Abstract
Purpose
To describe clinical characteristics and outcomes of treatment in patients with presumed tuberculous uveitis (PTU).
Methods
All patients diagnosed with PTU between January 1996 and March 2013 were reviewed. The diagnosis was made when clinical findings were consistent with possible intraocular tuberculosis, strongly positive purified protein derivative (PPD) skin test result, and response to anti-tuberculous therapy with no other cause of uveitis as suggested by history, symptoms, or ancillary testing.
Results
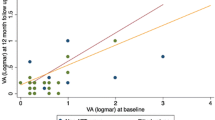
Ninety patients (141 eyes) were identified. There were 43 males (47.3%) and 47 females (52.7%). Mean age was 48.2 ± 14.4 years. Mean duration of symptoms prior to presentation was 6.7 ± 8.3 months. Ten eyes (7.1%) had anterior uveitis, 18 eyes (12.8%) had intermediate uveitis, 34 eyes (24.1%) had posterior uveitis, and 79 eyes (56%) had panuveitis. Macular edema was present in 33.3% of the eyes at presentation. All patients received anti-tuberculous therapy and systemic corticosteroids. Mean follow-up after completion of therapy was 36 ± 2.5 months. Only 2 eyes developed recurrent inflammation after treatment completion. At last follow-up, all eyes showed resolution of inflammation, associated with significant improvement in visual acuity. There was a significant positive correlation between initial and final VA. Eyes that had macular edema at presentation showed a significant reduction in central macular thickness at final follow-up.
Conclusions
There is delay in presentation of patients with PTU. The most common anatomic diagnosis was panuveitis. Treatment with anti-tuberculous therapy combined with systemic corticosteroids resulted in resolution of inflammation and macular edema with significant improvement in visual acuity.









Similar content being viewed by others

References
Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC (1999) Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA 282:677–686
World Health Organisation. Tuberculosis Fact Sheet 2015. World Health Organization; 2016. http://www.who.int/mediacentre/factsheets/fs104/en/. Accessed 21 November 2016
Centers for Disease Control (USA). Tuberculosis—Data and Statistics 2015. http://www.cdc.gov/tb/statistics/default.htm. Accessed 21 November 2017
Al-Mezaine HS, Kangave D, Abu El-Asrar AM (2010) Patterns of Uveitis in patients admitted to a university hospital in Riyadh, Saudi Arabia. Ocul Immunol Inflamm 18:424–431
Al Dhahri H, Al Rubaie K, Hemachandran S et al (2015) Patterns of uveitis in a university-based tertiary referral center in Riyadh, Saudi Arabia. Ocul Immunol Inflamm 23:311–319
Amin RM, Goweida M, Bedda A, Kamel A, Radwan A (2016) Clinical patterns and causes of intraocular inflammation in a uveitis patient cohort from Egypt. Ocul Immunol Inflamm. https://doi.org/10.1080/09273948.2016.1236972
Nguyen M, Siak J, Chee SP, Diem VQ (2016) The spectrum of uveitis in Southern vietnam. Ocul Immunol Inflamm. https://doi.org/10.1080/09273948.2016.1231826
Kianersi F, Mohammadi Z, Ghanbari H, Ghoreyshi SM, Karimzadeh H, Soheilian M (2015) Clinical patterns of uveitis in an iranian tertiary eye-care center. Ocul Immunol Inflamm 23:278–282
Vos AG, Wassenberg MWM, de Hoog J, Oosterheert JJ (2013) Diagnosis and treatment of tuberculous uveitis in a low endemic setting. Int J Infect Dis 17:e993–e999
Llorenç Bellés V, Adán Civera A, Espinosa Garriga G et al (2012) Uveitis diagnosis characterization at a referral centre in the area of Barcelona, Spain. Med Clin (Barc) 138:277–282
Ducommun M-A, Eperon S, Khonkarly MB, Cavassini M, Guex-Crosier Y (2012) Long-term close follow-up of chorioretinal lesions in presumed ocular tuberculosis. Eur J Ophthalmol 22:195–202
Sanghvi C, Bell C, Woodhead M, Hardy C, Jones N (2011) Presumed tuberculous uveitis: diagnosis, management, and outcome. Eye 25:475–480. https://doi.org/10.1038/eye.2010.235
Kazokoglu H, Onal S, Tugal-Tutkun I et al (2008) Demographic and clinical features of uveitis in tertiary centers in Turkey. Ophthalmic Epidemiol 15:285–293
Pathanapitoon K, Kunavisarut P, Ausayakhun S, Sirirungsi W, Rothova A (2008) Uveitis in a tertiary ophthalmology centre in Thailand. Br J Ophthalmol 92:474–478
Khairallah M, Ben Yahia S, Ladjimi A et al (2007) Pattern of uveitis in a referral centre in Tunisia, North Africa. Eye 21:33–39
Rathinam SR, Namperumalsamy P (2007) Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol 55:173–183
Yang P, Zhang Z, Zhou H et al (2005) Clinical patterns and characteristics of uveitis in a tertiary center for uveitis in China. Curr Eye Res 30:943–948
Sengün A, Karadağ R, Karakurt A, Saricaoğlu MS, Abdik O, Hasiripi H (2005) Causes of uveitis in a referral hospital in Ankara, Turkey. Ocul Immunol Inflamm 13:45–50
Soheilian M, Heidari K, Yazdani S, Shahsavari M, Ahmadieh H, Dehghan M (2004) Patterns of uveitis in a tertiary eye care center in Iran. Ocul Immunol Inflamm 12:297–310
Singh R, Gupta V, Gupta A (2004) Pattern of uveitis in a referral eye clinic in north India. Indian J Ophthalmol 52:121–125
Wakabayashi T, Morimura Y, Miyamoto Y, Okada AA (2003) Changing patterns of intraocular inflammatory disease in Japan. Ocul Immunol Inflamm 11:277–286
Islam SMM, Tabbara KF (2002) Causes of uveitis at the eye center in Saudi Arabia: a retrospective review. Ophthalmic Epidemiol 9:239–249
Mercanti A, Parolini B, Bonora A, Lequaglie Q, Tomazzoli L (2001) Epidemiology of endogenous uveitis in north-eastern Italy. Analysis of 655 new cases. Acta Ophthalmol Scand 79:64–68
Kaimbo Wa Kimbo D, Bifuko A, Dernouchamps JP, Missotten L (1998) Chronic uveitis in Kinshasa (D R Congo). Bull Soc Belge Ophtalmol 270:95–100
Kotake S, Furudate N, Sasamoto Y, Yoshikawa K, Goda C, Matsuda H (1997) Characteristics of endogenous uveitis in Hokkaido, Japan. Graefes Arch Clin Exp Ophthalmol 235:5–9
Merrill PT, Kim J, Cox TA, Betor CC, McCallum RM, Jaffe GJ (1997) Uveitis in the southeastern United States. Curr Eye Res 16:865–874
Rodriguez A, Calonge M, Pedroza-Seres M, et al (1996) Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol (Chicago, Ill 1960) 114:593–599
Thean LH, Thompson J, Rosenthal AR (1996) A uveitis register at the Leicester royal Infirmary. Ophthalmic Epidemiol 3:151–158
Smit RL, Baarsma GS (1995) Epidemiology of uveitis. Curr Opin Ophthalmol 6:57–61
Weiner A, BenEzra D (1991) Clinical patterns and associated conditions in chronic uveitis. Am J Ophthalmol 112:151–158
Palmares J, Coutinho MF, Castro-Correia J (1990) Uveitis in northern Portugal. Curr Eye Res 9(Suppl):31–34
Rosen PH, Spalton DJ, Graham EM (1990) Intraocular tuberculosis. Eye 4:486–492
Sheu SJ, Shyu JS, Chen LM, Chen YY, Chirn SC, Wang JS (2001) Ocular manifestations of tuberculosis. Ophthalmology 108:1580–1585
Sakai J, Matsuzawa S, Usui M, Yano I (2001) New diagnostic approach for ocular tuberculosis by ELISA using the cord factor as antigen. Br J Ophthalmol 85:130–133
Al-Mezaine HS, Al-Muammar A, Kangave D, Abu El-Asrar AM (2008) Clinical and optical coherence tomographic findings and outcome of treatment in patients with presumed tuberculous uveitis. Int Ophthalmol 28:413–423
Sarvananthan N, Wiselka M, Bibby K (1998) Intraocular tuberculosis without detectable systemic infection. Arch Ophthalmol (Chicago, III 1960) 116:1386–1388
Cimino L, Herbort CP, Aldigeri R, Salvarani C, Boiardi L (2009) Tuberculous uveitis, a resurgent and underdiagnosed disease. Int Ophthalmol 29:67–74
Morimura Y, Okada AA, Kawahara S et al (2002) Tuberculin skin testing in uveitis patients and treatment of presumed intraocular tuberculosis in Japan. Ophthalmology 109:851–857
Wolfensberger TJ, Piguet B, Herbort CP (1999) Indocyanine green angiographic features in tuberculous chorioretinitis. Am J Ophthalmol 127:350–353
Abu El-asrar A, Abouammoh M, Al-mezaine HS (2009) Tuberculous uveitis. Middle East Afr J Ophthalmol 16:188–201
Alvarez S, McCabe WR (1984) Extrapulmonary tuberculosis revisited: a review of experience at Boston City and other hospitals. Med 63:25–55
Schlaegel TF, Weber JC (1969) Double-blind therapeutic trial of isoniazid in 344 patients with uveitis. Br J Ophthalmol 53:425–427
Woods AC, Wood R, Senterfit LB (1958) Studies in experimental ocular tuberculosis. XVIII. The effect of cortisone combined with specific antibacterial therapy on experimental ocular tuberculosis in the immune-allergic rabbit. AMA Arch Ophthalmol 59:559–578
Hamade IH, Tabbara KF (2010) Complications of presumed ocular tuberculosis. Acta Ophthalmol 88:905–909
Gupta V, Gupta A, Rao NA (2007) Intraocular Tuberculosis—An Update. Surv Ophthalmol 52:561–587
Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group (2005) Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 140(3):509–516
Rowland K, Guthmann R, Jamieson B, Malloy D (2006) Clinical inquiries. How should we manage a patient with a positive PPD and prior BCG vaccination? J Fam Pract 55:718–720
Manousaridis K, Ong E, Stenton C, Gupta R, Browning AC, Pandit R (2013) Clinical presentation, treatment, and outcomes in presumed intraocular tuberculosis: experience from Newcastle upon Tyne, UK. Eye (Lond) 27:480–486. https://doi.org/10.1038/eye.2013.11
Llorenç V, González-Martin J, Keller J et al (2013) Indirect supportive evidence for diagnosis of tuberculosis-related uveitis: from the tuberculin skin test to the new interferon gamma release assays. Acta Ophthalmol 91:99–107. https://doi.org/10.1111/j.1755-3768.2012.02564.x
Mao Y, Peng XY, You QS, Wang H, Zhao M, Jonas JB (2014) Tuberculous uveitis in China. Acta Ophthalmol 92:393–397. https://doi.org/10.1111/aos.12351
Basu S, Monira S, Modi RR et al (2014) Degree, duration, and causes of visual impairment in eyes affected with ocular tuberculosis. J Ophthalmic Inflamm Infect 4:3. https://doi.org/10.1186/1869-5760-4-3
La Distia Nora R, Van Velthoven MEJ, Ten Dam-Van Loon NH et al (2014) Clinical manifestations of patients with intraocular inflammation and positive QuantiFERON-TB gold in-tube test in a country nonendemic for tuberculosis. Am J Ophthalmol 157:754–761
Khochtali S, Gargouri S, Abroug N et al (2015) The spectrum of presumed tubercular uveitis in Tunisia, North Africa. Int Ophthalmol 35:663–671
Gunasekeran DV, Gupta B, Cardoso J, Pavesio CE, Agrawal R (2017) Visual morbidity and ocular complications in presumed intraocular tuberculosis: an analysis of 354 cases from a non-endemic population. Ocul Immunol Inflamm. https://doi.org/10.1080/09273948.2017.1296580
Gineys R, Bodaghi B, Carcelain G et al (2011) QuantiFERON-TB gold cut-off value: implications for the management of tuberculosis-related ocular inflammation. Am J Ophthalmol 152(433–440):e1
Gupta V, Arora S, Gupta A, Ram J, Bambery P, Sehgal S (1998) Management of presumed intraocular tuberculosis: possible role of the polymerase chain reaction. Acta Ophthalmol Scand 76:679–682
Bansal R, Gupta A, Gupta V, Dogra MR, Sharma A, Bambery P (2012) Tubercular serpiginous-like choroiditis presenting as multifocal serpiginoid choroiditis. Ophthalmology 119:2334–2342
El-Asrar AMA, Al-Kharashi SA (2002) Full panretinal photocoagulation and early vitrectomy improve prognosis of retinal vasculitis associated with tuberculoprotein hypersensitivity (Eales’ disease). Br J Ophthalmol 86:1248–1251
Helm CJ, Holland GN (1993) Ocular tuberculosis. Surv Ophthalmol 38:229–256
Vasconcelos-Santos DV, Rao PK, Davies JB, Sohn EH, Rao NA (2010) Clinical features of tuberculous serpiginouslike choroiditis in contrast to classic serpiginous choroiditis. Arch Ophthalmol 128:853–858
Massaro D, Katz S, Sachs M (1964) Choroidal tubercles. a clue to hematogenous tuberculosis. Ann Intern Med 60:231–241
Cangemi FE, Friedman AH, Josephberg R (1980) Tuberculoma of the choroid. Ophthalmology 87:252–258
Mansour AM, Haymond R (1990) Choroidal tuberculomas without evidence of extraocular tuberculosis. Graefes Arch Clin Exp Ophthalmol 228:382–383
Alaraj AM, Al-Dhibi H, Al-Mezaine HS, Abu El-Asrar AM (2013) Solitary presumed choroidal tuberculomas masquerading as choroidal tumors. Saudi Med J 34:86–90
Lardenoye CWTA, van Kooij B, Rothova A (2006) Impact of Macular Edema on Visual Acuity in Uveitis. Ophthalmology 113:1446–1449
Babu K, Satish V, Prakash O, Subbakrishna DK, Murthy KR (2009) Role of the mantoux test and treatment with antitubercular therapy in a South Indian patient population of presumed intraocular tuberculosis. Ocul Immunol Inflamm 17:307–311
Ang M, Wong WL, Li X, Chee S-P (2013) Interferon γ release assay for the diagnosis of uveitis associated with tuberculosis: a Bayesian evaluation in the absence of a gold standard. Br J Ophthalmol 97:1062–1067
Bodaghi B, LeHoang P (2000) Ocular tuberculosis. Curr Opin Ophthalmol 11:443–448
Gupta V, Gupta A, Arora S, Bambery P, Dogra MR, Agarwal A (2003) Presumed tubercular serpiginouslike choroiditis: clinical presentations and management. Ophthalmology 110:1744–1749
Gupta A, Gupta V, Arora S, Dogra MR, Bambery P (2001) PCR-positive tubercular retinal vasculitis: clinical characteristics and management. Retina 21:435–444
Bansal R, Gupta A, Gupta V, Dogra MR, Bambery P, Arora SK (2008) Role of anti-tubercular therapy in uveitis with latent/manifest tuberculosis. Am J Ophthalmol 146(772–779):e2
Agarwal A, Handa S, Aggarwal K, Sharma M, Singh R, Sharma A, Agrawal R, Sharma K, Gupta V (2017) The role of dexamethasone implant in the management of tubercular uveitis. Ocul Immunol Inflamm. https://doi.org/10.1080/09273948.2017.1400074. [Epub ahead of print]
Jain L, Panda KG, Basu S (2017) Clinical outcomes of adjunctive sustained-release intravitreal dexamethasone implants in tuberculosis-associated multifocal serpigenoid choroiditis. Ocul Immunol Inflamm. https://doi.org/10.1080/09273948.2017.1383446. [Epub ahead of print]
Rao NA, Saraswathy S, Smith RE et al (2006) Tuberculous uveitis: distribution of Mycobacterium tuberculosis in the Retinal Pigment Epithelium. Arch Ophthalmol 124:1777
Acknowledgements
The authors thank Ms. Connie Unisa-Marfil for secretarial assistance. This work was supported by King Saud University through Vice Deanship of Research Chair (Dr. Nasser Al-Rashid Research Chair in Ophthalmology [AMA]), Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they do not have any conflict of interest on the content of manuscript and study undertaken.
Rights and permissions
About this article

Cite this article
Al-Qarni, A., Abouammoh, M.A., Almousa, A.N. et al. Presumed tuberculous uveitis in a university-based tertiary referral center in Saudi Arabia. Int Ophthalmol 39, 317–333 (2019). https://doi.org/10.1007/s10792-017-0815-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-017-0815-9