
Abstract
Background
Nephrosclerosis is an increasingly reason for dialysis in Japan. However, kidney biopsy specimens for hypertensive nephrosclerosis are very limited; thus, the pathologic evaluation of hypertensive nephrosclerosis currently remains unclear.
Methods
Clinical and pathologic data of a total of 184 biopsy-confirmed hypertensive nephrosclerosis patients were collected from 13 centers throughout Japan. Seven pathological findings were assessed in this study. The outcomes of interest for this study were dialysis, composite kidney events, cardiovascular events, and all-cause mortality.
Results
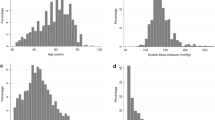
The Green and Yellow (G&Y), Orange, and Red groups of the chronic kidney diseases (CKD) heat map contained 36, 57, and 91 cases, respectively. The mean observation period was 7.3 ± 5.2 (median, IQR; 6.1, 2.6–9.7) years. Global glomerulosclerosis (GScle), interstitial fibrosis and tubular atrophy (IFTA), arteriolar hyalinosis in Red exhibited higher scores than those in G&Y and Orange. The incidence rates of the composite kidney end points in 100 person-years for the G&Y, Orange, and Red groups were 1.42, 2.16, and 3.98, respectively. In the univariate Cox analysis for the composite kidney end points, GScle, IFTA and interstitial cell infiltration exhibited statistically significant high hazard ratios (1.18, 1.84, 1.69, respectively). However, after adjustment for clinical and medication data, the Red group in the CKD heat map category was risk factor for the composite kidney end points (HR 9.51).
Conclusions
In summary, although pathologic findings had minor impacts on the prediction of composite outcomes in this study, the clinical stage of the CKD heat map is a good predictor of composite kidney events.


Similar content being viewed by others

References
Hanafusa N, Nakai S, Iseki K, et al. Japanese society for dialysis therapy renal data registry—a window through which we can view the details of Japanese dialysis population. Kidney Int Suppl. 2015;5(1):15–22.
Norris K, Bourgoigne J, Gassman J, et al. Cardiovascular outcomes in the African American Study of Kidney Disease and Hypertension (AASK) trial. Am J Kidney Dis. 2006;48(5):739–51.
Vikse BE, Aasarod K, Bostad L, et al. Clinical prognostic factors in biopsy-proven benign nephrosclerosis. Nephrol Dial Transplant. 2003;18(3):517–23.
Suzuki H, Kobayashi K, Ishida Y, et al. Patients with biopsy-proven nephrosclerosis and moderately impaired renal function have a higher risk for cardiovascular disease: 15 years’ experience in a single, kidney disease center. Ther Adv Cardiovasc Dis. 2015;9(3):77–86.
Takebayashi S, Kiyoshi Y, Hisano S, et al. Benign nephrosclerosis: incidence, morphology and prognosis. Clin Nephrol. 2001;55(5):349–56.
Dasgupta I, Porter C, Innes A, et al. “Benign” hypertensive nephrosclerosis. QJM. 2007;100(2):113–9.
Liang S, Le W, Liang D, et al. Clinico-pathological characteristics and outcomes of patients with biopsy-proven hypertensive nephrosclerosis: a retrospective cohort study. BMC Nephrol. 2016;17:42.
Levin A, Stevens PE. Summary of KDIGO 2012 CKD Guideline: behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014;85(1):49–61.
Akbari A, Clase CM, Acott P, et al. Canadian Society of Nephrology commentary on the KDIGO clinical practice guideline for CKD evaluation and management. Am J Kidney Dis. 2015;65(2):177–205.
Furuichi K, Yuzawa Y, Shimizu M, et al. Nationwide multicentre kidney biopsy study of Japanese patients with type 2 diabetes. Nephrol Dial Transplant. 2017. https://doi.org/10.1093/ndt/gfw417.
Matsuo S, Imai E, Horio M, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982–92.
Levey AS, de Jong PE, Coresh J, et al. The definition, classification, and prognosis of chronic kidney disease: a KDIGO Controversies Conference report. Kidney Int. 2011;80(1):17–28.
Norris KC, Greene T, Kopple J, et al. Baseline predictors of renal disease progression in the African American Study of Hypertension and Kidney Disease. J Am Soc Nephrol. 2006;17(10):2928–36.
Sumida K, Hoshino J, Ueno T, et al. Effect of proteinuria and glomerular filtration rate on renal outcome in patients with biopsy-proven benign nephrosclerosis. PLoS One. 2016;11(1):e0147690.
Fogo A, Breyer JA, Smith MC, et al. Accuracy of the diagnosis of hypertensive nephrosclerosis in African Americans: a report from the African American Study of Kidney Disease (AASK) Trial. AASK Pilot Study Investigators. Kidney Int. 1997;51(1):244–52.
Appel LJ, Wright JT Jr, Greene T, et al. Long-term effects of renin-angiotensin system-blocking therapy and a low blood pressure goal on progression of hypertensive chronic kidney disease in African Americans. Arch Intern Med. 2008;168(8):832–9.
Appel LJ, Wright JT Jr, Greene T, et al. Intensive blood-pressure control in hypertensive chronic kidney disease. N Engl J Med. 2010;363(10):918–29.
Acknowledgements
This study was supported in part by a Grant-in-Aid for Diabetic Nephropathy and Nephrosclerosis Research from the Ministry of Health, Labour and Welfare of Japan and Grant-in-Aid for Practical Research Project for Renal Diseases, from the Japan Agency for Medical Research and Development (No. 15ek0310003h0001). This work was also supported in part by Grants-in-Aids from the Ministry of Education, Culture, Sports, Science, and Technology of the Japanese Government.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted (the medical ethics committee of Kanazawa University, Approval No. 1204)) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Financial disclosure
All authors; none.
Electronic supplementary material
Below is the link to the electronic supplementary material.
10157_2017_1496_MOESM1_ESM.ppt
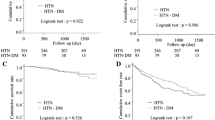
Supplementary Figure. Survival curves for each outcome as derived from the Kaplan–Meier method with log-rank test. Survival curves for the following: (A) composite kidney end points, (B) kidney death, (C) cardiovascular events, and (D) all-cause mortalities. Classification of three categories (Green & Yellow, Orange, and Red) is shown for all end points. The green line indicates Green & Yellow, the orange line indicates Orange, and the red line indicates Red. Differences between groups were compared using a log-rank test. (PPT 2869 kb)
About this article

Cite this article
Furuichi, K., Shimizu, M., Yuzawa, Y. et al. Nationwide multicenter kidney biopsy study of Japanese patients with hypertensive nephrosclerosis. Clin Exp Nephrol 22, 629–637 (2018). https://doi.org/10.1007/s10157-017-1496-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-017-1496-4