
Abstract
Background and Aims
Endoscopic biliary sphincterotomy (EST) is commonly performed during therapeutic endoscopic retrograde cholangiopancreatography (ERCP), but is an independent risk factor for post-ERCP pancreatitis, bleeding and duodenal perforation. These are partly ascribed to the electrosurgical current mode used for EST, and currently the optimal current model for EST remains controversial. In this study, we aimed to compare the rate of complications undergoing EST using the Endocut versus the blended current.
Methods
A systematic search of databases was performed for relevant published and prospective studies including randomized clinical trials (RCTs) to compare Endocut with blended current modes for EST. Data were collected from inception until 1 July 2018, using post-ERCP pancreatitis, bleeding and perforation as primary outcomes.
Results
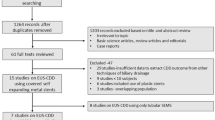
Three RCTs including a total of 594 patients met the inclusion criteria. Our meta-analysis results showed the rate of post-ERCP pancreatitis, primarily mild to moderate pancreatitis, was no different between Endocut versus blended current modes [risk ratio (RR) 0.61, 95% confidence interval (CI) 0.25–1.52, P = 0.29]. However, the risk of endoscopically bleeding events, primarily mild bleeding, was lower in studies using Endocut versus blended current (RR 0.54, 95% CI 0.31–0.95, P = 0.03). Notably, none of the patients experienced perforation in these three trials.
Conclusions
The rate of post-ERCP pancreatitis was not significantly different when using the Endocut versus blended current during EST. Nevertheless, compared with the blended current, Endocut reduced the incidence of endoscopically evident bleeding; however, the available data were insufficient to assess the perforation risk.




Similar content being viewed by others


Abbreviations
- EST:
-
Endoscopic biliary sphincterotomy
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
- RR:
-
Risk ratio
- CI:
-
Confidence interval
- RCTs:
-
Randomized clinical trials
References
Freeman ML, Nelson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–918. https://doi.org/10.1056/nejm199609263351301.
Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001;54:425–434. Epub 2001/09/29 PubMed PMID: 11577302.
Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454. https://doi.org/10.1016/j.gie.2009.10.027.
Donnellan F, Byrne MF. Prevention of post-ERCP pancreatitis. Gastroenterol Res Pract. 2012;2012:796751. https://doi.org/10.1155/2012/796751.
Arata S, Takada T, Hirata K, et al. Post-ERCP pancreatitis. J Hepatobiliary Pancreat Sci. 2010;17:70–78. https://doi.org/10.1007/s00534-009-0220-5.
Masci E, Mariani A, Curioni S, Testoni PA. Risk factors for pancreatitis following endoscopic retrograde cholangiopancreatography: a meta-analysis. Endoscopy. 2003;35:830–834. https://doi.org/10.1055/s-2003-42614.
Stefanidis G, Karamanolis G, Viazis N, et al. A comparative study of postendoscopic sphincterotomy complications with various types of electrosurgical current in patients with choledocholithiasis. Gastrointest Endosc. 2003;57:192–197. https://doi.org/10.1067/mge.2003.61.
Gottlieb K, Sherman S. ERCP and biliary endoscopic sphincterotomy-induced pancreatitis. Gastrointest Endosc Clin N Am. 1998;8:87–114. Epub 1998/02/14 PubMed PMID: 9405753.
Sherman S. ERCP and endoscopic sphincterotomy-induced pancreatitis. Am J Gastroenterol. 1994;89:303–305.
Morris ML, Tucker RD, Baron TH, Song LM. Electrosurgery in gastrointestinal endoscopy: principles to practice. Am J Gastroenterol. 2009;104:1563–1574. https://doi.org/10.1038/ajg.2009.105.
Gorelick A, Cannon M, Barnett J, Chey W, Scheiman J, Elta G. First cut, then blend: an electrocautery technique affecting bleeding at sphincterotomy. Endoscopy. 2001;33:976–980. https://doi.org/10.1055/s-2001-17918.
Elta GH, Barnett JL, Wille RT, Brown KA, Chey WD, Scheiman JM. Pure cut electrocautery current for sphincterotomy causes less post-procedure pancreatitis than blended current. Gastrointest Endosc. 1998;47:149–153.
Slivka A, Bosco JJ, Barkun AN, et al. Electrosurgical generators: May 2003. Gastrointest Endosc. 2003;58:656–660.
Macintosh DG, Love J, Abraham NS. Endoscopic sphincterotomy by using pure-cut electrosurgical current and the risk of post-ERCP pancreatitis: a prospective randomized trial. Gastrointest Endosc. 2004;60:551–556.
Norton ID, Petersen BT, Bosco J, et al. A randomized trial of endoscopic biliary sphincterotomy using pure-cut versus combined cut and coagulation waveforms. Clin Gastroenterol Hepatol. 2005;3:1029–1033.
Lee SJ, Song KS, Chung JP, et al. Type of electric currents used for standard endoscopic sphincterotomy does not determine the type of complications. Korean J Gastroenterol. 2004;43:204–210.
Verma D, Kapadia A, Adler DG. Pure versus mixed electrosurgical current for endoscopic biliary sphincterotomy: a meta-analysis of adverse outcomes. Gastrointest Endosc. 2007;66:283–290. https://doi.org/10.1016/j.gie.2007.01.018.
Testoni PA, Mariani A, Aabakken L, et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016;48:657–683. https://doi.org/10.1055/s-0042-108641.
Kohler A, Maier M, Benz C, Martin WR, Farin G, Riemann JF. A new HF current generator with automatically controlled system (Endocut mode) for endoscopic sphincterotomy–preliminary experience. Endoscopy. 1998;30:351–355. https://doi.org/10.1055/s-2007-1001281.
Perini RF, Sadurski R, Cotton PB, Patel RS, Hawes RH, Cunningham JT. Post-sphincterotomy bleeding after the introduction of microprocessor-controlled electrosurgery: Does the new technology make the difference? Gastrointest Endosc. 2005;61:53–57.
Akiho H, Sumida Y, Akahoshi K, et al. Safety advantage of endocut mode over endoscopic sphincterotomy for choledocholithiasis. World J Gastroenterol. 2006;12:2086–2088.
Tanaka Y, Sato K, Tsuchida H, et al. A prospective randomized controlled study of endoscopic sphincterotomy with the Endocut mode or conventional blended cut mode. J Clin Gastroenterol. 2015;49:127–131. https://doi.org/10.1097/mcg.0000000000000096.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151:W65–W94. Epub 2009/07/23 PubMed PMID: 19622512.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials. 1996;17:1–12. Epub 1996/02/01 PubMed PMID: 8721797.
Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393. Epub 1991/05/01 PubMed PMID: 2070995.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. https://doi.org/10.1136/bmj.327.7414.557.
Kida M, Kikuchi H, Araki M, et al. Randomized control trial of EST with either endocut mode or conventional pure cut mode. Gastrointest Endosc. 2004;59:201 Abstract.
Giuffrida MA. Type II error and statistical power in reports of small animal clinical trials. J Am Vet Med Assoc. 2014;244:1075–1080. https://doi.org/10.2460/javma.244.9.1075.
Acknowledgments
This work was supported by the Natural Science Foundation of Hunan Province (no. 2017JJ3270), Natural Science Foundation of Guangdong Province (no. 2018A0303100024), Three Engineering Training Funds in Shenzhen (nos. SYLY201718 and SYLY201801) Technical Research and Development Project of Shenzhen (no. JCYJ20150403101028164), National Key R&D Program of China (nos. 2017YFC1308800 and 2018YFC1313103) and National Natural Science Foundation of China (nos. 81670473 and 81873546).
Author information
Authors and Affiliations
Contributions
LW, ZL, YY, YB were responsible for design of the study and reviewed the manuscript. DL, MY, XC, XF, SW drafted the manuscript. NW, FT, HX, JW, SW, ZY, CW, FX, TL, ML were responsible for screening the literature. DL, MY, XC, NW, FT, HX abstracted data and did statistical analysis. WF was responsible for revising the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Li-sheng Wang, Zhao-shen Li, Jun Yao and Yu Bai share co-corresponding authorship.
Rights and permissions
About this article

Cite this article
Li, Df., Yang, Mf., Chang, X. et al. Endocut Versus Conventional Blended Electrosurgical Current for Endoscopic Biliary Sphincterotomy: A Meta-Analysis of Complications. Dig Dis Sci 64, 2088–2094 (2019). https://doi.org/10.1007/s10620-019-05513-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05513-w