
Introduction
Acute cardiogenic pulmonary edema (ACPE) is among the most common diseases observed in emergency departments. It is responsible for more than 1 million visits in the US with a remarkable in-hospital mortality ranging from 10 to 15%.
Medical treatment consists of preload and afterload reduction with vasodilators, and diuretics in fluid-overloaded patients. Response to medical treatment is generally observed after several hours, while the beneficial effects of non-invasive ventilation (NIV) or continuous positive airway pressure (CPAP) [1] on both cardiac and respiratory function are immediate and rapidly correct hypoxemia and respiratory distress. Therefore, NIV/CPAP is the mainstay of ACPE treatment with a major clinical impact on disease course and mortality [2].
Why it works
The lung
Hypoxemia observed in ACPE is mainly due to collapsed alveoli that do not participate in gas exchange; this intrapulmonary shunt mechanism of hypoxemia responds poorly to oxygen administration.
In this case, the best way to improve gas exchange is alveolar recruitment induced by positive pressure application, which allows reopening of collapsed units (inspiratory pressure) and prevents derecruitement (positive end expiratory pressure, PEEP). More alveoli participate in gas exchange, thus leading to improved oxygenation due to shunt effect decrease with improved ventilation/perfusion ratio [3].
The heart
The beneficial effects of positive pressure application on the circulatory system are twofold: pre-load decrease and after-load decrease.
Pre-load The increased intrathoracic pressure induced by the application of positive pressure decreases venous return that is usually elevated in patients with heart failure, especially in those with reduced ejection fraction.
After-load Positive pressure application leads to remarkable reduction of inspiratory effort, thereby decreasing the negative pleural pressure during inspiration. This in turn leads to a parallel decrease of left ventricular (LV) transmural pressure, which is intraventricular pressure minus the negative pleural pressure [3].
NIV in practice, how to do NIV/CPAP in ACPE
-
1.
Ensure the availability of equipment and human resources (trained personnel) NIV/CPAP must be performed by trained physicians and nurses. ACPE patients clearly benefit from early NIV/CPAP. This is why prehospital and emergency department NIV/CPAP is appropriate and effective.
-
2.
Ask yourself what to do if NIV/CPAP fails Is your patient a candidate for invasive mechanical ventilation in case of NIV/CPAP failure? Or is NIV/CPAP the maximal therapeutic effort you will consider? If the patient is rapidly deteriorating, NIV/CPAP might be started along with medical treatment, and the decision on more aggressive options delayed. Once the patient is stabilized on NIV/CPAP, you should gather all the information and advice (intensivist, cardiologist, treating physician) needed to decide your strategy in case of NIV/CPAP failure.
-
3.
Decide whether to apply CPAP or NIV (see Fig. 1) In ACPE patients, CPAP is as effective as NIV even in patients with acute respiratory acidosis on admission. CPAP is easier to perform, requires less technical equipment, and evidence in the literature suggests it may be better than NIV in ACPE [2]. Our advice in ACPE is in general to choose CPAP over NIV. Severe COPD patients where a diagnosis of ACPE vs COPD decompensation is not immediately clear should be treated with NIV.
Fig. 1 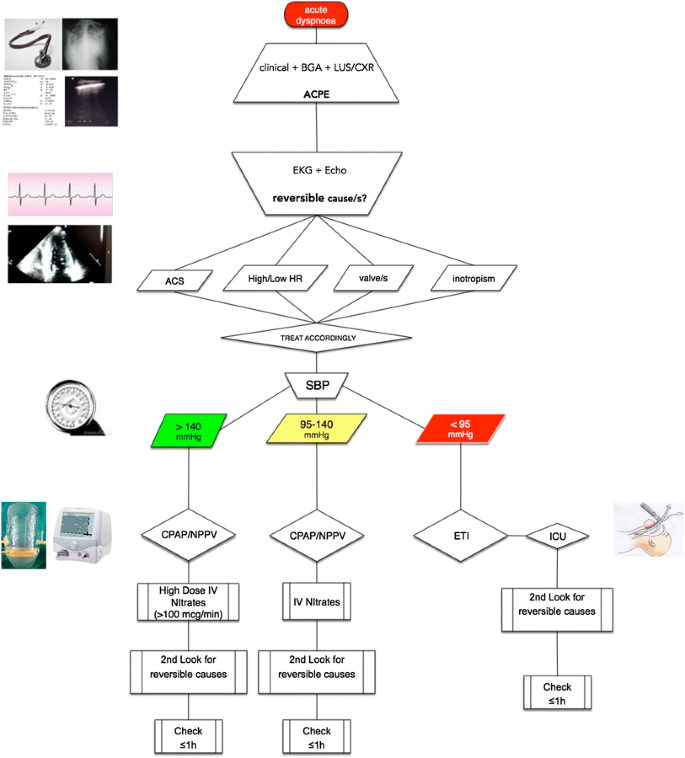
NIV flowchart for ACPE treatment
-
4.
Decide the type of flow generator The most important factor in delivering a positive pressure non-invasively is the administration of adequate inspiratory flow. ACPE patients are in respiratory distress, and therefore, need a high gas flow. The choice of the correct flow generator is, therefore, paramount.
-
(a)
In case you decide to start NIV you need a mechanical ventilator.
-
(b)
In case you decide to start CPAP there are different options:
-
(i)
Venturi flow generators They are stand-alone, easy to use, do not require advance technical knowledge and assure high flows even at elevated FiO2.
-
(ii)
Boussignac valve It is the simplest, but also a lesser performance device. It only requires a source of oxygen, even a tank, but positive pressure is inconstant and at best 7–8 cmH2O.
-
(iii)
Specially conceived devices integrating a low performance Venturi flow generator on the CPAP interface, such as the Ventukit (Intersurgical). These devices are easy to use, do not require any special equipment and allow the application of high inspiratory flows at a moderate FiO2 (max 50% on average).
-
(iv)
Mechanical ventilator Mechanical ventilators are effective in administering a high inspiratory flow, but their use requires technical knowledge and the right settings need to be selected.
Our advice is to use either a Venturi flow generator (first choice) or a mechanical ventilator (second choice) if available. If you are in the prehospital setting or assisting a patient in a non-equipped environment, use either a Boussignac CPAP (first choice) or an integrated Venturi CPAP interface (such as the Ventukit, Intersurgical—second choice) for initial treatment and stabilization.
-
(i)
-
(a)
-
5.
Choose the interface Interface choice is the key to NIV/CPAP success. The type of interface (nasal mask vs oronasal mask vs full-face mask vs helmet) depends on patient characteristics, whether you want to deliver CPAP or NIV and the flow generator you decide to use. The wrong interface, or the wrong size, may determine rapid NIV failure independent of other variables.
Nasal masks should be avoided in acute respiratory failure. Oronasal or full face masks are our first choices in case of NIV, taking care to choose the right type and size adapted to the patient’s facial characteristics (to minimize leaks) and patient’s optimal comfort. The helmet is our first choice in case of CPAP because of superior comfort and better tolerance on long term; we discourage helmet use in NIV mode due to extremely difficult patient ventilator-synchrony, and it should be reserved to expert users and probably intensive care units. Furthermore, helmet NIV should only be performed with a flow generator able to provide high flows due to the risk of CO2 rebreathing [5].
Take your time to study the patient’s characteristics, and do not hesitate to try different types of masks and different sizes. The interface should be adapted to the patient’s need and not the opposite!
-
6.
Before applying the interface, talk to your patient and explain what you are going to do. Do not force NIV/CPAP against a patient’s will.
-
7.
Initial settings No study specifically addresses the question of initial NIV/CPAP settings in ACPE. Therefore, we make recommendations based on our experience and current practice. We suggest starting with 10 cmH2O of PEEP if you use Venturi flow-generator, and lower moderate pressures to avoid leaks in case of NIV, and increase pressure if clinically needed. Suggested initial settings are shown in Table 1.
Table 1 Initial suggested settings and recommended monitoring during NIV/CPAP -
8.
Alarm settings Some Venturi flow generators allow for pressure and FiO2 alarms to be set. On every mechanical ventilator alarms must be set after confirming ventilatory settings.
-
9.
Monitoring (see Table 1) Monitoring the patient undergoing NIV/CPAP should be multimodal, no single parameter can predict NIV/CPAP success or failure. Therefore, we recommend the following assessment strategy:
-
(a)
Stay with the patient at least for the first 5–10 min, and monitor patient comfort, interface tolerance and the presence of air leaks. If air leaks are present, tighten the interface or change interface type or size. If the patient is agitated talk to him or her, and try to reassure him or her.
In case of NIV, monitoring expiratory tidal volume easily allows for the detection of air leaks.
-
(b)
After 30 min of NIV/CPAP, SpO2 should be improving, respiratory rate should be decreasing as well as signs of respiratory distress. Consciousness should be assessed and neurological deterioration detected immediately. Hemodynamic response to NIV/CPAP should be assessed by non-invasive blood pressure and heart rate. Reassess lung congestion by ultrasound [4].
-
(c)
After 60 min, perform the first blood gases: oxygenation should be assessed in terms of PaO2/FiO2 ratio, an improvement should be already present. pH and PaCO2 might not yet show clear signs of improvement, but should not be worsening; if respiratory acidosis is worsening consider increasing PS (= increase IPAP) or PEEP (= increase EPAP).
-
(d)
At 180 min perform a full clinical assessment, new blood gases and obtain hemodynamic parameters. At this stage, a clinical improvement in the respiratory pattern and respiratory rate should be evident. Blood gases should show improvement in PaO2/FiO2, pH and PaCO2.
-
(a)
-
10.
Weaning NIV/CPAP may induce a rapid and dramatic improvement in clinical and blood gas variables in ACPE patients, especially in those patients who also rapidly respond to medical treatment (either vasodilators or diuretics or both). Clinicians should, however. refrain from the temptation of stopping NIV/CPAP abruptly after clinical improvement. In ACPE a rapid but systematic weaning must be performed, our suggestion is to lower PEEP to 5 cmH2O if on CPAP mode or to lower PEEP to 4 cmH20 (= EPAP 4 cmH2O) and PS to 4 cm H2O (= IPAP 8 cmH2O) in NIPPV mode, and to maintain these settings for 30–60 min. No blood gases are needed, but if clinical parameters and SpO2 remain stable, NIV can be safely stopped and conventional O2 therapy started; conversely, if clinical parameters and SpO2 deteriorate, settings must be switched back to original values and NIV/CPAP continued.

References
Margutti E, Greco I, Brambilla AM, Maraffi T, Cosentini R (2017) Non-invasive ventilation in acute respiratory failure: the key “W” questions. Intern Emerg Med. doi:10.1007/s11739-017-1721-x
Vital FM, Ladeira MT, Atallah AN (2013) Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev. doi:10.1002/14651858.CD005351.pub3
Lenique F, Habis M, Lofaso F, Dubois-Rande JL, Harf A, Brochard L (1997) Ventilatory and hemodynamic effects of continuous positive airway pressure in left heart failure. Am J Respir Crit Care Med 155:500–505
Leidi F, Casella F, Cogliati C (2016) Bedside lung ultrasound in the evaluation of acute decompensated heart failure. Intern Emerg Med 11(4):597–601
Taccone P, Hess D, Caironi P (2004) Continuous positive airway pressure delivered with a “helmet”: effects on carbon dioxide rebreathing. Crit Care Med 32(10):2090–2096
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
This article does not involve any human beings or animals.
Informed consent
None.
Rights and permissions
About this article

Cite this article
Maraffi, T., Brambilla, A.M. & Cosentini, R. Non-invasive ventilation in acute cardiogenic pulmonary edema: how to do it. Intern Emerg Med 13, 107–111 (2018). https://doi.org/10.1007/s11739-017-1751-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-017-1751-4