
Abstract
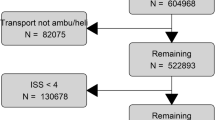
Emergency department (ED) overcrowding remains a significant problem in many hospitals, and results in multiple negative effects on patient care outcomes and operational metrics. We sought to test whether implementing a quality improvement project could decrease ED LOS for trauma patients requiring an ICU admission from the ED, specifically by directly admitting critically ill trauma patients from the ED CT scanner to an ICU bed. This was a retrospective study comparing patients during the intervention period (2013–2014) to historical controls (2011–2013). Critically ill trauma patients requiring a CT scan, but not the operating room (OR) or Interventional Radiology (IR), were directly admitted from the CT scanner to the ICU, termed the “One-way street (OWS)”. Controls from the 2011–2013 Trauma Registry were matched 1:1 based on the following criteria: Injury Severity Score; mechanism of injury; and age. Only patients who required emergent trauma consult were included. Our primary outcome was ED LOS, defined in minutes. Our secondary outcomes were ICU LOS, hospital LOS and mortality. Paired t test or Wilcoxon signed rank test were used for continuous univariate analysis and Chi square for categorical variables. Logistic regression and linear regressions were used for categorical and continuous multivariable analysis, respectively. 110 patients were enrolled in this study, with 55 in the OWS group and 55 matched controls. Matched controls had lower APACHE II score (12 vs. 15, p = 0.03) and a higher GCS (14 vs. 6, p = 0.04). ED LOS was 229 min shorter in the OWS group (82 vs. 311 min, p < 0.0001). The time between CT performed and ICU disposition decreased by 230 min in the OWS arm (30 vs. 300 min, p < 0.001). There was no difference in ED arrival to CT time between groups. Following multivariable analysis, mortality was primarily predicted by the APACHE II score (OR 1.29, p < 0.001), and not ISS, mechanism of injury, or age. After controlling for APACHE II score, there was no difference in mortality between the two cohorts (OR = 0.49, p = 0.28). Expedited admission of critically ill trauma patients immediately following CT imaging significantly reduced ED LOS by 3.82 h (229 min), without a change in ICU LOS, hospital LOS, or mortality. Further studies are needed to assess the impact of expedited admission on morbidity and mortality.


Similar content being viewed by others

References
Dickinson G (1989) Emergency department overcrowding. CMAJ 140:270–271
Richardson DB (2006) Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 184:213–216
Pines JM, Hollander JE, Localio AR, Metlay JP (2006) The association between emergency department crowding and hospital performance on antibiotic timing for pneumonia and percutaneous intervention for myocardial infarction. Acad Emerg Med 13:873–878
Pines JM, Localio AR, Hollander JE et al (2007) The impact of emergency department crowding measures on time to antibiotics for patients with community-acquired pneumonia. Ann Emerg Med 50:510–516
Fee C, Weber EJ, Maak CA, Bacchetti P (2007) Effect of emergency department crowding on time to antibiotics in patients admitted with community-acquired pneumonia. Ann Emerg Med 50:501–509 (509.e1)
Nguyen HB, Rivers EP, Havstad S et al (2000) Critical care in the emergency department: a physiologic assessment and outcome evaluation. Acad Emerg Med 7:1354–1361
Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP, group D-Es (2007) Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med 35:1477–1483
Hung SC, Kung CT, Hung CW et al (2014) Determining delayed admission to intensive care unit for mechanically ventilated patients in the emergency department. Crit Care 18:485
Sampalis JS, Denis R, Frechette P, Brown R, Fleiszer D, Mulder D (1997) Direct transport to tertiary trauma centers versus transfer from lower level facilities: impact on mortality and morbidity among patients with major trauma. J Trauma 43:288–295 (discussion 95-6)
Baker SP, O’Neill B, Haddon W Jr, Long WB (1974) The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 14:187–196
Copes WS, Champion HR, Sacco WJ et al (1990) Progress in characterizing anatomic injury. J Trauma 30:1200–1207
Ladha KS, Zhao K, Quraishi SA et al (2015) The Deyo-Charlson and Elixhauser-van Walraven comorbidity indices as predictors of mortality in critically ill patients. BMJ Open 5:e008990
Richardson JD, Franklin G, Santos A et al (2009) Effective triage can ameliorate the deleterious effects of delayed transfer of trauma patients from the emergency department to the ICU. J Am Coll Surg 208:671–678 (discussion 8-81)
Singer AJ, Thode HC Jr, Viccellio P, Pines JM (2011) The association between length of emergency department boarding and mortality. Acad Emerg Med 18:1324–1329
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Fuentes, E., Shields, JF., Chirumamilla, N. et al. “One-way-street” streamlined admission of critically ill trauma patients reduces emergency department length of stay. Intern Emerg Med 12, 1019–1024 (2017). https://doi.org/10.1007/s11739-016-1511-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-016-1511-x