
Abstract
Purpose
To evaluate which is the minimum number of oocytes to be allocated to each recipient in a shared egg donor program.
Methods
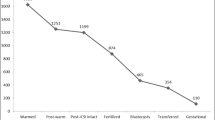
We analyzed 953 recipients that received at least 4 metaphase II (MII) oocytes in the period 2006–2008. We retrospectively divided the recipients according to the number of MII oocytes actually received.
Results
No statistically significant differences were found among the analyzed strata in clinical pregnancy rate (A:43.7%; B:45.6%; C:48.6%; D:45.5%; E:53%, P = NS) and miscarriage rate. However, the rate of top quality transferred embryos, and the embryo freezing rate were significantly higher among those recipients that received 7 or more mature eggs.
Conclusions
After a large sample was analyzed, no significant differences in fresh embryo transfer outcome were encountered when a different number of oocytes was allocated. A minimum of 4 MII oocytes seems to achieve satisfactory pregnancy rates in our shared egg donor program.
Similar content being viewed by others


References
Bustillo M, Buster JE, Cohen SW, Hamilton F, Thorneycroft IH, Simon JA, et al. Delivery of a healthy infant following nonsurgical ovum transfer. JAMA. 1984;251(7):889.
Navot D, Laufer N, Kopolovic J, Rabinowitz R, Birkenfeld A, Lewin A, et al. Artificially induced endometrial cycles and establishment of pregnancies in the absence of ovaries. N Engl J Med. 1986;314(13):806–11.
Buster JE, Bustillo M, Thorneycroft I, Simon JA, Boyers SP, Marshall JR, et al. Non-surgical transfer of an in-vivo fertilised donated ovum to an infertility patient. Lancet. 1983;1(8328):816–7.
Registro Latinoamericano de Reproducción Asistida. Registro Latinoamericano (RLA). 2007 [updated 2007; cited 23/10/2009]; Available from: http://www.redlara.com/esp/reg_2007.asp.
Nyboe Andersen A, Goossens V, Bhattacharya S, Ferraretti AP, Kupka MS, de Mouzon J, et al. Assisted reproductive technology and intrauterine inseminations in Europe, 2005: results generated from European registers by ESHRE: ESHRE. The European IVF Monitoring Programme (EIM), for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod. 2009;24(6):1267–87.
SART. Clinical Summary Report (2007). 2009 [updated 2009; cited 13/01/2010]; Available from: https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?ClinicPKID=0.
Glujovsky D, Fiszbajn G, Lipowicz R, Lavolpe M, Sueldo C. Practice of sharing donated oocytes among several recipients. Fertil Steril. 2006;86(6):1786–8.
Moomjy M, Mangieri R, Beltramone F, Cholst I, Veeck L, Rosenwaks Z. Shared oocyte donation: society’s benefits. Fertil Steril. 2000;73(6):1165–9.
Blyth E. Subsidized IVF: the development of ‘egg sharing’ in the United Kingdom. Hum Reprod. 2002;17(12):3254–9.
Oyesanya OA, Olufowobi O, Ross W, Sharif K, Afnan M. Prognosis of oocyte donation cycles: a prospective comparison of the in vitro fertilization-embryo transfer cycles of recipients who used shared oocytes versus those who used altruistic donors. Fertil Steril. 2009;92(3):930–6.
Patrizio P, Sakkas D. From oocyte to baby: a clinical evaluation of the biological efficiency of in vitro fertilization. Fertil Steril. 2009;91(4):1061–6.
Inge GB, Brinsden PR, Elder KT. Oocyte number per live birth in IVF: were Steptoe and Edwards less wasteful? Hum Reprod. 2005;20(3):588–92.
Mullin CM, Fino ME, Talebian S, Keegan D, Grifo JA, Licciardi F. Comparison of pregnancy outcomes in anonymous shared versus exclusive donor oocyte in vitro fertilization cycles. Fertil Steril. 2009;93(2):574–8.
Kolibianakis EM, Tournaye H, Osmanagaoglu K, Camus M, Van Waesberghe L, Van Steirteghem A, et al. Outcome for donors and recipients in two egg-sharing policies. Fertil Steril. 2003;79(1):69–73.
ASRM. Guidelines for gamete and embryo donation. Fertil Steril. 2006;86(5):S38.
Cohen MA, Lindheim SR, Sauer MV. Donor age is paramount to success in oocyte donation. Hum Reprod. 1999;14(11):2755–8.
Shulman A, Frenkel Y, Dor J, Levran D, Shiff E, Maschiach S. The best donor. Hum Reprod. 1999;14(10):2493–6.
Harris SE, Faddy M, Levett S, Sharma V, Gosden R. Analysis of donor heterogeneity as a factor affecting the clinical outcome of oocyte donation. Hum Fertil (Camb). 2002;5(4):193–8.
Mirkin S, Gimeno TG, Bovea C, Stadtmauer L, Gibbons WE, Oehninger S. Factors associated with an optimal pregnancy outcome in an oocyte donation program. J Assist Reprod Genet. 2003;20(10):400–8.
Letterie G, Marshall L, Angle M. The relationship of clinical response, oocyte number, and success in oocyte donor cycles. J Assist Reprod Genet. 2005;22(3):115–7.
ASRM. Guidelines on number of embryos transferred. Fertil Steril. 2006;86(5 Suppl):S51–2.
Sauer MV, Kavic SM. Oocyte and embryo donation 2006: reviewing two decades of innovation and controversy. Reprod Biomed Online. 2006;12(2):153–62.
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule Allocating a minimum of 4 MII oocytes seems to achieve satisfactory pregnancy rates in shared egg donation cycles.
Rights and permissions
About this article
Cite this article
Glujovsky, D., Dominguez, M., Fiszbajn, G. et al. A shared egg donor program: which is the minimum number of oocytes to be allocated?. J Assist Reprod Genet 28, 263–267 (2011). https://doi.org/10.1007/s10815-010-9511-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-010-9511-7