
Abstract
Background and Aim
The purpose of this study was to determine (1) the diagnostic yield for endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) in patients with pancreatic cystic lesions, (2) additional value of EUS-FNA over EUS alone in the diagnosis of pancreatic cysts, and (3) diagnostic sensitivity and specificity of EUS and EUS-FNA in the subset of patients where histopathology of surgical specimens were available.
Methods
All patients who underwent EUS examination for the evaluation of pancreatic cystic lesions in six Asian centres were included in the study.
Results
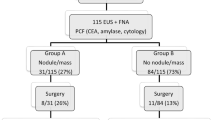
Of 298 patients with pancreatic cysts who underwent EUS, 132 (44.3 %) underwent FNA. In the entire cohort, pseudocysts and intraductal papillary mucinous neoplasm (IPMN) were the predominant cystic lesions. The cytologic yield of EUS-FNA was 47 %. On univariate analysis, factors associated with higher cytologic yield included vascular involvement on EUS, presence of solid cystic component, and increased number of needle passes during EUS-FNA. On multivariate analysis, presence of solid cystic components and increased number of needle passes during EUS-FNA were associated with higher diagnostic yield of EUS-FNA. For pancreatic cysts with a solid component, the diagnostic yield of EUS-FNA increased significantly from 44 % with one pass to 78 % with more than one pass (p = 0.016). In the absence of a solid component, the diagnostic yield was 29 % with one pass and was not significantly different from the diagnostic yield of 50 % with more than one pass, p = 0.081.
Conclusion
The cytologic yield of EUS-FNA was 47 %. When a solid component was present in the cyst, doing more than one pass during EUS-FNA increased its diagnostic yield.


Similar content being viewed by others


References
de Jong K, Poley JW, van Hooft JE, Visser M, Bruno MJ, Fockens P. Endoscopic ultrasound-guided fine-needle aspiration of pancreatic cystic lesions provides inadequate material for cytology and laboratory analysis: initial results from a prospective study. Endoscopy. 2011;43:585–590.
Frossard JL, Amouyal P, Amouyal G, et al. Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions. Am J Gastroenterol. 2003;98:1516–1524.
Lim LG, Itoi T, Lim WC, et al. Current status on the diagnosis and management of pancreatic cysts in the Asia-Pacific region: the role of endoscopic ultrasound. J Gastroenterol Hepatol. 2011;26:1702–1708.
Williams DB, Sahai AV, Aabakken L, et al. Endoscopic ultrasound guided fine needle aspiration biopsy: a large single centre experience. Gut. 1999;44:720–726.
Varadarajulu S, Eloubeidi MA. Frequency and significance of acute intracystic hemorrhage during EUS-FNA of cystic lesions of the pancreas. Gastrointest Endosc. 2004;60:631–635.
O’Toole D, Palazzo L, Arotçarena R, et al. Assessment of complications of EUS-guided fine-needle aspiration. Gastrointest Endosc. 2001;53:470–474.
Al-Haddad M, Wallace MB, Woodward TA, et al. The safety of fine-needle aspiration guided by endoscopic ultrasound: a prospective study. Endoscopy. 2008;40:204–208.
Hirooka Y, Goto H, Itoh A, et al. Case of intraductal papillary mucinous tumor in which endosconography-guided fine-needle aspiration biopsy caused dissemination. J Gastroenterol Hepatol. 2003;18:1323–1324.
Lee JH, Stewart J, Ross WA, et al. Blinded prospective comparison of the performance of 22-gauge and 25-gauge needles in endoscopic ultrasound-guided fine needle aspiration of the pancreas and peri-pancreatic lesions. Dig Dis Sci. 2009;54:2274–2281.
Sahai AV, Chua TS, Paquin S, Gariepy G. Analysis of variables associated with surgery versus observation in patients with pancreatic cystic lesions referred for endoscopic ultrasound. Endoscopy. 2011;43:591–595.
Conflict of interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Lim, L.G., Lakhtakia, S., Ang, T.L. et al. Factors Determining Diagnostic Yield of Endoscopic Ultrasound Guided Fine-Needle Aspiration for Pancreatic Cystic Lesions: A Multicentre Asian Study. Dig Dis Sci 58, 1751–1757 (2013). https://doi.org/10.1007/s10620-012-2528-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-012-2528-2