
Abstract
Background
The occurrence of postoperative complications may have a significant negative impact on the prognosis of patients with gastrointestinal cancers. The inflammatory response releases systemic cytokines, which may induce residual cancer cell growth. Recently, neoadjuvant chemotherapy (NAC) was found to improve the prognosis of advanced gastric cancer (GC). We hypothesize that when postoperative complications occur after gastrectomy, NAC treatment of micrometastases can prevent residual cancer cell growth.
Methods
This study included 101 patients who underwent curative resection after NAC for GC from 2005 to 2015. Clinical data, including intraoperative parameters, were collected retrospectively. Overall survival (OS) and relapse-free survival (RFS) were compared between the patients with complications and those without complications.
Results
Of the 101 patients, 35 (34.7%) had grade 2 or higher complications. Among those with complications, the 3- and 5-year OS rates were 63.5 and 58.2% and the 3- and 5-year RFS rates 41.7 and 41.7%, respectively. Among those without complications, the 3- and 5-year OS rates were 65.9 and 56.3% and the 3- and 5-year RFS rates 51.1 and 43.9%, respectively. There was no significant difference in prognosis between the patients with complications and those without complications.
Conclusion
Our study is the first to demonstrate the potential of NAC to abolish the poor prognosis induced by postoperative complications after curative resection for GC.
Similar content being viewed by others


Introduction
Gastric cancer (GC) is the fourth most commonly diagnosed malignancy and the second leading cause of cancer death worldwide [1]. Despite the recent progress in cancer treatment, the prognosis of patients with advanced GC remains poor. Gastrectomy and regional lymph node dissection are the most powerful treatments for patients with GC; however, recurrence and metastasis can be observed in 20–60% of patients even after curative surgery for GC [2,3,4]. Approximately 10–20% of patients with GC who are considered for potentially curative resection have invisible peritoneal seeding at the time of surgery, and even patients treated with curative intent experience invisible metastasis not long after resection [5]. Despite significant advances in surgical skills and medical instruments such as laparoscopic or robotic devices, surgery is not capable of treating invisible micrometastases in blood and other organs and thus cannot prevent all cases of recurrence.
Previous studies revealed that the occurrence of postoperative complications, especially inflammatory complications, could have a significant negative impact on the prognosis of patients with colorectal cancer, esophageal cancer, and GC [6,7,8,9,10,11,12,13]. The association between postoperative complications and a negative prognosis is considered to result from the release of systemic cytokines during inflammatory responses, and these factors may induce residual cancer cell growth [10, 14].
Adjuvant chemotherapy with S-1 demonstrated a significant survival benefit over surgery alone in patients with GC, and it was successful in treating invisible micrometastases [15, 16]. Recently, administration of neoadjuvant chemotherapy (NAC) was found to improve the prognosis of patients with advanced GC by downstaging the tumor, eliminating micrometastases, and rapidly improving tumor-related symptoms [17,18,19,20,21,22,23]. We hypothesized that eliminating micrometastases by NAC before postoperative complications occur after gastrectomy may suppress the growth of residual invisible cancer cells and control metastasis.
The aim of this study was to evaluate whether NAC abolishes the poor prognosis induced by postoperative complications after gastrectomy.
Patients and methods
Data collection
From March 2005 to December 2015, a total of 101 patients with GC underwent curative (R0) gastrectomy after receiving NAC at the Cancer Institute Hospital of the Japanese Foundation for Cancer Research, Tokyo, Japan. The eligibility criteria for NAC were bulky N GC, para-aortic lymph node swelling, and type 4 and large type 3 GC (clinical trial: JCOG0501, 1002). Surgery was performed within 3–5 weeks from the last chemotherapy treatment. Gastrectomy and lymph node dissection were carried out according to the recommendations of the Japanese Research Society for GC [24]. Patients underwent open gastrectomy with standardized extended lymphadenectomy (D2). Moreover, we performed para-aortic lymph node dissection if para-aortic lymph node swelling persisted after NAC. If para-aortic lymph node swelling did not persist after NAC, we performed para-aortic lymph node sampling. Tumor staging was evaluated according to the seventh edition of the International Union Against Cancer tumor, node, metastasis (TNM) classification system. Information including patient characteristics, surgical records, and pathological data were obtained from a database of the Cancer Institute Hospital. The dates and causes of death were determined from follow-up data collected during clinical examinations performed every 3–6 months after discharge.
Evaluation of complications
During the postoperative period, all patients were observed for any complications, and only those occurring within 1 month after surgery were recorded. The severity of postoperative complications was evaluated according to the Clavien–Dindo classification system. We considered complications of grade II or higher as postoperative complications in this study, and we divided the patients into two groups: those with complications (C group) and those without complications (NC group). When two or more complications occurred in one patient, the higher-grade complication was used. We considered inflammatory complications such as pneumonia, catheter infection, cholecystitis, and infection at the surgical site (SSI), including wound infection (superficial and deep incisional SSIs) and organ space SSIs caused by abscess, leakage, and pancreatic fistula. Additionally, to evaluate the postoperative inflammation status, we obtained blood samples from patients on days 1, 3, 5, and 7 after surgery and measured relevant parameters including white blood cell (WBC) counts and C-reactive protein (CRP) levels. Body temperature (BT) was measured every day, and the peak BT for each day was recorded.
Statistics
Overall survival (OS) was defined as the interval from surgery to the date of death from any cause, or the last follow-up in living patients. Recurrence-free survival (RFS) was defined as the interval from surgery to either the first recurrence or death from any cause. Clinicopathological characteristics and laboratory data were compared between the C and NC groups using the chi-square test for categorical variables and the Mann–Whitney U test for continuous variables. Cumulative survival was plotted using the Kaplan–Meier method, and differences were compared using the log-rank test. P values < 0.05 were considered statistically significant. The Cox proportional hazards model was applied to assess the effects of covariates on RFS in both univariate and multivariate analyses with the categorical covariates listed in Tables 3 and 4. We conducted multivariate analysis using factors that were < 0.10 in univariate analysis (age, gender, ypN, histological response, operation time, and blood loss). Patients with missing covariate values were excluded. All tests were analyzed using JMP software (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
A total of 35 patients (34.7%) were included in the C group and a total of 27 patients (26.7%) were included in the inflammatory complications group. The complications experienced were anastomotic leakage (3 patients, 3.0%), pancreatic fistula (7 patients, 6.9%), intra-abdominal infection (10 patients 9.9%), pneumonia (3 patients, 3.0%), wound infection (2 patients, 2.0%), catheter infection (1 patients, 1.0%), and cholecystitis (1 patients, 1.0%). Of these, 18 (17.8%) patients had grade 3 complications requiring surgical, endoscopic, or radiological intervention. Table 1 summarizes the baseline characteristics before surgery of the 101 patients who underwent curative resection for GC according to the presence of complications. The incidence of complications was only significantly associated with sex. Table 2 summarizes the intraoperative factors and postoperative pathological factors. The C group had a significantly longer operation time and a tendency towards an extent lymphadenectomy rate. However, the pathological stage and proportion of the patients who received adjuvant therapy were not significantly different between the two groups. Moreover, the data on the duration of adjuvant chemotherapy were not significantly different between the two groups.
Survival outcomes
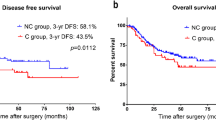
The median follow-up time for the 101 patients was 33.7 months. Of the 41 patients (40.6%) who died within this period, 33 died of GC. During the follow-up, 50 patients (49.5%) developed recurrence (24 in the lymph nodes, 15 in the peritoneum, 10 in the liver, and 7 in other sites), while 6 patients (5.9%) died from other diseases. Among all patients, the 3-year OS rate was 65.5% and the 3-year RFS rate was 45.8%. In the C group, the 3-year OS rate was 61.9% and the 3-year RFS rate was 41.7%. In the NC group, the 3-year OS rate was 65.7% and the 3-year RFS rate was 47.0%. The OS and RFS results are represented graphically in Fig. 1a, b, respectively, and the resultant curves stratified by inflammatory complications are shown in Fig. 2a, b. There were no significant differences between the two groups. The only risk factor for 3-year OS was the histological response of the primary tumor. The risk factors for 3-year RFS were histological response of the primary tumor and gender. The presence of complications was not a risk factor for survival in this cohort (Tables 3, 4).

Kaplan–Meier analyses of overall survival (a) and relapse-free survival (b) in patients with and without complications after resection of GC with curative intent

Kaplan–Meier analyses of overall survival (a) and relapse-free survival (b) in patients with and without inflammatory complications after resection of GC with curative intent
Postoperative changes in the WBC count, CRP level, and BT
Figure 3 shows the changes in clinical and laboratory data according to the presence of inflammatory complications over the postoperative period. The mean BT peaked on day 1 and then decreased. The mean WBC count and CRP level peaked on day 3 and then decreased. The mean WBC count, CRP level, and BT were all significantly higher in the C group than in the NC group. The RFS tended to be worse for high-peak CRP groups than for low-peak CRP groups (Fig. S1a, b in the Electronic supplementary material, ESM). However, univariate analysis for RFS was performed, there was no significant difference in postoperative infectious complications or peak CRP level (Table 3).

Changes in the white blood cell count (a), C-reactive protein level (b), and body temperature (c) in patients with and without complications after resection of GC with curative intent. For the analysis, we used the peak body temperatures for each day evaluated. Bars show standard errors. *P < 0.05, **P < 0.005
Discussion
The present study revealed that the prognosis of the 101 patients with GC who underwent curative gastrectomy after NAC was not significantly affected by the occurrence of complications. We demonstrated the possibility that NAC abolishes the poor prognosis induced by postoperative complications.
Kubota et al. revealed that postoperative complications prolonged inflammation and negatively impacted prognosis in 1395 patients who underwent curative resection for GC [12]. Their finding that survival was different between patients with and without complications was especially remarkable in those with pStage III GC. Our study enrolled similar cases with locally advanced or extensive lymph node metastasis. In such cases, the occurrence of postoperative complications may affect prognosis more adversely because there is a high probability with advanced GC that residual and circulating cancer cells will remain. However, in our study, the prognosis was not significantly different between the C and NC groups. We consider that NAC is capable of treating invisible micrometastases and abolishing the poor prognosis induced by postoperative complications.
Next, we focused on the postoperative inflammatory response. The mediators and cellular effectors of inflammation are important constituents of the local tumor environment. The inflammatory cells and mediators in tumor tissues induce tissue remodeling and angiogenesis [25]. The long-term follow-ups performed in randomized trials have shown that aspirin reduces the risk of colorectal cancer after a delay of several years, possibly via inhibition of COX-2, which is one of the major inflammatory cytokines [26]. It was shown recently that postoperative peritoneal fluid from infected patients after surgery for colorectal cancer enhanced both the migration and invasion of residual tumor cells, thus facilitating their growth into recurrent tumors [27]. These findings suggest that inflammation caused by postoperative complications leads to the release of systemic cytokines and immunosuppression, which cause metastasis and recurrence. In the present study, the postoperative inflammatory response (as defined by BT, WBC count, and CRP level) was significantly increased and prolonged in the C group; however, the prognosis was not significantly different between the C and NC groups. Moreover, we evaluated the prognosis of the patients with inflammatory complications within the C group. There was no significant difference in prognosis between the patients with and those without inflammatory complications. The RFS tended to be worse for high-peak CRP groups than for low-peak CRP groups (Fig. S1a, b in the ESM). We believe that it is difficult to completely abolish the impact of inflammation, but the results of this study show an improved prognosis compared to the report by Kubota et al. [12].
There are several limitations of our study. First, this study was a retrospective analysis conducted at a single institution and thus might be subject to several biases. The number of cases was relatively small, and the patient background characteristics showed nonuniform distributions. Hence, a prospective multi-institutional study is desirable to validate the present findings. Second, this study was subject to the shortcomings generally associated with observational studies. The median follow-up of 33.7 months was relatively short. However, when it occurs, recurrence of GC usually develops within the first 2 years after surgery, so our follow-up time may have been sufficient considering the recurrence rate [28].
In conclusion, the results we have presented here are the first to demonstrate the possibility that NAC abolishes the poor prognosis induced by postoperative complications after curative resection in patients with GC, suggesting a novel effect of NAC as a prophylactic therapy for GC. Further basic and clinical studies of the mechanisms of micrometastasis, inflammatory mediators, and the microenvironment of the tumor are necessary in the future. These findings may help to improve the prognosis of patients with GC.
References
Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–50.
Rivera F, Vega-Villegas ME, Lopez-Brea MF. Chemotherapy of advanced gastric cancer. Cancer Treat Rev. 2007;33:315–24.
Maehara Y, Hasuda S, Koga T, et al. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. Br J Surg. 2000;87:353–7.
Isobe Y, Nashimoto A, Akazawa K, et al. Gastric cancer treatment in Japan: 2008 annual report of the JGCA nationwide registry. Gastric Cancer. 2011;14:301–16.
Gretschel S, Siegel R, Estevez-Schwarz L, et al. Surgical strategies for gastric cancer with synchronous peritoneal carcinomatosis. Br J Surg. 2006;93:1530–5.
Walker KG, Bell SW, Rickard MJ, et al. Anastomotic leakage is predictive of diminished survival after potentially curative resection for colorectal cancer. Ann Surg. 2004;240:255–9.
Artinyan A, Orcutt ST, Anaya DA, et al. Infectious postoperative complications decrease long-term survival in patients undergoing curative surgery for colorectal cancer: a study of 12,075 patients. Ann Surg. 2015;261:497–505.
Lerut T, Moons J, Coosemans W, et al. Postoperative complications after transthoracic esophagectomy for cancer of the esophagus and gastroesophageal junction are correlated with early cancer recurrence: role of systematic grading of complications using the modified Clavien classification. Ann Surg. 2009;250:798–807.
Rizk NP, Bach PB, Schrag D, et al. The impact of complications on outcomes after resection for esophageal and gastroesophageal junction carcinoma. J Am Coll Surg. 2004;198:42–50.
Sierzega M, Kolodziejczyk P, Kulig J. Impact of anastomotic leakage on long-term survival after total gastrectomy for carcinoma of the stomach. Br J Surg. 2010;97:1035–42.
Tokunaga M, Tanizawa Y, Bando E, et al. Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann Surg Oncol. 2013;20:1575–83.
Kubota T, Hiki N, Sano T, et al. Prognostic significance of complications after curative surgery for gastric cancer. Ann Surg Oncol. 2014;21:891–8.
Saito T, Kurokawa Y, Miyazaki Y, et al. Which is a more reliable indicator of survival after gastric cancer surgery: postoperative complication occurrence or C-reactive protein elevation? J Surg Oncol. 2015;112:894–9.
Bohle B, Pera M, Pascual M, et al. Postoperative intra-abdominal infection increases angiogenesis and tumor recurrence after surgical excision of colon cancer in mice. Surgery. 2010;147:120–6.
Sakuramoto S, Sasako M, Yamaguchi T, et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med. 2007;357:1810–20.
Eguchi T, Kodera Y, Nakanishi H, et al. The effect of chemotherapy against micrometastases and isolated tumor cells in lymph nodes: an in vivo study. In Vivo. 2008;22:707–12.
Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20.
Ajani JA, Mansfield PF, Janjan N, et al. Multi-institutional trial of preoperative chemoradiotherapy in patients with potentially resectable gastric carcinoma. J Clin Oncol. 2004;22:2774–80.
Schuhmacher C, Gretschel S, Lordick F, et al. Neoadjuvant chemotherapy compared with surgery alone for locally advanced cancer of the stomach and cardia: European Organisation for Research and Treatment of Cancer randomized trial 40954. J Clin Oncol. 2010;28:5210–8.
Yoshikawa T, Sasako M, Yamamoto S, et al. Phase II study of neoadjuvant chemotherapy and extended surgery for locally advanced gastric cancer. Br J Surg. 2009;96:1015–22.
Tsuburaya A, Nagata N, Cho H, et al. Phase II trial of paclitaxel and cisplatin as neoadjuvant chemotherapy for locally advanced gastric cancer. Cancer Chemother Pharmacol. 2013;71:1309–14.
Kosaka T, Akiyama H, Makino H, et al. Preoperative S-1 and docetaxel combination chemotherapy in patients with locally advanced gastric cancer. Cancer Chemother Pharmacol. 2014;73:281–5.
Oki E, Emi Y, Kusumoto T, et al. Phase II study of docetaxel and S-1 (DS) as neoadjuvant chemotherapy for clinical stage III resectable gastric cancer. Ann Surg Oncol. 2014;21:2340–6.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines (ver 3). Gastric Cancer. 2010;2011(14):113–23.
Balkwill F, Charles KA, Mantovani A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell. 2005;7:211–7.
Rothwell PM, Fowkes FG, Belch JF, et al. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet. 2011;377:31–41.
Salvans S, Mayol X, Alonso S, et al. Postoperative peritoneal infection enhances migration and invasion capacities of tumor cells in vitro: an insight into the association between anastomotic leak and recurrence after surgery for colorectal cancer. Ann Surg. 2014;260:939–43.
Baiocchi GL, Marrelli D, Verlato G, et al. Follow-up after gastrectomy for cancer: an appraisal of the Italian Research Group for Gastric Cancer. Ann Surg Oncol. 2014;21:2005–11.
Author information
Authors and Affiliations
Contributions
Study conception and design: KE, NH, KK, TS, and TY; acquisition of the data: KE, NH, and KK; analysis and interpretation of the data: KE, NH, and KK; writing of the manuscript: KE, NH, KK, TS, and TY. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and patient consent
The data collection and analysis were approved by the institutional review board of the Cancer Institute Hospital. Informed consent was obtained from all patients before they were included in this study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
10120_2017_781_MOESM1_ESM.pptx
Fig. S1 Kaplan–Meier analyses of overall survival (a) and relapse-free survival (b) comparing the low-peak and high-peak CRP groups after resection of GC with curative intent (PPTX 86 kb)
Rights and permissions
About this article

Cite this article
Eto, K., Hiki, N., Kumagai, K. et al. Prophylactic effect of neoadjuvant chemotherapy in gastric cancer patients with postoperative complications. Gastric Cancer 21, 703–709 (2018). https://doi.org/10.1007/s10120-017-0781-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-017-0781-y