
Abstract
Background
Medicaid expansion in Michigan, known as the Healthy Michigan Plan (HMP), emphasizes primary care and preventive services.
Objective
Evaluate the impact of enrollment in HMP on access to and receipt of care, particularly primary care and preventive services.
Design
Telephone survey conducted during January–November 2016 with stratified random sampling by income and geographic region (response rate = 53.7%). Logistic regression analyses accounted for sampling and nonresponse adjustment.
Participants
4090 HMP enrollees aged 19–64 with ≥ 12 months of HMP coverage
Main Measures
Surveys assessed demographic factors, health, access to and use of health care before and after HMP enrollment, health behaviors, receipt of counseling for health risks, and knowledge of preventive services’ copayments. Utilization of preventive services was assessed using Medicaid claims.
Key Results
In the 12 months prior to HMP enrollment, 33.0% of enrollees reported not getting health care they needed. Three quarters (73.8%) of enrollees reported having a regular source of care (RSOC) before enrollment; 65.1% of those reported a doctor’s office/clinic, while 16.2% reported the emergency room. After HMP enrollment, 92.2% of enrollees reported having a RSOC; 91.7% had a doctor’s office/clinic and 1.7% the emergency room. One fifth (20.6%) of enrollees reported that, before HMP enrollment, it had been over 5 years since their last primary care visit. Enrollees who reported a visit with their primary care provider after HMP enrollment (79.3%) were significantly more likely than those who did not report a visit to receive counseling about health behaviors, improved access to cancer screening, new diagnoses of chronic conditions, and nearly all preventive services. Enrollee knowledge that some services have no copayments was also associated with greater utilization of most preventive services.
Conclusions
After enrolling in Michigan’s Medicaid expansion program, beneficiaries reported less forgone care and improved access to primary care and preventive services.
Similar content being viewed by others


INTRODUCTION
Michigan received a Section 1115 waiver from the Centers for Medicare & Medicaid Services allowing the implementation of an alternative approach to Medicaid expansion under the Affordable Care Act.1, 2 Michigan’s approach, the Healthy Michigan Plan (HMP), opened enrollment for beneficiaries up to 133% of the Federal Poverty Level (FPL) in April 2014. Most participants must enroll in a Medicaid managed care plan, either of their own choosing or by assignment if they do not select one. All plan enrollees choose or are assigned a primary care provider (PCP).
HMP emphasizes primary care and prevention, encouraging each enrollee to schedule an appointment with their PCP within 60–90 days of enrollment, though there is no penalty for failing to do so. During a PCP visit, enrollees are asked to complete a Health Risk Assessment (HRA) which includes questions about their health behaviors (e.g., exercise, smoking) and, until late 2017, included measures of health risk (e.g., blood pressure). The HRA encourages enrollees, in consultation with their PCP, to commit to adopting or maintaining healthy behaviors. Enrollees could receive financial incentives such as gift cards or discounted premiums and copayments1 if they complete the HRA and their PCP submits it to their health plan.
Other features of HMP include copayments for most enrollees, waived for preventive services or care related to many chronic conditions. Those with incomes over 100% FPL owe premium-like monthly contributions, up to 2% of household income; total annual contributions and copayments cannot exceed 5% of household income (https://www.michigan.gov/documents/mdch/Healthy_Michigan_Copayment-final_452237_7.pdf). MI Health Account statements, sent quarterly to enrollees, list health care services received; costs to the health plan and the enrollee, including copayments and contributions; and payments owed and remitted. Statements also refer enrollees to their health plan to learn how to earn healthy behavior rewards.
This study is derived from a federally authorized evaluation of HMP examining the impact of the program on enrollees from a variety of perspectives. Through a survey of over 4000 HMP enrollees, we evaluated the impact of enrollment on access to and receipt of care, particularly primary care and preventive services, whether changes were more likely for those who were uninsured prior to enrollment, and what effect incentives to reduce enrollees’ cost-sharing might have on their receipt of preventive services.
METHODS
Survey Sampling and Administration
The Healthy Michigan Voices telephone survey, conducted from January to November 2016, included 4090 non-elderly enrollees in the Healthy Michigan Plan (HMP). The sample, described previously,3,4,5 was drawn using a design that stratified HMP enrollees based on four geographic regions in the state and three FPL categories (0–35%; 36–99%; ≥ 100%) to ensure statistical power for subgroup analysis. Enrollees eligible for the survey were aged 19–64 years, enrolled in HMP ≥ 12 months, with a preferred language of English, Spanish, or Arabic and a complete Michigan address and phone number in Medicaid program files. The weighted response rate for the 2016 Healthy Michigan Voices enrollee survey was 53.7%. The median interview length was 22 min (range 12–96). Respondents received a $25 gift card. Survey weights reflecting the stratified sample design were developed,6 adjusted for potential nonresponse bias through a logistic regression model7, 8 and calibrated to the known population totals through ratio-raking.9, 10
Survey Measures
The survey included measures of demographic characteristics, health status, access to care, insurance status prior to HMP enrollment, and experiences of primary and preventive care. Many measures were drawn from national surveys.11,12,13,14,15,16,17,18,19 New items and scales (e.g., understanding of HMP features) were developed from 67 semi-structured interviews with enrollees. New items underwent cognitive testing and pre-testing for timing and flow before being included in the survey instrument.Footnote 1
Utilization Measures
Vaccination data were drawn from the Michigan Care Improvement Registry and included receipt of flu vaccine for the 2015–2016 season and receipt of other vaccines at any time during 2015 and 2016. Receipt of other preventive services was drawn from Medicaid administrative claims for the period from each respondent’s initial HMP enrollment to the time of survey completion, including:
Breast cancer screening (restricted to women ≥ 50 years).
Cervical cancer screening (Pap smear only; restricted to women).
Colorectal cancer screening (enrollees ≥ 50 years).
Diabetes Prevention Program—not a Michigan Medicaid-covered benefit, although health plans may cover.
Any nutrition service—not a Michigan Medicaid-covered benefit absent specific diagnoses; health plans may cover.
Dental visit—although not all visits are solely preventive, having ≥ 1 dental visit was counted as providing an oral wellness service.
Testing for sexually transmitted infections (excluding HPV).
Prescription for HMG CoA reductase inhibitor, varenicline (tobacco users), and nicotine replacement (tobacco users).
Primary care visits.
Analysis
Descriptive statistics were generated for all survey and utilization measures. Pearson’s chi-square analyses were performed to describe bivariate relationships. Multivariate analyses examined relationships between pre-enrollment insurance status (insured all 12 months, some of the 12 months, or none of the 12 months prior to enrollment) and dependent variables of access, health and worry, adjusting for age, gender, FPL, race and ethnicity (Hispanic, Arabic/Chaldean), urbanicity, self-reported health status, and self-reported chronic condition(s). Bivariate relationships between receipt of preventive services and knowledge about waived copayments for preventive services and health behavior rewards used Pearson’s chi-square tests, multivariate analyses of the relationship between self-reported primary care visit and receipt of preventive services controlled for age, gender, race, ethnicity, urbanicity, self-reported health status, and self-reported chronic condition(s). We used self-reported primary care visits for analyses examining the relationship between PCP visits and other variables. Analyses using claims data for primary care visits found similar relationships, When applicable, analyses only included relevant subgroups (e.g., colon cancer screening for enrollees ≥ 50, tobacco counseling by tobacco users).
All statistical analyses were conducted using Stata v.14.2 and accounted for weights based on sample design features.
This study based on data collected for a federally authorized evaluation of a public program was deemed exempt from review by the University of Michigan and MDHHS Institutional Review Boards.
RESULTS
Demographic Characteristics of Respondents
After weighting, demographic characteristics of respondents closely matched characteristics of the broader HMP enrollee population (Table 1; Appendix Table 5). Just over half (51.6%) were women, 51.8% had incomes 0–35% FPL, 26.0% were over 51 years old, and 10.2% lived in rural areas. More than two thirds (69.2%) reported having a chronic condition, and three in ten (29.7%) reported fair/poor health status. Almost half (48.8%) of enrollees reported they were employed or self-employed, 27.6% were out of work, 11.3% were unable to work, and 2.5% were retired.
Insurance Before Enrollment
Over half (57.9%) of enrollees had no health insurance at any time in the 12 months prior to HMP enrollment. Enrollees with an income of 0–35% FPL were more likely than those in other income groups to have no health insurance in the 12 months prior to HMP enrollment (62.6% vs. 54.1% for enrollees 36–99% FPL and 50.9% for enrollees ≥ 100% FPL, p < 0.001). Most enrollees who reported having health insurance at some point during the 12 months prior to HMP enrollment were insured all 12 months (73.8%). About half (50.8%) of enrollees who reported having health insurance at any time in the 12 months prior to enrollment had Medicaid or coverage through another state program, while a quarter (26.2%) had private insurance through a job or union and 10.2% had individually purchased insurance.
Forgone Care Before Enrollment
One third (33.0%) of enrollees reported not getting the health care they needed in the 12 months prior to HMP enrollment. Forgone care was most often dental care (63.2%), with specialty care (21.7%) and prescriptions (19.9%) the next most common types. The most common reasons for not getting care prior to HMP were being worried about the cost (77.5%) and not having health insurance (67.4%). Those who were insured all 12 months prior to HMP enrollment were significantly less likely than those who were uninsured all 12 months to report forgone care or forgone care due to cost prior to HMP enrollment (Table 2).
Forgone Care, Health, and Stress After Enrollment
In the 12 months preceding the survey, 15.6% reported not getting the medical or dental care they needed. Among this group, the most common reasons for not getting this care were that their health plan would not pay for the treatment (39.6%), being worried about cost (25.4%), and that a doctor or hospital would not accept insurance (23.9%). When asked about changes in access to care, many reported greater ability to get prescription medications (59.3%), dental care (46.1%), specialist care (44.4%), and mental health care (27.5%) (Table 2). Many also reported improved physical health (47.8%), mental health (38.2%), and oral health (39.5%). Most enrollees reported less stress (87.9% strongly agreed/agreed) and less worry about something bad happening to their health since enrolling in HMP (69.0% strongly agreed/agreed). Those who were insured all 12 months prior to HMP enrollment were significantly less likely than those who were uninsured all 12 months to report improvements in access, health, stress, or worry. (Table 2).
Regular Source of Care Before and After Enrollment
About three quarters (73.8%) of enrollees reported having a regular source of care (RSOC) in the 12 months prior to HMP enrollment (Fig. 1). Among enrollees who reported having a RSOC before enrollment, they most often named a doctor’s office (47.9%) or clinic (17.2%). Substantial portions reported the emergency room (16.2%) and urgent care (16.8%) (Fig. 1). Those with incomes > 100% FPL were more likely to report having a RSOC in the 12 months prior to HMP enrollment than those with lower incomes (77.3% for > 100% FPL, 74.1% for 36–99% FPL, 72.2% for 0–35% FPL, p = 0.035). After HMP enrollment, almost all (92.2%) enrollees indicated having a regular source of care; there were no significant differences by income category. Those reporting a RSOC most often named a doctor’s office (75.2%) or clinic (16.5%). Few reported the emergency room (1.7%) and urgent care (5.8%) (Fig. 2).]-->

Regular source of care before and after enrollment in HMP.
]-->

Receipt of preventive care while enrolled in Healthy Michigan Plan. Weighted proportions of services based on claims analysis. See Table 6, Appendix. HPV human papilloma virus, STI sexually transmitted infection. *Analysis restricted to women 50 and older. **Analysis restricted to women; excludes HPV. ***Analysis restricted to women and men 50 and older. ^Any preventive service with the exception of primary care visit. Diabetes Prevention Program and other nutrition services are not necessarily covered by a Medicaid health plan.
Primary Care Before and After Enrollment
One fifth (20.6%) of enrollees reported that, before enrolling in HMP, it had been over 5 years since their last primary care visit, with 37.8% reporting a primary care visit 1–5 years and 40.1% within 12 months prior to enrollment. Those with an income of 0–35% FPL were more likely to report they had not seen a PCP for more than 5 years prior to HMP enrollment (23.7% for 0–35% FPL, 18.1% for 36–99% FPL, 15.9% for > 100% FPL, p < 0.004).
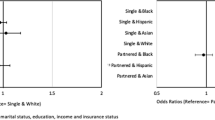
The majority (85.2%) of enrollees who indicated having a PCP through HMP reported having a primary care visit within the preceding 12 months; 89.5% of all enrollees had a claim for a primary care visit. For enrollees who reported not seeing their PCP in the past 12 months, the most common reason was that they were healthy and did not need to see a provider (63.4%). Older enrollees, women, white enrollees, those in worse health or with a chronic condition, and those residing in rural areas were more likely to report a primary care visit. Self-reported primary care visits after enrollment did not differ on the basis of income, ethnicity, employment, partnership status, or health literacy (Tables 7 and 8, Appendix).
Relationship Between Primary Care and Access, Health Behavior Counseling, and Preventive Services
Of enrollees who reported a primary care visit, 91.1% said they discussed health promotion and disease prevention. They were almost twice as likely to report receiving help with staying healthy (aOR = 1.82, p < 0.001) and improved access to cancer screening (aOR = 1.82, p < 0.001) and more likely to report improved access to dental care (aOR = 1.31, p = 0.016) and specialty care (aOR = 1.64, p < 0.001). They were much more likely to report being counseled about exercise (aOR = 4.52, p < 0.001), nutrition (aOR = 4.01, p < 0.001), tobacco cessation (aOR = 4.64, p < 0.001), or alcohol use (aOR = 3.27, p < 0.001). They were also more likely to report having a new diagnosis of a chronic condition after HMP enrollment (aOR = 1.77, p < 0.001). The vast majority of enrollees received at least one preventive service (Fig. 2). Those who reported having a PCP visit were significantly more likely than those who did not to have claims for most preventive services (Table 3).
Knowledge About Costs and Healthy Behavior Rewards, Relation to Preventive Services
Three quarters of enrollees (75.6%) were aware that some kinds of visits, tests, and medicines have no copayments while one quarter (28.1%) were aware that they could get a reduction in the amount they have to pay by completing an HRA. Enrollee knowledge that some services have no copayments was significantly associated with greater utilization of nearly all preventive services examined (Table 4). Enrollee knowledge that completing an HRA could result in lower fees was not associated with any preventive service use.
DISCUSSION
This comprehensive study of Medicaid expansion in Michigan found less forgone care; improved access to primary care, health counseling, and other health services; high use of preventive services; and enrollee reports of improved overall physical, mental, and dental health and less stress and worry. These improvements were greater for those, a majority, who lacked insurance for all 12 months before enrollment in Healthy Michigan.
We found substantial increases in having a regular source of care after enrollment in HMP, similar to the Oregon Health Insurance Experiment.20 Other studies have not found statistically significant changes21, 22. About three quarters of HMP enrollees reported having a regular source of care before enrollment, while almost all (92.2%) reported a RSOC after enrollment. Reporting the emergency room as a RSOC decreased.
Our findings expand on other studies demonstrating that Medicaid expansion enhances primary care utilization.21,22,23,24, 32 A national study of low-income adults found Medicaid expansions were associated with increased visits to physicians in general practice by 6.6 percentage points.18 Another study comparing three states found that expansion was associated with a 12.1% increase in access to primary care.[24] Remarkably, one fifth of enrollees said they had not had a primary care visit in over 5 years, and only two fifths reported a primary care visit in the 12 months prior to enrolling in HMP; double that proportion reported a PCP visit in the 12 months before the survey. Clearly, the previously uninsured covered by Medicaid expansion had great unmet needs for primary care.
This study adds to a modest literature about the impact of Medicaid expansion on preventive services.20, 21, 31 We found high utilization of a broad range of preventive services. Survey data adds enrollee reports of prevention that can be harder to measure using administrative data, such as counseling for health behaviors. Many enrollees reported improved access to cancer screening and help with staying healthy, and being counseled about healthy behaviors.
Preventive service use and counseling were more likely for those reporting a primary care visit. For services that require a clinician’s order, such as colon cancer screening, the visit may be more of a mediator than an influence on receipt. However, some services, such as dental visits, influenza vaccinations, and breast and cervical cancer screening, may not require a referral. We found connections between primary care visits and nearly all preventive services, not just those requiring a physician’s order. Combined with connections between primary care and enrollees’ reports of improved access to prevention and health behavior counseling, results suggest that the emphasis on primary care and health risk assessment promotes prevention.
Enrollee knowledge that some services have no copayments was also associated with greater use of preventive services, while knowledge that completing an HRA could result in lower fees was not. It is not clear whether preventive service use itself improves knowledge that these services have no copay, or knowledge that they have no copay encourages use; further exploration would be helpful before drawing conclusions about causality. The lack of relationship between preventive services and knowledge of HRA incentives adds to evidence that those being incentivized must be aware of and understand the incentives in order for them to be effective.22,23,24,25, 26, 27, 29
A few studies have found Medicaid expansion increases the probability of diagnosis of specific chronic conditions.17, 18, 20, 26, 30 Medicaid expansion emphasizing primary care and prevention should lead to earlier diagnosis of chronic conditions; enrollees who reported a primary care visit were indeed more likely to report a new diagnosis.
Improvements in health since HMP enrollment were reported by a substantial number of enrollees. A few other studies, looking at differences between Medicaid expansion and non-expansion states, have found expansion associated with improved self-reported health status and lower rates of depression.16, 20, 27, 28
Limitations
Findings should be interpreted in the context of this work’s limitations. First, self-reported outcomes may be limited by recall bias and social desirability bias, an unavoidable limitation reporting what enrollees themselves say about their experiences of the impact of Medicaid expansion. Second, a cross-sectional study conducted after expansion limits inferences about causality. While this should temper conclusions about health improvements, reports about forgone care and a regular source of care are probably more robust. Third, the study was conducted relatively soon after expansion; results about enrollee knowledge of HMP (e.g., incentives) may change over time. Fourth, surveys are subject to response bias. Although our response rate was higher than most surveys of low-income populations, we nonetheless applied weights to lessen nonresponse bias. Fifth, claims may not be accurate proxies for some preventive services. Nutritional counseling, for example, may be provided without a claim. Some services (e.g., colorectal cancer screening) should occur at intervals longer than the time period we examined. Since we were not able to identify cancer screening received prior to enrollment, our results may underestimate the proportion who could be considered up to date. Finally, this study of Medicaid expansion was conducted in one state; generalization to other states and health systems outside the USA is limited.
Conclusions
Enrollees in Michigan’s Medicaid expansion, which has a strong emphasis on primary care and assessing health risks, report less forgone care, improved access to primary care, health promotion, and disease prevention. Our findings also show evidence of shifts in the regular source of care away from emergency rooms to doctor’s offices and clinics. Meeting unmet needs for primary care, with an emphasis on health promotion, disease prevention, and detection and management of chronic conditions, has potential for long-term improvements in health. Other states should consider ways to encourage the use of primary care to improve the health of low-income adults covered by Medicaid.
Notes
The survey instrument is available from the corresponding author.
References
https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/mi/Healthy-Michigan/mi-healthy-michigan-cms-amend-appvl-12302013.pdf. Accessed 12/28/18.
Ayanian JZ. Michigan’s approach to Medicaid expansion and reform. N Engl J Med. 2013;369:1773-5.
Moniz MH, Kirch MA, Solway E, Goold SD, Ayanian JZ, Kieffer EC, Clark SJ, Tipirneni R, Kullgren JT, Chang T. Association of Access to Family Planning Services with Medicaid Expansion Among Female Enrollees in Michigan. JAMA Netw Open. 2018;1(4):e181627.
Tipirneni R, Goold SD, Ayanian JZ. Employment Status and Health Characteristics of Adults with Expanded Medicaid Coverage in Michigan. JAMA Intern Med. 2017. https://doi.org/10.1001/jamainternmed.2017.7055.
Tipirneni R, Kullgren JT, Ayanian JZ, Kieffer EC, Rosland A, Chang T, Haggins AN, Clark SJ, Lee S, Solway E, Kirch MA, Mrukowicz C, Beathard E, Sears E, Goold SD. Changes in health and ability to work among Medicaid expansion enrollees: a mixed methods study. J Gen Intern Med. 2018;5.
Kish L. Weighting for unequal Pi. J Off Stat. 1992;8(2):183.
Kim JK, Kim JJ. Nonresponse weighting adjustment using estimated response probability. Can J Stat. 2007;35(4):501-514.
Lee S, Valliant R. Weighting telephone samples using propensity scores. Adv Telephone Surv Methodol. 2007;170-183.
Deville JC, Särndal CE, Sautory O. Generalized raking procedures in survey sampling. J Am Stat Assoc. 1993;88(423):1013-1020.
Kalton G, Flores-Cervantes I. Weighting methods. J Off Stat. 2003;19(2):81.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Questionnaire (or Examination Protocol, or Laboratory Protocol). Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2012. https://www.cdc.gov/nchs/nhanes/.
Center for Studying Health System Change. Health Tracking Household Survey, 2010 [United States]. Ann Arbor, MI: Inter-university Consortium for Political and Social Research [distributor], 2012-08-09. https://doi.org/10.3886/ICPSR34141.v1.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health Interview Survey Questionnaire. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/nhis/index.htm.
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Questionnaire. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
Ware JE, Kosinski M, Keller SD. A 12-item Short Form Health Survey: construction of scales and preliminary test of reliability and validity. Med Care. 1996;34:220–33.
Centers for Medicare & Medicaid Services. Consumer Assessment of Healthcare Providers and Systems (CAHPS). Rockville, MD: Agency for Healthcare Research and Quality. https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/CAHPS/. Modified March 15, 2018. Accessed July 2, 2018.
Fronstin P, Elmlinger A. Findings from the 2015 EBRI/Greenwald & Associates Consumer Engagement in Health Care Survey. EBRI Issue Brief. 2015;(421):1-25.
Center for Studying Health System Change. Health Tracking Household Survey, 2007 [United States] (ICPSR 26001). https://www.icpsr.umich.edu/icpsrweb/HMCA/studies/26001/version/1. Published April 15, 2011. Accessed July 2, 2018.
S Census Bureau. American Community Survey (ACS). https://www.census.gov/programs-surveys/acs/. Accessed July 2, 2018.
Baicker K, Taubman SL, Allen HL, et al. The Oregon Experiment—effects of Medicaid on clinical outcomes. N Engl J Med. 2013;368:1713-1722.
Sommers B, Blendon R, Orav EJ. Both the ‘private option’ and traditional Medicaid expansions improved access to care for low-income adults. Health Aff. 2016;35:96-105.
Miller S, Wherry LR. Health and access to care during the first 2 years of the ACA Medicaid expansions. N Engl J Med. 2017;376:947-956.
Wherry LR, Miller S. Early coverage, access, utilization, and health effects associated with the Affordable Care Act Medicaid expansions: a Quasi-experimental Study. JAMA Intern Med. 2016;164:795-803.
Sommers BD, Blendon RJ, Orav EJ, Epstein AM. Changes in utilization and health among low-income adults after Medicaid expansion or expanded private insurance. JAMA Intern Med. 2016;176:1501-1509.
Van der Wees PJ, Zaslavsky AM, Ayanian JZ. Improvements in health status after Massachusetts health care reform. Milbank Q. 2013;91:663-89.
Askelson NM, Wright B, Bentler S, Momany ET, Damiano P. Iowa’s Medicaid expansion promoted healthy behaviors but was challenging to implement and attracted few participants. Health Affairs. 2017;36(5).
Blumenthal KJ, Saulsgiver KA, Norton L, et al. Medicaid incentive programs to encourage healthy behavior show mixed results to date and should be studied and improved. Health Affairs. 2013;32(3).
Saunders R, Vulimiri M, Japinga M, Bleser W, Wong C. Are carrots good for your health? Current Evidence on Health Behavior Incentives in the Medicaid Program. June 2018. https://healthpolicy.duke.edu/sites/default/files/atoms/files/duke_healthybehaviorincentives_6.1.pdf. Accessed 12/28/18.
Brunette MF, Pratt SI, Barteis SJ, Schere EA, Sigmon SC, Ferron JC, Santos M, Williams GE, Kosydar S, Wolfe RS, Lotz D, Capuchino K. Randomized trial of interventions for smoking cessation among Medicaid beneficiaries with mental illness psychiatric services. 2018;69(3):274-280.
Soni A, Simon K, Cawley J, Sabik L. Effect of Medicaid expansions of 2014 on overall and early-stage cancer diagnoses. Am J Public Health. 2018;108(2);216-218.
Finkelstein A, Taubman S, Wright B, et al. The Oregon health insurance experiment: evidence from the first year. Q J Econ. 2012;127(3):1057-1106.
Sommers B, Maylone B, Blendon R, Orav EJ, Epstein A. “Three-Year Impacts of the Affordable Care Act: Improved Medical Care and Health Among Low-Income Adults,” Health Affairs epub ahead of print (May 2017). http://content.healthaffairs.org/content/early/2017/05/15/hlthaff.2017.0293.
Acknowledgments
The University of Michigan Institute for Healthcare Policy and Innovation (IHPI) is conducting the evaluation required by the Centers for Medicare and Medicaid Services (CMS) of the Healthy Michigan Plan (HMP) under contract with the Michigan Department of Health and Human Services (MDHHS). Data collection was funded by MDHHS and CMS for the purposes of the evaluation, but the findings in this paper do not represent the official views of either agency.
Support was also provided by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development (HSR&D) Service to Dr. Kullgren as a VA HSR&D Career Development awardee at the Ann Arbor VA. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government. The authors gratefully acknowledge the advice, insights, and efforts of the DECIDERS Steering Committee and other community leaders who served on our community advisory board.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Kullgren has received consulting fees from SeeChange Health, HealthMine, and the Kaiser Permanente Washington Health Research Institute and honoraria from the Robert Wood Johnson Foundation, AbilTo, Inc., the Kansas City Area Life Sciences Institute, and the American Diabetes Association.
Dr. Goold and all coauthors report no other financial relationships that could influence or be perceived to influence the submitted work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 149 KB).
Rights and permissions
About this article

Cite this article
Goold, S.D., Tipirneni, R., Chang, T. et al. Primary Care, Health Promotion, and Disease Prevention with Michigan Medicaid Expansion. J GEN INTERN MED 35, 800–807 (2020). https://doi.org/10.1007/s11606-019-05370-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-019-05370-3