
Abstract
Introduction
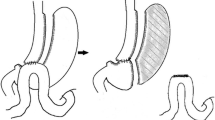
A subset of patients undergoing laparoscopic sleeve gastrectomy (SG) require eventual conversion to Roux-en-Y gastric bypass (RYGB) due to complications from SG or to enhance weight loss. The aim of this study is to characterize the indications for conversion and perioperative outcomes in a large cohort of these patients at a single institution.
Methods
Patients who underwent revisional surgery to convert SG to RYGB at our institution from January 2008 through January 2017 were retrospectively reviewed.
Results
Eighty-nine patients with previous SG underwent conversion to RYGB as part of a planned two-stage approach to gastric bypass (n = 36), for weight recidivism (n = 11), or for complications related to SG (n = 42). Complications from SG that warranted conversion included refractory GERD (40.5%), sleeve stenosis (31.0%), gastrocutaneous (16.7%), or gastropleural (7.1%) fistula, and gastric torsion (4.1%). The mean (SD) age was 47.2 years (11.4 years) and median BMI at the time of revision was 43.2 kg/m2. A laparoscopic approach was successfully completed in 76 patients (85.4%), with an additional of four completed robotically (4.5%). The median length of stay was 3 days. Twenty-eight patients (31.5%) had complications which included surgical site infection (20.2%), re-operation (6.7%), anastomotic stricture (3.4%), and one pulmonary embolism. There were no mortalities with a median follow-up of 15 months.
Conclusions
Conversion of SG to RYGB is safe and technically feasible when performed for complications of SG or to enhance weight loss. This operation can be successfully performed laparoscopically with a low rate of conversion and reasonable complication profile.

Similar content being viewed by others

References
Hess DS, Hess DW. Biliopancreatic diversion with a duodenal switch. ObesSurg. 1998;8:267–82.
Marceau P, Hould FS, Simard S, et al. Biliopancreatic diversion with duodenal switch. World J Surg. 1998;22:947–54.
Trelles N, Gagner M. Sleeve gastrectomy. Oper Tech Gen Surg. 2007;9:123–31.
Rosenthal RJ, International Sleeve Gastrectomy Expert Panel, Diaz AA, et al. International Sleeve Gastrectomy Expert Panel Consensus Statement: best practice guidelines based on experience of >12,000 cases. Surg Obes Relat Dis. 2012;8:8–19.
Deitel M, Crosby RD, Gagner M. The First International Consensus Summit for Sleeve Gastrectomy (SG), New York City, October 25-27, 2007. ObesSurg. 2008;18:487–96.
Gagner M, Deitel M, Kalberer TL, et al. The Second International Consensus Summit for Sleeve Gastrectomy, March 19-21, 2009. SurgObesRelatDis. 2009;5:476–85.
Deitel M, Gagner M, Erickson AL, et al. Third International Summit: current status of sleeve gastrectomy. SurgObesRelatDis. 2011;7:749–59.
Gagner M, Deitel M, Erickson AL, et al. Survey on laparoscopic sleeve gastrectomy (LSG) at the Fourth International Consensus Summit on Sleeve Gastrectomy. ObesSurg. 2013;23:2013–7.
Gagner M, Hutchinson C, Rosenthal R. Fifth International Consensus Conference: current status of sleeve gastrectomy. SurgObesRelatDis. 2016;12:750–6.
Clinical Issues Committee of American Society for Metabolic and Bariatric Surgery. Sleeve gastrectomy as a bariatric procedure. SurgObesRelatDis. 2007;3:573–6.
ASMBS Clinical Issues Committee. Updated position statement on sleeve gastrectomy as a bariatric procedure. Surg Obes Relat Dis. 2012;8:e21–6.
Ferrer-Marquez M, Belda-Lozano R, Solvas-Salmeron MJ, et al. Revisional surgery after laparoscopic sleeve gastrectomy. Surg Laparosc Endosc Percutan Tech. 2015;25:6–9.
Brethauer SA, Kothari S, Sudan R, et al. Systematic review on reoperative bariatric surgery: American Society for Metabolic and Bariatric Surgery Revision Task Force. Surg Obes Relat Dis. 2014;10:952–72.
Homan J, Betzel B, Aarts EO, et al. Secondary surgery after sleeve gastrectomy: Roux-en-Y gastric bypass or biliopancreatic diversion with duodenal switch. Surg Obes Relat Dis. 2015;11:771–7.
Sanchez-Pernaute A, Rubio MA, Cabrerizo L, et al. Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11:1092–8.
Noel P, Nedelcu M, Nocca D, et al. Revised sleeve gastrectomy: another option for weight loss failure after sleeve gastrectomy. Surg Endosc. 2014;28:1096–102.
Bruzzi M, Voron T, Zinzindohoue F, et al. Revisional single-anastomosis gastric bypass for a failed restrictive procedure: 5-year results. Surg Obes Relat Dis. 2016;12:240–5.
User Guide for the 2015 ACS NSQIP Procedure Targeted Participant Use Data File (PUF). American College of Surgeons National Surgical Quality Improvement Program. 2016.
Mangram AJ, Horan TC, Pearson ML, et al. Guideline for prevention of surgical site infection, 1999. Hospital infection control practices advisory committee. Infect Control Hosp Epidemiol. 1999;20:250–78. quiz 279–80
Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81.
Brethauer SA, Kim J, el Chaar M, et al. Standardized outcomes reporting in metabolic and bariatric surgery. Surg Obes Relat Dis. 2015;11:489–506.
Silecchia G, Boru C, Pecchia A, et al. Effectiveness of laparoscopic sleeve gastrectomy (first stage of biliopancreatic diversion with duodenal switch) on co-morbidities in super-obese high-risk patients. Obes Surg. 2006;16:1138–44.
Frezza EE. Laparoscopic vertical sleeve gastrectomy for morbid obesity. The future procedure of choice? Surg Today. 2007;37:275–81.
Boza C, Salinas J, Salgado N, et al. Laparoscopic sleeve gastrectomy as a stand-alone procedure for morbid obesity: report of 1,000 cases and 3-year follow-up. Obes Surg. 2012;22:866–71.
Estimate of Bariatric Surgery Numbers, 2011–2015 [Internet]. Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers.
van Rutte PW, Smulders JF, de Zoete JP, et al. Indications and short-term outcomes of revisional surgery after failed or complicated sleeve gastrectomy. Obes Surg. 2012;22:1903–8.
Arman GA, Himpens J, Dhaenens J, et al. Long-term (11+years) outcomes in weight, patient satisfaction, comorbidities, and gastroesophageal reflux treatment after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2016;12:1778–86.
Shabino PJ, Khoraki J, Elegbede AF, et al. Reduction of surgical site infections after laparoscopic gastric bypass with circular stapled gastrojejunostomy. Surg Obes Relat Dis. 2016;12:4–9.
Yorke E, Sheppard C, Switzer NJ, et al. Revision of sleeve gastrectomy to Roux-en-Y gastric bypass: a Canadian experience. Am J Surg. 2017;213:970–4.
Quezada N, Hernandez J, Perez G, et al. Laparoscopic sleeve gastrectomy conversion to Roux-en-Y gastric bypass: experience in 50 patients after 1 to 3 years of follow-up. Surg Obes Relat Dis. 2016;12:1611–5.
Carmeli I, Golomb I, Sadot E, et al. Laparoscopic conversion of sleeve gastrectomy to a biliopancreatic diversion with duodenal switch or a Roux-en-Y gastric bypass due to weight loss failure: our algorithm. Surg Obes Relat Dis. 2015;11:79–85.
Prachand VN, Ward M, Alverdy JC. Duodenal switch provides superior resolution of metabolic comorbidities independent of weight loss in the super-obese (BMI > or = 50 kg/m2) compared with gastric bypass. J Gastrointest Surg. 2010;14:211–20.
Dapri G, Cadiere GB, Himpens J. Laparoscopic repeat sleeve gastrectomy versus duodenal switch after isolated sleeve gastrectomy for obesity. Surg Obes Relat Dis. 2011;7:38–43.
Rebibo L, Fuks D, Verhaeghe P, et al. Repeat sleeve gastrectomy compared with primary sleeve gastrectomy: a single-center, matched case study. Obes Surg. 2012;22:1909–15.
Cohen R, Pinheiro JS, Correa JL, et al. Laparoscopic revisional bariatric surgery: myths and facts. Surg Endosc. 2005;19:822–5.
Moon R, Teixeira A, Potenza K, et al. Routine gastrostomy tube placement in gastric bypass patients: impact on length of stay and 30-day readmission rate. Obes Surg. 2013;23:216–21.
Acknowledgements
No individuals other than the stated authors contributed to this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
John H. Rodriguez has no conflict of interest relevant to this publication and has received research funding from Pacira Pharmaceuticals and Intuitive Surgical. Stacy Brethauer has no conflict of interest relevant to this publication, is a consultant for Ethicon, and has been a speaker for Ethicon and Covidien. Philip R. Schauer has no conflict of interest relevant to this publication; has been a speaker for Ethicon; has received research funding from Ethicon, Medtronic, and Pacira Pharmaceuticals; and is on the advisory boards of AMAG Pharmaceuticals, GI Dynamics, Pacira Pharmaceuticals, and Neurotronic. Matthew D. Kroh has no conflict of interest relevant to this publication, is a consultant for Levita Magnetics, and has received research funding from Cook Biotech, Medtronic, and Pacira Pharmaceuticals. Joshua P. Landreneau, Andrew T. Strong, Essa M. Aleassa, and Ali Aminian have no conflict of interest or financial ties to disclose.
Statement Regarding Ethics and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent was not required.
Rights and permissions
About this article

Cite this article
Landreneau, J.P., Strong, A.T., Rodriguez, J.H. et al. Conversion of Sleeve Gastrectomy to Roux-en-Y Gastric Bypass. OBES SURG 28, 3843–3850 (2018). https://doi.org/10.1007/s11695-018-3435-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3435-1