
Abstract
Background
Obesity is a risk factor for colorectal cancer, and colonoscopy can be technically challenging in obese patients. It has been proposed (with little supporting data) that prone positioning of obese patients might facilitate a difficult colonoscopy.
Aim
The aim of this study was to determine if starting colonoscopy in the prone position for obese patients decreases cecal intubation times.
Methods
This was a prospective, randomized study conducted at the North Texas VA Medical Center. Patients with a body mass index of ≥30 kg/m2 undergoing elective colonoscopy were randomized 1:1 to either initial prone positioning or standard, left-lateral positioning. The outcome measurements were cecal intubation time, frequency of repositioning, sedative medications used, reports of pain, complications, and procedure tolerability.
Results
Fifty patients were randomized to have colonoscopy starting in the standard, left-lateral decubitus position, and 51 to the prone position. The average cecal intubation time for the standard group was 550 vs. 424 s in the prone group (p = 0.03). Patient repositioning was used in 28 % of patients in the standard group versus 8 % in the prone group (p = 0.009). There was no difference in subjective reports of pain between groups (p = 0.95) or in average pain scores (p = 0.79). Follow-up interviews were conducted in 93 % of patients, all of whom said that they would be willing to have repeat colonoscopy in the same position.
Conclusions
Performance of colonoscopy in the prone position for obese patients results in significantly shorter cecal intubation times and decreased need for patient repositioning. Prone positioning is well accepted and does not significantly increase procedure-related discomfort.
Similar content being viewed by others


Introduction
Obesity is a risk factor for colorectal cancer, and it has been estimated that more than one-third of adult Americans are obese [1]. Compared to individuals of normal weight, those with a body mass index (BMI) ≥30 kg/m2 have almost a 20 % greater risk of developing colorectal cancer [2]. A central pattern of obesity, with excess abdominal adiposity, is an especially strong risk factor for this tumor [3].
In the United States, colonoscopy is being used with increasing frequency in an effort to prevent morbidity and mortality from colorectal cancer [4]. Colonoscopy can be especially challenging in obese patients [5]. For example, obese patients are more likely than normal weight patients to have an inadequate bowel preparation [6]. In addition, patient repositioning often is performed during colonoscopy to facilitate the advancement of the endoscope, and it can be difficult for the endoscopist and support staff to reposition an obese patient who is sedated.
In obese patients, it has been proposed that a change to the prone position might facilitate a difficult colonoscopy [7–9]. However, there is little supporting data, with only one retrospective study reported in abstract form. This study found that for obese patients, colonoscopies started in the prone position were associated with more rapid cecal intubation times than colonoscopies started in the conventional position [10]. In our own practices, furthermore, we had noted that repositioning obese patients into the prone position during colonoscopy could be difficult, but that it often seemed to facilitate the procedure. Therefore, we hypothesized that starting colonoscopy for obese patients in the prone position would reduce cecal intubation times, and we performed a prospective, randomized trial to test that hypothesis.
Methods
Setting and Patients
All procedures were performed at the Dallas VA Medical Center by experienced staff endoscopists (W.V.H., K.B.D., B.L.C., S.J.S., L.A.F.) or a senior gastroenterology fellow (F.S.U.) who had performed more than 200 colonoscopies. The study was approved by the Institutional Review Board of the Dallas VA Medical Center in December 2010. The study was registered on ClincialTrials.gov, number NCT01616602.
The prospective, randomized trial was conducted from January 2011 to February 2012. All eligible patients with BMI ≥ 30 kg/m2 presenting for elective colonoscopy were invited to participate. Exclusion criteria included a history of colonic resection, colonic strictures, inadequate bowel preparation, and colonic or intra-abdominal malignancy. Patients scheduled to receive deep sedation with propofol or general anesthesia also were excluded.
Study Design
For patients who provided informed consent, we recorded data on age, gender, BMI, measurement of waist circumference, indication for colonoscopy, history of prior colonoscopy, history of abdominal surgery, and comorbid conditions (chronic obstructive pulmonary disease, obstructive sleep apnea, coronary artery disease, congestive heart failure, cirrhosis, presence of ascites, history of back or neck problems, and use of CPAP or BiPAP). Patients were randomized in a 1:1 ratio to one of two starting positions, i.e. the standard left lateral decubitus position or prone position. The randomization schedule was computer-generated and allocation concealment was performed using sequentially numbered, sealed envelopes with the position assignment that was opened at the time of randomization.
All patients received standard bowel preparation with 4-liter polyethylene glycol electrolyte solution. Both standard adult and pediatric Olympus high-definition colonoscopies, all with variable stiffness, were used at the discretion of the endoscopist. Intravenous sedation was administered in standard fashion, also at the discretion of the endoscopist; a combination of midazolam with either meperidine or fentanyl was used in most cases. During the insertion portion of the colonoscopy, the patient’s starting position was changed only if the endoscopist encountered difficulty in advancing the endoscope that, in the endoscopist’s opinion, would be facilitated by a position change.
We recorded the time when the colonoscope was inserted in the rectum and the time when the appendiceal orifice was identified. Cecal intubation time, the primary outcome variable, was defined as the difference between these two time points. We also recorded medications and doses used for sedation, patient reports of pain (as assessed using a scale from 0 to 10, with 10 being the greatest level of pain), quality of bowel preparation as determined by the individual endoscopist, the presence of diverticular disease, and the use of any ancillary maneuvers ordered by the endoscopist to complete the examination, including position change.
Follow-up interviews were conducted by telephone 3 days after the colonoscopy. Information gathered included the patient’s recollection of pain or discomfort during the procedure. Additionally, patients were asked if they had experienced any other post-procedure complications including bleeding and ongoing pain. Finally, patients were asked if they would be willing to undergo a repeat colonoscopy in the same starting position if needed in the future.
Statistical Analysis
Analyses were performed on a per-protocol basis using the Mann–Whitney U test for continuous variables (as the data were not normally distributed) and the Fisher’s exact test for categorical variables. A p value of 0.05 was considered statistically significant.
Due to the unavailability of published reports on the utility of prone positioning for obese patients, a formal power calculation could not be performed. Instead, we designed this trial as a pilot study, and planned to enroll 100 patients.
All authors had access to the study data and reviewed and approved the final manuscript. Statistical analysis was performed using Graph Pad Instat3.
Results
Patient Characteristics
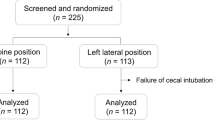
During the study, we screened 1,812 patients who were scheduled for elective colonoscopy. Of these, 1,707 were not obese (BMI < 30), had prior colonic resections, met other exclusion criteria, or declined to participate. We enrolled 105 study patients; 51 were randomized to undergo colonoscopy in the standard, left-sided position, and 54 were randomized to undergo colonoscopy in the prone position. Four patients were excluded because of incomplete data collection (1 each from the standard group and the prone group) or because of inadequate bowel preparation that precluded complete colonoscopy (2 from the prone group). We ultimately had 50 patients who underwent colonoscopy in the standard position and 51 patients in the prone group (see Fig. 1).

Flow chart of patient enrollment
Demographic data are summarized in Table 1. All patients were men. There were no significant differences between the randomization groups in age, ethnicity, indications for colonoscopy, frequency of prior colonoscopy, frequency of abdominal surgery or frequency of comorbid conditions. In addition, the groups did not differ significantly in mean BMI and waist circumference, or in the frequency of diverticular disease and adequacy of bowel preparation.
Average Cecal Intubation Times Were Shorter for the Prone Position
The cecal intubation rate in both groups was 100 %. The average cecal intubation time in the standard group was 550 s (approximately 9 min), compared to 420 s (7 min) in the prone group (p = 0.03) (see Table 2).
Patients Starting in the Prone Position Required Less Frequent Repositioning
During colonoscopy in the standard group, 14 patients (28 %) were repositioned, with five ultimately having their examination completed in the prone position. During colonoscopy in the prone group, only four patients (8 %) were repositioned. The relative risk (RR) of repositioning was significantly higher in the standard group with a RR of 1.79 (95 % CI 1.23–2.54, p = 0.009) (see Table 2).
No Differences in Medications Needed for Sedation or Reports of Pain Between Patients in the Prone and Standard Positions
As shown in Table 2, there were no significant differences between the groups in the use of sedatives or in the mean doses of sedative medications used during colonoscopy. In addition, there were no significant differences between the two groups in the number of patients who reported pain during their procedure (56 % in the standard group versus 59 % in the prone group, p = 0.95, RR = 0.95, 95 % CI 0.63–1.43) or in the average pain score reported per patient (3.7 in the standard group vs. 3.8 in the prone group, p = 0.79) (see Table 2).
Prone Positioning Was Well Accepted by Patients
A follow-up telephone interview was conducted in 93 (92 %) patients, specifically, 46 of 50 in the standard group and 47 of 51 in the prone group. No patient reported pain after the procedure. There was 1 complication—a post-polypectomy bleed in a patient in the prone group. All patients said that they would agree to have repeat colonoscopy in the same position if one were needed in the future. When patients who had been repositioned from their designated starting position were asked if they had preference for either their starting or ending position, 16 of 18 (89 %) expressed that they had no preference. However, of the five patients who started in the standard position and were repositioned to complete their examination in the prone position, two expressed a preference for the prone position.
Discussion
Although more than one-third of adult Americans are obese, and obesity is a colorectal cancer risk factor that can adversely influence the performance of colonoscopy, few studies have focused on techniques that might facilitate colonoscopy for obese patients. In this prospective randomized trial, we have found that starting colonoscopy in the prone position rather than in the standard left lateral decubitus position results in significantly shorter cecal intubation times (420 vs. 550 s, p = 0.03) and significantly reduces the frequency of patient repositioning during the procedure (8 vs. 28 %, p = 0.009). In addition, initial prone positioning in our study was not associated with any significant difference in the use or dosages of sedative medications, or in the frequency of pain reported during colonoscopy. Furthermore, we found that prone positioning was well accepted by obese patients.
Obesity is associated with a number of factors that make colonoscopy technically challenging. Compared to normal weight patients, obese patients are more likely to have inadequate bowel preparations, which are known to prolong the time and reduce the quality of colonoscopy [6]. When colonoscope loop formation occurs, it can be difficult to appreciate the location of the loop in an obese abdomen and, therefore, to determine where to apply pressure that might facilitate passage of the endoscope. When the application of manual pressure fails, colonoscopists often change the patient’s position [8]. Such a position change can be difficult for the obese patient and, if the patient is more than lightly sedated, position changing often requires some patient lifting by the endoscopist or assistant that might be physically demanding and potentially hazardous.
It is not clear why prone positioning facilitates the performance of colonoscopy in obese patients. One study that used fluoroscopy to document the orientation of the colonoscope found that prone positioning straightened that orientation and facilitated intubation of the terminal ileum [11]. This study focused on ileal (not cecal) intubation, however, and the report provides no information on the BMI of study participants. Therefore, it is not clear that prone position-induced colonoscope straightening is what reduces the time for cecal intubation in obese subjects. Although our study did not explore the mechanism underlying the beneficial effect of prone positioning, we speculate that prone positioning in the obese results in a redistribution of abdominal pressure that prevents loop formation.
Our study has the major strengths of being prospective and randomized, but it has some limitations as well. Our study population comprised only male veteran patients, and this limits the generalizability of the results to women. Female gender has been identified as a factor that contributes to difficult colonoscopy and prolonged cecal intubation time [12]. From our study, it is not clear whether initial prone positioning will reduce cecal intubation time in obese women. Our study involved a number of different endoscopists and endoscopy assistants with varying levels of experience, and we did not mandate the use of any one colonoscope for study purposes, as this is more representative of real-life colonoscopy. However, all endoscopists felt it was technically easy to perform colonoscopy with obese patients in the prone position. Thus, it is not clear how these factors might have influenced our study results.
In addition, the results of our study apply to obese patients undergoing colonoscopy with light to moderate conscious sedation. We chose to exclude patients who were scheduled for colonoscopy with deep sedation (propofol) or general anesthesia. Obese patients are at increased risk for sleep apnea, and patients with sleep apnea have an increased risk for cardiovascular complications during sedation [13, 14]. In one study of 397 patients undergoing average-risk endoscopy, 35 % had BMI > 30 kg/m2, 82 % of whom were judged to be at increased risk for sleep apnea. These high-risk patients were found to be more likely to have oxygen desaturations and hypercapneic episodes during sedation [5]. In our study, we used only light to moderate sedation, and a gastroenterology nurse continually monitored the patient’s vital signs including oxygen saturation and comfort. Our study did include 18 patients with known obstructive sleep apnea, seven of whom underwent colonoscopy in the prone position, with no complications.
We did not have any sedation related complications in our study, nor did we have any complications with respect to airway management. Nevertheless, apnea and sedation-related complications are serious complications that occur with increased frequency in obese patients. If sedation were to result in the need to administer cardiopulmonary resuscitation to an obese patient, then a prone position might interfere with that resuscitation. Prone positioning probably should not be used in a patient who needs deep sedation or who is at high risk for cardiopulmonary complications of sedation.
We conclude that in patients with BMI > 30 kg/m2, the performance of colonoscopy starting in the prone position results in significantly shorter cecal intubation times and decreased need for patient repositioning. Prone positioning is well accepted by patients and does not significantly increase procedure-related discomfort. For obese patients, consideration should be given to starting colonoscopy in the prone position.
References
Ogden CL, Carroll ME, Kit BK, et al. Prevalence of obesity in the United States, 2009–2010. NCHS Data Brief. 2012;82:1–8.
Moghaddam AA, Woodward M, Huxley R. Obesity and risk of colorectal cancer: a meta-analysis of 31 studies with 70,000 events. Cancer Epidemiol Biomarkers Prev. 2007;16:2533–2547.
Haggar FA, Boushey RP. Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors. Clin Colon Rectal Surg. 2009;22:191–197.
Phillips KA, Liang SY, Ladabaum U, et al. Trends in colonoscopy for colorectal cancer screening. Med Care. 2007;45:160–167.
Schreiner MA, Fennerty MB. Endoscopy in the obese patient. Gastroenterol Clin N Am. 2010;39:87–97.
Borg BB, Gupta NK, Zukerman GR, et al. Impact of obesity on bowel preparation for colonoscopy. Clin Gastroenterol Hepatol. 2009;7:670–675.
Hansel SL, Prechel JA, Horn B, et al. Observational study of the frequency of use and perceived usefulness of ancillary maneuvers to facilitate colonoscopy completion. Dig Liv Dis. 2009;41:812–816.
Roberts-Thomson IC, Teo E. Colonoscopy: art or science? J Gastroenterol Hepatol. 2009;24:180–184.
Waye JD, Yessayan SA, Lewis BS, et al. The technique of abdominal pressure in total colonoscopy. Gastrointest Endosc. 1991;37:147–151.
Desormeaux M, Scicluna M, Friedland S. Colonoscopy in obese patients: a growing problem. Gastrointest Endosc. 2008;67:AB89.
De Silva AP, Kumarasena RS, Perera Keragala SD, et al. The prone 12 o’clock position reduces ileal intubation time during colonoscopy compared to the left lateral 6 o’clock (standard) position. BMC Gastroenterol. 2011;11:89.
Chutkan R. Colonoscopy issues related to women. Gastrointest Endoscopy Clin N Am. 2006;16:153–163.
Tishler PV, Larkin EK, Schluchter MD, et al. Incidence of sleep-disordered breathing in an urban adult population. JAMA. 2003;289:2230–2237.
Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg. 2008;107:1543–1563.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Uddin, F.S., Iqbal, R., Harford, W.V. et al. Prone Positioning of Obese Patients for Colonoscopy Results in Shortened Cecal Intubation Times: A Randomized Trial. Dig Dis Sci 58, 782–787 (2013). https://doi.org/10.1007/s10620-012-2468-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-012-2468-x