
Abstract
Background
The objective of this study was to measure the change in colonic transit time after resection rectopexy for complete rectal prolapse.
Methods
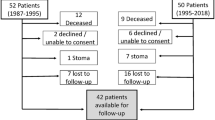
We prospectively carried out isotope colonic transit studies before resection rectopexy in 38 patients with full-thickness complete rectal prolapse and invited them to attend for a postoperative transit study at least 1 year after resection rectopexy.
Results
Preoperatively, 27 (70 %) patients had abnormally prolonged colonic transit times, while 11 had normal colonic transit. Twenty-two (61 %) patients agreed to attend for a three-day colonic transit study. Resection rectopexy failed to correct delayed colonic transit in all patients with abnormal preoperative tests, while 4 patients developed new delayed transit and 2 with normal transit were unchanged.
Conclusions
The study suggests that most prolapse patients have a pan-colonic motility disorder that is not corrected by rectopexy and resection of most of the left colon. If resection rectopexy fails to correct abnormal transit, this study questions the rationale for continuing to offer resection and supports less invasive surgical procedures such as ventral rectopexy.
Similar content being viewed by others


References
Kim DS, Tsang CB, Wong WD, Lowry AC, Goldberg SM, Madoff RD (1999) Complete rectal prolapse: evolution of management and results. Dis Colon Rectum 42:460–466
Azimuddin K, Khubchandani IT, Rosen L, Stasik JJ, Riether RD, Reed JF 3rd (2001) Rectal prolapse: a search for the “best” operation. Am Surg 67:622–627
Cirocco WC (2010) The Altemeier procedure for rectal prolapse: an operation for all ages. Dis Colon Rectum 53:1618–1623
Kim M, Reibetanz J, Boenicke L, Germer CT, Jayne D, Isbert C (2010) Quality of life after transperineal rectosigmoidectomy. Br J Surg 97:269–272
Farouk R, Duthie GS, Bartolo DC, MacGregor AB (1992) Restoration of continence following rectopexy for rectal prolapse and recovery of the internal anal sphincter electromyogram. Br J Surg 79:439–440
Madden MV, Kamm MA, Nicholls RJ, Santhanam AN, Cabot R, Speakman CT (1992) Abdominal rectopexy for complete prolapse: prospective study evaluating changes in symptoms and anorectal function. Dis Colon Rectum 35:48–55
Sayfan J, Pinho M, Alexander-Williams J, Keighley MR (1990) Sutured posterior abdominal rectopexy with sigmoidectomy compared with Marlex rectopexy for rectal prolapse. Br J Surg 77:143–145
Huber FT, Stein H, Siewert JR (1995) Functional results after treatment of rectal prolapse with rectopexy and sigmoid resection. World J Surg 19:138–143
Brown AJ, Nicol L, Anderson JH, McKee RF, Finlay IG (2005) Prospective study of the effect of rectopexy on colonic motility in patients with rectal prolapse. Br J Surg 92:1417–1422
Luukkonen P, Mikkonen U, Järvinen H (1992) Abdominal rectopexy with sigmoidectomy vs. rectopexy alone for rectal prolapse: a prospective, randomized study. Int J Colorectal Dis 7:219–222
Notghi A, Mills A, Hutchinson R, Kumar D, Harding LK (1995) Reporting simplified colonic transit studies using radionuclides: clinician friendly reports. Gut 36:274–275
Notghi A, Hutchinson R, Kumar D, Smith NB, Harding LK (1994) Simplified method for the measurement of segmental colonic transit time. Gut 35:976–981
Metcalf AM, Phillips SF, Zinsmeister AR, MacCarty RL, Beart RW, Wolff BG (1987) Simplified assessment of segmental colonic transit. Gastroenterology 92:40–47
Madiba TE, Baig MK, Wexner SD (2005) Surgical management of rectal prolapse. Arch Surg 140:63–73
Kuijpers HC (1992) Treatment of complete rectal prolapse: to narrow, to wrap, to suspend, to fix, to encircle, to plicate or to resect? World J Surg 16:826–830
Speakman CT, Madden MV, Nicholls RJ, Kamm MA (1991) Lateral ligament division during rectopexy causes constipation but prevents recurrence: results of a prospective randomized study. Br J Surg 78:1431–1433
Mollen RM, Kuijpers JH, van Hoek F (2000) Effects of rectal mobilization and lateral ligaments division on colonic and anorectal function. Dis Colon Rectum 43:1283–1287
Watts JD, Rothenberger DA, Buls JG, Goldberg SM, Nivatvongs S (1985) The management of procidentia. 30 years’ experience. Dis Colon Rectum 28:96–102
Wijffels N, Cunningham C, Dixon A, Greenslade G, Lindsey I (2011) Laparoscopic ventral rectopexy for external rectal prolapse is safe and effective in the elderly. Does this make perineal procedures obsolete? Colorectal Dis 13:561–566
Dinning PG, Bampton PA, Andre J et al (2004) Abnormal predefecatory colonic motor patterns define constipation in obstructed defecation. Gastroenterology 127:49–56
Orr TG (1947) A suspension operation for prolapse of rectum. Ann Surg 126:833–837
Loygue J, Cerbonnet G (1957) Surgical treatment of total prolapse of the rectum by rectopexy following the Orr technic; based on 14 case reports. Mem Acad Chir 83:325–329
D’Hoore A, Penninckx F (2006) Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc 20:1919–1923
Samaranayake CB, Luo C, Plank AW, Merrie AE, Plank LD, Bissett IP (2010) Systematic review on ventral rectopexy for rectal prolapse and intussusception. Colorectal Dis 12:504–512
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
El Muhtaseb, M.S., Bartolo, D.C.C., Zayiae, D. et al. Colonic transit before and after resection rectopexy for full-thickness rectal prolapse. Tech Coloproctol 18, 273–276 (2014). https://doi.org/10.1007/s10151-013-1053-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-013-1053-4