10.1002/lary.21067
Huret B, Perez T, Dhalluin X, Dewavrin F, Ramon PP, Fournier C (2015) Treatment of malignant central airways obstruction by rigid bronchoscopy. Rev Mal Respir 32(5):477–484. https://doi.org/10.1016/j.rmr.2013.09.018
Jung B, Murgu S, Colt H (2011) Rigid bronchoscopy for malignant central airway obstruction from small cell lung cancer complicated by SVC syndrome. Ann Thorac Cardiovasc Surg 17(1):53–57
Funding
This study was funded by the College of Anaesthetists of Ireland.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Royds, J., Buckley, M.A., Campbell, M.D. et al. Achieving proficiency in rigid bronchoscopy—a study in manikins. Ir J Med Sci 188, 979–986 (2019). https://doi.org/10.1007/s11845-018-1944-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-018-1944-5