
Abstract
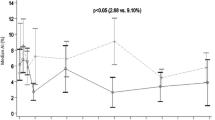
We compared the respiratory rate (RR) and transcutaneous carbon dioxide pressure (\({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\)) during intravenous sedation (IVS), to determine whether RR is a useful parameter for monitoring ventilation. This was a prospective cohort study. The study sample comprised dental patients who received IVS via propofol or midazolam administration at Nippon Dental University Hospital. We simultaneously measured RR (through capnography), \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\) (using the \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\) monitor), and percutaneous oxygen saturation (SpO2). RR was the predictor and the outcome variable was \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\). Data were analyzed by Dunnett’s test and Pearson’s correlation coefficient. P < 0.05 was considered statistically significant. The study sample consisted of 15 patients. No significant changes were identified in the RR and SpO2 measurements over time. However, \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\) values obtained from 20 to 40 min after induction of sedation were significantly higher than baseline values (P < 0.05). A correlation was found between RR and \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\) (P < 0.05), but the correlation coefficient was low (r = 0.22), indicating a weak correlation between these two factors. The results of this study suggest that RR is an inadequate parameter for monitoring ventilation during IVS; however, \({\text{Pt}}{{\text{c}}_{{\text{C}}{{\text{O}}_{\text{2}}}}}\) may be useful for monitoring.



Similar content being viewed by others


References
Fu ES, Downs JB, Schweiger JW, Miguel RV, Smith RA. Supplemental oxygen impairs detection of hypoventilation by pulse oximetry. Chest. 2004;126:1552–8.
McEvedy BAB, McLeod ME, Mulera M, Kirpalani H, Lerman J. End-tidal, transcutaneous, and arterial pCO2 measurements in critically ill neonates: a comparative study. Anesthesiology. 1988;69:112–6.
Abraham E, Smith M, Silver L. Continuous monitoring of critically ill patients with transcutaneous oxygen and carbon dioxide and conjunctival oxygen sensors. Ann Emerg Med. 1984;13:1021–6.
Bell JK, Laasch HU, Wilbraham L, England RE, Morris JA, Martin DF. Bispectral index monitoring for conscious sedation in intervention: better, safer, faster. Clin Radiol. 2004;59:1106–13.
Bower AL, Ripepi A, Dilger J, Boparai N, Brody FJ, Ponsky JL. Bispectral index monitoring of sedation during endoscopy. Gastrointest Endosc. 2000;52:192–6.
Chernik DA, Gillings D, Laine H, Hendler J, Silver JM, Davidson AB, Schwam EM, Siegel JL. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol. 1990;10:244–51.
Sandler NA, Hodges J, Sabino M. Assessment of recovery in patients undergoing intravenous conscious sedation using bispectral analysis. J Oral Maxillofac Surg. 2001; 59:603–11 (discussion 611-2).
Kwon MY, Lee SY, Kim TY, Kim DK, Lee KM, Woo NS, Chang YJ, Lee MA. Spectral entropy for assessing the depth of propofol sedation. Korean J Anesthesiol. 2012;62:234–9.
Bellman MH, Pleuvry BJ. Comparison of the respiratory effects of ICI 35 868 and thiopentone in the rabbit. Br J Anaesth. 1981;53:425–9.
Taylor MB, Grounds RM, Mulroony PD, Morgan M. Ventilatory effects of propofol during induction of anaesthesia. Anaesthesia. 1986;41:816–20.
Gautier H, Gaudy JH. Changes in ventilatory pattern induced by intravenous anesthetic agents in human subjects. J Appl Physiol. 1978;45:171–6.
Grounds RM, Maxwell DL, Talor MB, Aber V, Royston D. Acute ventilatory changes during i.v. induction of anaesthesia with thiopentone or propofol in man. Br J Anaesth. 1987;59:1098–102.
Milic-Emili J, Zin WA. Breathing responses to imposed mechanical loads (Handbook of physiology, the respiratory system II). Washington, DC: American Physiology Society; 1986. pp. 751–69.
Ponte J, Sadler CL. Effect of thiopentone, etomidate and propofol on carotid body chemoreceptor activity in the rabbit and the cat. Br J Anaesth. 1989;62:41–5.
Goodman NW, Black AMS, Carter JA. Some ventilatory effects of propofol as sole anaesthetic agent. Br J Anaesth. 1978;59:1497–503.
Zippi M, Traversa G, De Felici I, Febbraro I, Mattei E, Pietranico B, Sergio C, Sgarro MG, Occhigrossi G. Sedation with propofol in endoscopic retrograde cholangiopancreatography: personal experience. Clin Ther. 2008;159:19–22.
Keidan I, Gravenstein D, Berkenstadt H, Ziv A, Shavit I, Sidi A. Supplemental oxygen compromises the use of pulse oximetry for detection of apnea and hypoventilation during sedation in simulated pediatric patients. Pediatrics. 2008;122:293–8.
Ninomiya A, Matsuura N, Ichinohe T. Inhalation of 50% oxygen does not impair respiratory depression during midazolam sedation. J Oral Maxillofac Surg. 2016;74:1932–6.
Acknowledgements
We thank the research staff at the Department of Dental Anesthesiology, The Nippon Dental University School of Life Dentistry, Tokyo, for their support. We would like to thank Editage (http://www.editage.jp) for English language editing.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Morimoto, K., Ogura, S., Shinohara, K. et al. Respiratory rate is an inadequate parameter of ventilation in non-intubated sedation. Odontology 107, 219–222 (2019). https://doi.org/10.1007/s10266-018-0404-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-018-0404-z