
Abstract
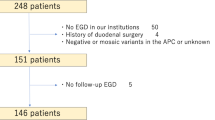
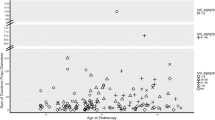
Duodenal polyposis is found in the majority of patients with familial adenomatous polyposis. Endoscopic surveillance programmes grade the severity of duodenal disease according to the Spigelman classification (stages 0–IV) to identify patients at risk of developing adenocarcinoma. To evaluate the progression of duodenal polyposis in patients with a previous diagnosis of Spigelman stage IV disease who have been downstaged by endoscopic or pharmacological means. A database search of a large polyposis registry identified patients who had been downstaged from stage IV disease and had further opportunity for disease progression. These patients were divided into three groups according to their new Spigelman stage. A measure of a patient’s disease progression was obtained by the increase in stage over the recommended follow up time period for their new, reduced, Spigelman stage. Group 1 (n = 16) were downstaged to stage III disease, with 50 % progressing back to stage IV over the recommended 1-year follow up period. Group 2 (n = 19) were downstaged to stage II disease, with 84 % progressing over the recommended 3-year follow up period. Group 3 (n = 6) were downstaged to stage I disease, with 100 % progressing over the recommended 5-year follow up period. Patients downstaged from Spigelman stage IV demonstrate an increased rate of disease progression in comparison to reported rates of primary disease progression. An amendment to the current endoscopic surveillance protocol is recommended to ensure that once a patient has been diagnosed with stage IV disease they are treated as a high-risk patient in perpetuity.

Similar content being viewed by others

References
Vasen HF, Moslein G, Alonso A, Aretz S et al (2008) Guidelines for the clinical management of familial adenomatous polyposis (FAP). Gut 57(5):704–713
Nugent KP, Spigelman AD, Phillips RK (1993) Life expectancy after colectomy and ileorectal anastomosis for familial adenomatous polyposis. Dis Colon Rectum 36:1059–1062
Vasen HF, Bulow S, Myrhoj T et al (1997) Decision analysis in the management of duodenal adenomatosis in familial adenomatous polyposis. Gut 40(6):716–719
Gallagher MC, Phillips RKS, Bulow S (2006) Surveillance and management of upper gastrointestinal disease in Familial Adenomatous Polyposis. Fam Cancer 5:263–273
Spigelman AD, Williams CB, Talbot IC et al (1989) Upper gastrointestinal cancer in patients with familial adenomatous polyposis. Lancet 2:783–785
Groves CJ, Saunders BP, Spigelman AD, Phillips RK (2002) Duodenal cancer in patients with familial adenomatous polyposis (FAP): results of a 10 year prospective study. Gut 50:636–641
Bulow S, Bjork J, Christensen IJ et al (2004) Duodenal adenomatosis in familial adenomatous polyposis. Gut 53:381–386
Nugent KP, Spigelman AD, Williams CB et al (1994) Surveillance of duodenal polyps in familial adenomatous polyposis: progress report. J R Soc Med 87(11):704–706
De Castro SMM, van Eijck CHJ, Rutten JP et al (2008) Pancreas-preserving total duodenectomy versus standard pancreatoduodenectomy for patients with familial adenomatous polyposis and polyps in the duodenum. Br J Surg 95:1380–1386
Brosens LAA, Keller JJ, Offerhaus GJA et al (2005) Prevention and management of duodenal polyps in familial adenomatous polyposis. Gut 54:1034–1043
Phillips RKS, Wallace M, Lynch P et al (2002) A randomised double-blind placebo-controlled study of celecoxib, a selective cyclooxygenase-2 inhibitor, on duodenal polyposis in familial adenomatous polyposis. Gut 50:857–860
Bulow S, Christensen J, Helle H et al. (2011) Duodenal surveillance improves the prognosis after duodenal cancer in familial adenomatous polyposis. Colorectal Dis, doi:10.1111/j.1463-1318.2011.02844.x [Epub ahead of print]
Acknowledgments
The authors would like to thank Kay Neale and the staff of the St Mark’s Hospital Polyposis Registry.
Conflict of interest
The authors state that there are no conflicting interests to declare.
Ethical Statement
Ethical approval was not required as anonymised data was obtained retrospectively from a database of our own patients.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Balmforth, D.C., Phillips, R.K.S. & Clark, S.K. Advanced duodenal disease in familial adenomatous polyposis: how frequently should patients be followed up after successful therapy?. Familial Cancer 11, 553–557 (2012). https://doi.org/10.1007/s10689-012-9546-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10689-012-9546-2