
Abstract
Diabetes mellitus has been associated with changes in the structure and function of the myocardium manifesting in the early stages of the disease as subtle systolic and diastolic dysfunction; the role of dobutamine stress echocardiography (DSE) in this setting remains unclear. We sought to evaluate the prevalence of dobutamine-induced systolic dysfunction amongst diabetic patients with normal at rest left ventricular ejection fraction and no coronary artery disease and to investigate whether an optimized therapeutic approach can reverse these abnormalities. 1,363 patients with DM referred to our echocardiography laboratory for DSE between January 2008 and June 2010 were prospectively investigated. Patients with normal left ventricular ejection fraction (LVEF) at rest and significant deterioration during peak dobutamine infusion (defined as a ≥10% decrease) in the absence of coronary artery disease or vasospasm were enrolled. They received on top of their usual treatment 5 mg perindopril and had their glycemic control intensified. At 60 days, all of them were controlled for clinical status and underwent a control DSE. 18 patients were included, there were 9 males and 9 females, mean age was 66.1 ± 10.2 years. All the patients had type II DM with a mean duration of 12.7 ± 6.6 years. They all had normal at rest echocardiographic findings with no wall motion abnormalities; mean LVEF was 62 ± 6%. At peak dobutamine, LVEF significantly deteriorated in all the patients with a mean 15 ± 5% decrease compared to baseline. After therapeutic optimization, Glycated haemoglobin improved from 8.53 ± 2.05% to 6.8 ± 0.6% (δ HbA1C = 1.73%, P = 0.001), mean LVEF at peak dobutamine infusion evolved from 47.17 ± 4.2% pre-optimization to 58 ± 4.8% at control (10.83% improvement; P < 0.001). In patients with DM and normal at rest LVEF, Dobutamine infusion during DSE can induce a significant deterioration in LVEF in the absence of coronary artery disease or vasospasm. This specific condition could be largely reversed through an optimized therapy based on a tighter metabolic control and a more stringent renin-angiotensin-aldosterone system inhibition.



Similar content being viewed by others

References
King H, Aubert RE, Herman WH (1998) Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care 21:1414–1431
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR (2000) Association of glycemia with macrovascular and microvascular complications of type 2 diabetes (United Kingdom Prospective Diabetes Study 35): prospective observational study. BMJ 321:405–412
Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, Gardin JM, Rutledge JE, Boineau RC (2000) Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol 35:1628–1637
Avogaro A, Nosadini R, Doria A, Fioretto P, Velussi M, Vigorito C, Saccà L, Toffolo G, Cobelli C, Trevisan R (1990) Myocardial metabolism in insulin deficient diabetic humans without coronary artery disease. Am J Physiol 258:E606–E618
Rubler S, Dlugash J, Yuceoglu YZ, Kumral T, Branwood AW, Grishman A (1972) New type of cardiomyopathy associated with diabetic glomerulosclerosis. Am J Cardiol 30:595–602
Aneja A, Tang WH, Bansilal S, Garcia MJ, Farkouh ME (2008) Diabetic cardiomyopathy: insights into pathogenesis, diagnostic challenges, and therapeutic options. Am J Med 121(9):748–757
Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I (1989) Recommendations for quantification of the left ventricle by two-dimensional echocardiography: American Society of Echocardiography Committee on Standards, Subcommittee on Quantification of Two- Dimensional Echocardiograms. J Am Soc Echocardiogr 2:358–367
Poldermans D, Fioretti PM, Boersma E, Bax JJ, Thomson IR, Roelandt JR, Simoons ML (1999) Long-term prognostic value of dobutamine–atropine stress echocardiography in 1,737 patients with known or suspected coronary artery disease: a single-center experience. Circulation; 99:757–762
Aboukhoudir F, Rekik S, Andrieu S, Cheggour S, Pansieri M, Metge M, Barnay P, Faugier JP, Schouvey S, Quaino G, Unal C, Gonzalez S, Hirsch JL (2009) Coronary artery spasm and dobutamine stress echocardiography. Eur J Echocardiogr 10(4):556–561
Boudina S, Abel ED (2010) Diabetic cardiomyopathy, causes and effects. Rev Endocr Metab Disord 11(1):31–39
Boyer JK, Thanigaraj S, Schechtman KB, Perez JE (2004) Prevalence of ventricular diastolic dysfunction in asymptomatic, normotensive diabetic mellitus. Am J Cardiol 93:870–875
Andersen NH, Poulsen SH, Eiskjaer H, Poulsen PL, Mogensen CE (2003) Decreased left ventricular longitudinal contraction in normotensive and normoalbuminuric patients with type II diabetes mellitus: a Doppler tissue tracking and strain rate echocardiography study. Clin Sci (Lond) 105:59–66
Fang ZY, Schull-Meade R, Leano R, Mottram PM, Prins JB, Marwick TH (2005) Screening for heart disease in diabetic subjects. Am Heart J 149(2):349–354
Palmieri V, Capaldo B, Russo C, Iaccarino M, Pezzullo S, Quintavalle G, Di Minno G, Riccardi G, Celentano A (2008) Uncomplicated type 1 diabetes and preclinical left ventricular myocardial dysfunction: Insights from echocardiography and exercise cardiac performance evaluation. Diabetes Res Clin Pract 79(2):262–268
Ha JW, Lee HC, Kang ES, Ahn CM, Kim JM, Ahn JA, Lee SW, Choi EY, Rim SJ, Oh JK, Chung N (2007) Abnormal left ventricular longitudinal functional reserve in patients with diabetes mellitus: implication for detecting subclinical myocardial dysfunction using exercise tissue Doppler echocardiography. Heart 93:1571–1576
Fang ZY, Najos-Valencia O, Leano R, Marwick TH (2003) Patients with early diabetic heart disease demonstrate a normal myocardial response to dobutamine. J Am Coll Cardiol 42:446–453
Scognamiglio R, Avogaro A, Casara D, Crepaldi C, Marin M, Palisi M, Mingardi R, Erle G, Fasoli G, Dalla Volta S (1998) Myocardial dysfunction and adrenergic cardiac innervation in patients with insulin-dependent diabetes mellitus. J Am Coll Cardiol 31:404–412
Von Bibra H, Thrainsdottir IS, Hansen A et al (2005) Tissue Doppler imaging for the detection and quantitation of myocardial dysfunction in patients with type 2 diabetes mellitus. Diab Vasc Dis Res 2:24–30
Von Bibra H, Hansen A, Dounis V, Bystedt T, Malmberg K, Rydén L (2004) Augmented metabolic control improves myocardial diastolic function and perfusion in patients with non-insulin dependent diabetes. Heart 90:1483–1484
Konduracka E, Gackowski A, Rostoff P, Galicka-Latala D, Frasik W, Piwowarska W (2007) Diabetes-specific cardiomyopathy in type 1 diabetes mellitus: no evidence for its occurrence in the era of intensive insulin therapy. Eur Heart J 28:2465–2471
Zaman AK, Fujii S, Goto D, Furumoto T, Mishima T, Nakai Y, Dong J, Imagawa S, Sobel BE, Kitabatake A (2004) Salutary effects of attenuation of angiotensin II on coronary perivascular fibrosis associated with insulin resistance and obesity. J Mol Cell Cardiol 37:525–535
Kawasaki D, Kosugi K, Waki H, Yamamoto K, Tsujino T, Masuyama T (2007) Role of activated renin angiotensin system in myocardial fibrosis and left ventricular diastolic dysfunction in diabetic patients-reversal by chronic angiotensin II type 1A receptor blockade. Circ J 71:524–529
Patel A, ADVANCE Collaborative Group, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, Harrap S, Poulter N, Marre M, Cooper M, Glasziou P, Grobbee DE, Hamet P, Heller S, Liu LS, Mancia G, Mogensen CE, Pan CY, Rodgers A, Williams B (2007) Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 8(370):829–840
Conflict of interest
None to declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
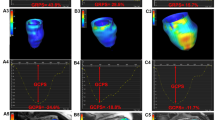
Movie 1: Echocardiographic loops recorded in the apical four-chamber views at rest and at low dose dobutamine infusion showing normal wall motion in all myocardial segments and normal left ventricular ejection fraction. At dobutamine-atropine peak stress, a global hypokinesia was observed with a marked deterioration in ejection fraction. (WMV 354 kb)
Movie 2: Echocardiographic loops recorded in the apical four-chamber views at rest and at low dose dobutamine infusion showing normal wall motion in all myocardial segments and normal left ventricular ejection fraction. An improved and adequate response was observed at dobutamine-atropine peak stress. (WMV 340 kb)
Rights and permissions
About this article
Cite this article
Aboukhoudir, F., Rekik, S. Left ventricular systolic function deterioration during dobutamine stress echocardiography as an early manifestation of diabetic cardiomyopathy and reversal by optimized therapeutic approach. Int J Cardiovasc Imaging 28, 1329–1339 (2012). https://doi.org/10.1007/s10554-011-9938-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-011-9938-7