
Abstract
Background
Fluoroscopic criteria have been described for the documentation of septal right ventricular (RV) lead positioning, but their accuracy remains questioned.
Methods and results
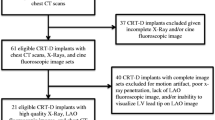
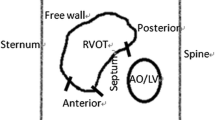
Consecutive patients undergoing pacemaker or defibrillator implantation were prospectively included. RV lead was positioned using postero-anterior and left anterior oblique 40° incidences, and right anterior oblique 30° to rule out coronary sinus positioning when suspected. RV lead positioning using fluoroscopy was compared to true RV lead positioning as assessed by transthoracic echocardiography (TTE). Precise anatomical localizations were determined with both modalities; then, RV lead positioning was ultimately dichotomized into two simple clinically relevant categories: RV septal or RV free wall. Accuracy of fluoroscopy for RV lead positioning was then assessed by comparison with TTE. We included 100 patients. On TTE, 66/100 had a septal RV lead and 34/100 had a free wall RV lead. Fluoroscopy had moderate agreement with TTE for precise anatomical localization of RV lead (k = 0.53), and poor agreement for septal/free wall localization (k = 0.36). For predicting septal RV lead positioning, classical fluoroscopy criteria had a high sensitivity (95.5%; 63/66 patients having a septal RV lead on TTE were correctly identified by fluoroscopy) but a very low specificity (35.3%; only 12/34 patients having a free wall RV lead on TTE were correctly identified by fluoroscopy).
Conclusion
Classical fluoroscopy criteria have a poor accuracy for identifying RV free wall leads, which are most of the time misclassified as septal. This raises important concerns about the efficacy and safety of RV lead positioning using classical fluoroscopy criteria.



Similar content being viewed by others

References
Cano O, Andres A, Alonso P, Osca J, Sancho-Tello MJ, Olague J, et al. Incidence and predictors of clinically relevant cardiac perforation associated with systematic implantation of active-fixation pacing and defibrillation leads: a single-centre experience with over 3800 implanted leads. Europace. 2017;19:96–102.
Shimony A, Eisenberg MJ, Filion KB, Amit G. Beneficial effects of right ventricular non-apical vs. apical pacing: a systematic review and meta-analysis of randomized-controlled trials. Europace. 2012;14:81–91.
Margulescu AD, Suran BM, Rimbas RC, Dulgheru RE, Siliste C, Vinereanu D. Accuracy of fluoroscopic and electrocardiographic criteria for pacemaker lead implantation by comparison with three-dimensional echocardiography. J Am Soc Echocardiogr. 2012;25:796–803.
Pang BJ, Joshi SB, Lui EH, Tacey MA, Ling LH, Alison J, et al. Validation of conventional fluoroscopic and ECG criteria for right ventricular pacemaker lead position using cardiac computed tomography. Pacing Clin Electrophysiol. 2014;37:495–504.
Sharma G, Salahuddin S, Sanders P, Gupta H, Gulati G, Jagia P, et al. Inadequacy of fluoroscopy and electrocardiogram in predicting septal position in RVOT pacing—validation with cardiac computed tomography. Indian Heart J. 2016;68:174–80.
Squara F, Tomi J, Scarlatti D, Theodore G, Moceri P, Ferrari E. Self-taught axillary vein access without venography for pacemaker implantation: prospective randomized comparison with the cephalic vein access. Europace 2017;1;19(12):2001–2006
McGavigan AD, Roberts-Thomson KC, Hillock RJ, Stevenson IH, Mond HG. Right ventricular outflow tract pacing: radiographic and electrocardiographic correlates of lead position. Pacing Clin Electrophysiol. 2006;29:1063–8.
Mond HG, Hillock RJ, Stevenson IH, McGavigan AD. The right ventricular outflow tract: the road to septal pacing. Pacing Clin Electrophysiol. 2007;30:482–91.
Mond HG. The road to right ventricular septal pacing: techniques and tools. Pacing Clin Electrophysiol. 2010;33:888–98.
Hillock RJ, Mond HG. Pacing the right ventricular outflow tract septum: time to embrace the future. Europace. 2012;14:28–35.
Burri H, Park CI, Zimmermann M, Gentil-Baron P, Stettler C, Sunthorn H, et al. Utility of the surface electrocardiogram for confirming right ventricular septal pacing: validation using electroanatomical mapping. Europace. 2011;13:82–6.
Andrikopoulos G, Tzeis S, Asbach S, Semmler V, Lennerz C, Solzbach U, et al. A stepwise electrocardiographic algorithm for differentiation of mid-septal vs. apical right ventricular lead positioning: the SPICE ECG substudy. Europace. 2015;17:915–20.
Engblom H, Hedstrom E, Palmer J, Wagner GS, Arheden H. Determination of the left ventricular long-axis orientation from a single short-axis MR image: relation to BMI and age. Clin Physiol Funct Imaging. 2004;24:310–5.
Cano O, Osca J, Sancho-Tello MJ, Sanchez JM, Ortiz V, Castro JE, et al. Comparison of effectiveness of right ventricular septal pacing versus right ventricular apical pacing. Am J Cardiol. 2010;105:1426–32.
Occhetta E, Bortnik M, Magnani A, Francalacci G, Piccinino C, Plebani L, et al. Prevention of ventricular desynchronization by permanent para-Hisian pacing after atrioventricular node ablation in chronic atrial fibrillation: a crossover, blinded, randomized study versus apical right ventricular pacing. J Am Coll Cardiol. 2006;47:1938–45.
Stambler BS, Ellenbogen K, Zhang X, Porter TR, Xie F, Malik R, et al. Right ventricular outflow versus apical pacing in pacemaker patients with congestive heart failure and atrial fibrillation. J Cardiovasc Electrophysiol. 2003;14:1180–6.
Victor F, Leclercq C, Mabo P, Pavin D, Deviller A, de Place C, et al. Optimal right ventricular pacing site in chronically implanted patients: a prospective randomized crossover comparison of apical and outflow tract pacing. J Am Coll Cardiol. 1999;33:311–6.
Victor F, Mabo P, Mansour H, Pavin D, Kabalu G, de Place C, et al. A randomized comparison of permanent septal versus apical right ventricular pacing: short-term results. J Cardiovasc Electrophysiol. 2006;17:238–42.
Burri H, Domenichini G, Sunthorn H, Ganiere V, Stettler C. Comparison of tools and techniques for implanting pacemaker leads on the ventricular mid-septum. Europace. 2012;14:847–52.
Osmancik P, Stros P, Herman D, Curila K, Petr R. The insufficiency of left anterior oblique and the usefulness of right anterior oblique projection for correct localization of a computed tomography-verified right ventricular lead into the midseptum. Circ Arrhythm Electrophysiol. 2013;6:719–25.
Chen D, Wei H, Tang J, Liu L, Wu S, Lin C, et al. A randomized comparison of fluoroscopic techniques for implanting pacemaker lead on the right ventricular outflow tract septum. Int J Cardiovasc Imaging. 2016;32:721–8.
Gudal M, Kervancioglu C, Oral D, Gurel T, Erol C, Sonel A. Permanent pacemaker implantation in a pregnant woman with the guidance of ECG and two-dimensional echocardiography. Pacing Clin Electrophysiol. 1987;10:543–5.
Pedrinazzi C, Gazzaniga P, Durin O, Tovena D, Inama G. Implantation of a permanent pacemaker in a pregnant woman under the guidance of electrophysiologic signals and transthoracic echocardiography. J Cardiovasc Med (Hagerstown). 2008;9:1169–72.
Moore P, Coucher J, Ngai S, Stanton T, Wahi S, Gould P, et al. Imaging and right ventricular pacing lead position: a comparison of CT, MRI, and echocardiography. Pacing Clin Electrophysiol. 2016;39:382–92.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Yes (institutional ethics committee).
Informed consent
Yes.
Rights and permissions
About this article

Cite this article
Squara, F., Scarlatti, D., Riccini, P. et al. Classical fluoroscopy criteria poorly predict right ventricular lead septal positioning by comparison with echocardiography. J Interv Card Electrophysiol 52, 209–215 (2018). https://doi.org/10.1007/s10840-018-0355-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-018-0355-x