
Abstract
Purpose
To review the techniques and technical success rate of adrenal venous sampling (AVS) in patients with inferior vena cava (IVC) or renal vein anomalies.
Materials and methods
The techniques and success rate of AVS in 15 patients with anomalies [8 with double IVC (dIVC), 3 with left IVC (ltIVC), 2 with retroaortic left renal vein (LRV), and 2 with circumaortic LRV] underwent AVS was retrospectively reviewed.
Results
Among 11 patients with IVC anomalies, the success rates for sampling the right and left adrenal veins (RAV and LAV) were 81.8 and 90.9%, respectively. In dIVC, the LAV was selected using the following four methods: approaching through the right IVC from the right femoral vein, flipping the LAV catheter tip in the LRV (n = 4) or the interiliac-communicating vein (n = 1), or through the ltIVC from the right (n = 1) or left (n = 2) femoral vein. Among the four patients with LRV anomalies, the success rate was 100% for each adrenal vein.
Conclusion
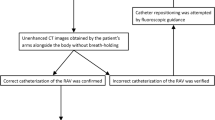
AVS can be successfully performed in patients with anomalies. The key to technical success is understanding the venous anatomy based on pre-procedural CT images and choosing appropriate methods.





Similar content being viewed by others


References
Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, Tamura N, Task Force Committee on Primary Aldosteronism, The Japan Endocrine Society, et al. Guidelines for the diagnosis and treatment of primary aldosteronism—the Japan Endocrine Society 2009. Endocr J. 2011;58(9):711–21.
Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008;93(9):3266–81.
Rossi GP, Auchus RJ, Brown M, Lenders JWM, Naruse M, Plouin PF, et al. An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism. Hypertension. 2014;63(1):151–60.
Morita S, Yamazaki H, Sonoyama Y, Nishina Y, Ichihara A, Sakai S. Successful adrenal venous sampling by non-experts with reference to CT images. Cardiovasc Intervent Radiol. 2016;39(7):1001–6.
Satani N, Ota H, Seiji K, Morimoto R, Kudo M, Iwakura Y, et al. Intra-adrenal aldosterone secretion: segmental adrenal venous sampling for localization. Radiology. 2016;278(1):265–74.
Sakamoto A, Urushida T, Sakakibara T, Sano M, Suwa K, Saitoh T, et al. Accidental entrapment of electrical mapping catheter by Chiari’s network in right atrium during catheter ablation procedure. Case Rep Cardiol. 2016;2016:1302473.
Takahashi K, Akabane M, Nishimatsu H, Suzuki H, Takeshita M, Matsui H, et al. Chiari network: a potential pitfall in adrenal venous sampling. Folia Endocrinol Jpn. 2007;83(1):162.
Morita S, Higuchi M, Saito N, Mitsuhashi N. Pelvic venous variations in patients with congenital inferior vena cava anomalies: classification with computed tomography. Acta Radiol. 2007;48(9):974–9.
Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000;20:639–52.
Kadir Saadoon. Loop catheter technique: a simple, rapid method for left adrenal vein catheterization. AJR. 1980;134:31–3.
Matsuura T, Takase K, Ota H, Yamada T, Sato A, Satoh F, et al. Radiologic anatomy of the right adrenal vein: preliminary experience with MDCT. Am J Roentgenol. 2008;191(2):402–8.
Omura K, Ota H, Takahashi Y, Matsuura T, Seiji K, Arai Y, et al. Anatomical variations of the right adrenal vein: concordance between multidetector computed tomography and catheter venography. Hypertension. 2017;69(3):428–34.
Morita S, Endo K, Suzaki S, Ishizaki U, Yamazaki H, Nishina Y, et al. Reduction of radiation exposure using dynamic trace digital angiography and spot fluoroscopy during adrenal venous sampling. Cardiovasc Intervent Radiol. 2017;40(5):697–703.
Acknowledgements
We have no acknowledgement.
Funding
We have received no Grants related to this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared no conflicts of interest.
Ethical approval
This retrospective, single-institution study was approved by the institutional review board of our facility.
Informed consent
Written informed consent for the inclusion of individual patient data in the analysis was waived because of the retrospective nature of the investigation. All patients gave their consent for the AVS procedure.
About this article

Cite this article
Endo, K., Morita, S., Suzaki, S. et al. Techniques of adrenal venous sampling in patients with inferior vena cava or renal vein anomalies. Jpn J Radiol 36, 407–413 (2018). https://doi.org/10.1007/s11604-018-0732-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-018-0732-5