
Abstract
Objectives
(1) Development and validation of a composite ultrasound score (cUSS) for the diagnosis of carpal tunnel syndrome (CTS). (2) To predict treatment response after local corticosteroid injection.
Methods
Wrists of CTS patients and controls were evaluated with high-resolution ultrasound and cross-sectional area of median nerve at carpal tunnel inlet (CSAp) and outlet (CSAd) and bowing of flexor retinaculum (FRB), flexor tenosynovitis, and intraneural vascularity and echogenicity changes were noted. Patients were prospectively followed after ultrasound-guided corticosteroid injection.
Results
We studied 479 wrists of 141 patients and 99 controls. Optimal cut-offs for diagnosing CTS were 9.5 mm2 and 10.5 mm2, respectively, for CSAp and CSAd. A cUSS consisting of the following parameters was developed: age, CSAp, CSAd, FRB, and flexor tenosynovitis and echogenicity changes. External validation of cUSS yielded sensitivity, specificity, and diagnostic accuracy of 91.7%, 87.1%, and 89.8%, respectively. Treatment responses from 88 injections (median duration of follow-up of 6 months) were available with satisfactory initial responses in 69.32% (61/88) and relapses in 30.86% (25/81). Median time to relapse was 2 months. Initial response was predicted by FRB (odds ratio (OR): 5.43, 95% confidence interval (CI): 1.45–20.3, p = 0.012). Relapse was predicted by age (hazard ratio (HR) 1.168, 95% CI: 1.076–1.268, p = 0.0002), male gender (HR: 8.1.02, 95% CI: 2.394–27.422, p = 0.0007), FRB, (HR: 46.982, 95% CI: 5.048–437.293, p = 0.0008), and higher body mass index (HR: 0.238, 95% CI: 0.064–0.892, p = 0.0332).
Conclusions
The developed cUSS has a diagnostic accuracy of 88% for diagnosing CTS. Ultrasound parameters could predict both initial treatment response and relapse.
Key points
• Anatomical ultrasound parameters in addition to nerve cross-sectional area is important for diagnosis of CTS.
• A composite US score for diagnosis of CTS was developed with accuracy 88.6%.
• Bowing of flexor retinaculum predicts short and long term response to local steroid injection.

Similar content being viewed by others


References
Klauser AS, Faschingbauer R, Bauer T, Wick M, Gabl M, Arora R, Cotten A, Martinoli C, Jaschke W (2010) Entrapment neuropathies II: carpal tunnel syndrome. Semin Musculoskelet Radiol 14:487–500
Roll SC, Case-Smith J, Evans KD (2011) Diagnostic accuracy of ultrasonography vs. electromyography in carpal tunnel syndrome: a systematic review of literature. Ultrasound Med Biol 37:1539–1553
Fowler JR, Gaughan JP, Ilyas AM (2011) The sensitivity and specificity of ultrasound for the diagnosis of carpal tunnel syndrome: a meta-analysis. Clin Orthop Relat Res 469:1089–1094
Seror P (2008) Sonography and electrodiagnosis in carpal tunnel syndrome diagnosis, an analysis of the literature. Eur J Radiol 67:146–152
Dejaco C, Stradner M, Zauner D et al (2013) Ultrasound for diagnosis of carpal tunnel syndrome: comparison of different methods to determine median nerve volume and value of power Doppler sonography. Ann Rheum Dis 72:1934–1939
Klauser AS, Halpern EJ, De Zordo T et al (2009) Carpal tunnel syndrome assessment with US: value of additional cross-sectional area measurements of the median nerve in patients versus healthy volunteers. Radiology 250:171–177
Hobson-Webb LD, Massey JM, Juel VC, Sanders DB (2008) The ultrasonographic wrist-to-forearm median nerve area ratio in carpal tunnel syndrome. Clin Neurophysiol 119:1353–1357
Hobson-Webb LD, Padua L (2009) Median nerve ultrasonography in carpal tunnel syndrome: findings from two laboratories. Muscle Nerve 40:94–97
Yesildag A, Kutluhan S, Sengul N et al (2004) The role of ultrasonographic measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin Radiol 9:910–915
Duncan I, Sullivan P, Lomas F (1999) Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol 173:681–684
Karadağ YS, Karadağ O, Ciçekli E (2010) Severity of carpal tunnel syndrome assessed with high frequency ultrasonography. Rheumatol Int 30:761–765
Buchberger W, Judmaier W, Birbamer G, Lener M, Schmidauer C (1992) Carpal tunnel syndrome: diagnosis with high-resolution sonography. AJR Am J Roentgenol 159:793–798
Nakamichi K, Tachibana S (2002) Ultrasonographic measurement of median nerve cross-sectional area in idiopathic carpal tunnel syndrome: diagnostic accuracy. Muscle Nerve 26:798–803
Ng AWH, Griffith JF, Lee RKL (2018) Ultrasound carpal tunnel syndrome: additional criteria for diagnosis. Clin Radiol 73:214.e11–214.e18
Hosmer DW, Hjort NL (2002) Goodness-of-fit processes for logistic regression: simulation results. Stat Med 21:2723–2738
Tobias A, Campbell MJ (1998) Akaike’s information criterion and Schwarz’s criterion. Stata Tech Bull 45:23–25
Raftery AE (1996) Bayesian model selection in social research. In: Marsden PV (ed) Sociological methodology. Blackwell, London, Oxford, pp 111–163
Sullivan LM, Massaro JM, D’Agostino RB (2004) Presentation of multivariate data for clinical use: the Framingham Study risk score functions. Stat Med 23:1631–1660
Wong SM, Griffith JF, Hui AC, Lo SK, Fu M, Wong KS (2004) Carpal tunnel syndrome: diagnostic usefulness of sonography. Radiology 232:93–99
Sernik RA, Abicalaf CA, Pimentel BF, Braga-Baiak A, Braga L, Cerri GG (2008) Ultrasound features of carpal tunnel syndrome: a prospective caseecontrol study. Skeletal Radiol 37:49–53
Kwon BC, Jung KI, Baek GH (2008) Comparison of sonography and electro- diagnostic testing in the diagnosis of carpal tunnel syndrome. J Hand Surg Am 33:65–71
Moran L, Perez M, Esteban A, Bellon J, Arranz B, del Cerro M (2009) Sonographic measurement of cross- sectional area of the median nerve in the diagnosis of carpal tunnel syndrome: correlation with nerve conduction studies. J Clin Ultrasound 37:125–131
Akcar N, Ozkan S, Mehmetoglu O, Calisir C, Adapinar B (2010) Value of power Doppler and gray-scale US in the diagnosis of carpal tunnel syndrome: contribution of cross-sectional area just before the tunnel inlet as compared with the cross-sectional area at the tunnel. Korean J Radiol 11:632–639
Bak L, Bak S, Gaster P, Mathiesen F et al (1997) MR imaging of the wrist in carpal tunnel syndrome. Acta Radiol 38:1050–1052
Healy C, Watson JD, Longstaff A, Campbell MJ (1990) Magnetic resonance imaging of the carpal tunnel. J Hand Surg Br 15:243–248
Altinok T, Baysal O, Karakas HM et al (2004) Ultrasonographic assessment of mild and moderate idiopathic carpal tunnel syndrome. Clin Radiol 59:916–925
Sarría L, Cabada T, Cozcolluela R, Martínez-Berganza T, García S (2000) Carpal tunnel syndrome: usefulness of sonography. Eur Radiol 10:1920–1925
Radack DM, Schweitzer ME, Taras J (1997) Carpal tunnel syndrome :are the MR findings a result of population selection bias? AJR Am J Roentgenol 169:1649–1653
Tsujii M, Hirata H, Morita A, Uchida A (2009) Palmar bowing of the flexor retinac- ulum on wrist MRI correlates with subjective reports of pain in carpal tunnel syndrome. J Magn Reson Imaging 29:1102–1105
Agarwal V, Singh R, Sachdev A, Wiclaff SS, Goel D (2005) A prospective study of the long-term efficacy of local methyl prednisolone acetate injection in the management of mild carpal tunnel syndrome. Rheumatology (Oxford) 44:647–650
Green DP (1984) Diagnostic and therapeutic value of carpal tunnel injection. J Hand Surg 9A:850–854
Gelberman RH, Aronson D, Weismann MH (1980) Carpal tunnel syndrome: results of a prospective trial of steroid injection and splinting. J Bone Joint Surg Am 62:1181–1184
Giannini F, Passero S, Cioni R et al (1991) Electrophysiologic evaluation of local steroid injection in carpal tunnel syndrome. Arch Phys Med Rehabil 72:738–742
Dammers JWHH, Veering MM, Vermeulen M (1999) Injection with methyl prednisolone proximal to the carpal tunnel: randomised double blind trial. BMJ 319:884–886
O'Gradaigh D, Merry P (2000) Corticosteroid injection for the treatment of carpal tunnel syndrome. Ann Rheum Dis 59:918–919
Kaplan SJ, Glickel SZ, Eaton RG (1990) Predictive factors in the non-surgical treatment of carpal tunnel syndrome. J Hand Surg [Br] 15:106–108
Goodman HV, Foster JB (1962) Effect of local corticosteroid injection on median nerve conduction in carpal tunnel syndrome. Ann Phys Med 7:287
Meys V, Thissen S, Rozeman S, Beekman R (2011) Prognostic factors in carpal tunnel syndrome treated with a corticosteroid injection. Muscle Nerve 44:763–768
Chung SY, Kwak JM, Kang S, Son SH, Kim JD, Yoon JS (2018) Predictive variables for sonographically guided corticosteroid injection in mild-to-moderate carpal tunnel syndrome. Ann Rehabil Med 42:213–221
Chakkalakkoombil SV, Nair PP, Govindarajalou R, Barathi D, Marusani R, Kumar Kottyen Thazhath H (2019) Role of ultrasound to monitor patients with carpal tunnel syndrome treated with a local corticosteroid. J Ultrasound Med 38:2373–2378
Asadov R, Erdal A, Buğdaycı O, Gündüz OH, Ekinci G (2018) The effectiveness of ultrasonography and ultrasonographic elastography in the diagnosis of carpal tunnel syndrome and evaluation of treatment response after steroid injection. Eur J Radiol 108:172–176
Rempel D, Dahlin L, Lundborg G (1999) Pathophysiology of nerve compression syndromes: response of peripheral nerves to loading. J Bone Joint Surg Am 81:1600–1610
Niessen FB, Spauwen PH, Schalkwijk J, Kon M (1999) On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg 104:1435–1458
Ketchum LD, Robinson DW, Masters FW (1967) The degradation of mature collagen: a laboratory study. Plast Reconstr Surg 40:89–91
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Our study complies with the Declaration of Helsinki and was reviewed by the Institutional Ethics Committee of IPGME&R, Kolkata, and the ethics committee has approved the research protocol (ethics no. IPGME&R/IEC/2018/042), and prior written informed consent has been obtained from all the subjects.
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 124 kb)
Figure S1
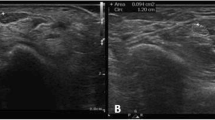
Panel of images showing median nerve in various points of the carpal tunnel of a single patient. The median nerve is imaged in various parts of the carpal tunnel: in proximal carpal tunnel (A), in distal carpal tunnel (B), panoramic view of proximal tunnel (C) and longitudinal view of the median nerve (D). In the cross-sectional view of the proximal part of the tunnel (Panel A) at the level of the pisiform (white hollow arrowhead), the median nerve is seen to lie just below the flexor retinaculum (multiple solid white arrowheads) and the retinaculum is seen to gain attachment at the ulnar side on the scaphoid tubercle. To measure bowing a horizontal dotted line is drawn from the scaphoid tubercle to the pisiform and a vertical distance measurement line (Green A and B) are drawn from this horizontal line to the top of the retinaculum. In this picture the bowing distance was 5 mm. In the cross-sectional view of the distal part of the tunnel (panel B), the median nerve (solid white star) is seen to lie between the trapezium (black star with white borders). In the panoramic view of the proximal carpal tunnel (panel C), both the radial (gree and yellow flow signals) and ulnar (red flow signals) are seen and the flexor digitorum superficialis tendons (white arrows) are seen lying below the median nerve (dotted green outline). The flexor carpi radialis (solid white star) lies outside the flexor retinaculum. The area of the median nerve was 8 mm2 in this patient. In the longitudinal view of the median nerve (panel D, the median nerve (solid white arrowheads) is seen lying on top of the flexor digitorum tendon (solid black star). There are inhomogeneoous hyperechoic changes within the nerve (hollow arrowhead with white borders). This patient had carpal tunnel syndrome with electrodiagnostic findings with median nerve area less than the cut off but ancillary criteria was positive. (JPG 140 kb)
Figure S2
Panel of images showing median nerve in various points of the carpal tunnel showing different pathologies. In panel A, the median nerve (white solid star) is traced out. Panel B shows an elarged median nerve with a cross-sectional area of 28 mm2. In panel C, the median neve (solid white star) in the proximal carpal tunnel, is seen to lie below the flexor retinauculm (hollow arrowhead with white borders). The flexor digitorum superficialis tendons (solid black stars with white borders) and the flexor digitorum profundus tendons (solid white stars with black borders) are displaced by the presence of flexor tenosynovitis marked by fluid accumulation (solid white arrowheads). In panel D (same picture as Panel A but the median nerve is not traced out) presence of flexor tenosynovitis (solid white arrowheads) is presence in the intervening areas and inbetween the flexor digitorum superficialis tendons (solid black stars with white borders) and the flexor digitorum profundus tendons (solid white stars with black borders). (JPG 121 kb)
Figure S3 Survival curves for the presence and absence of bowing each for male and female, keeping age fixed at median level We have further tested the similarities between them using the Mantel Cox test. The data shows that the odds ratio (OR) of relapse for the male patients in the presence of bowing compared to absence is 1.25 (95% confidece interval: 0.12–13.24). Similarly for the female patients, OR of relapse in the presence of bowing compared to absence is 3.83 (95% CI 0.98–14.99). The results of the Mantel Cox test shows for male patients relapse occurred in 5/9 males with baseline bowing compared to 2/4 in no baseline bowing (p = 0.02). For females, relapse occurred in 14/42 with baseline bowing comapred to 3/26 without bowing at baseline (p = 0.03).
Rights and permissions
About this article

{kind=link}
{kind=link}
Cite this article
Goswami, R.P., Sit, H., Chatterjee, M. et al. High-resolution ultrasonography in carpal tunnel syndrome: role of ancillary criteria in diagnosis and response to steroid injection. Clin Rheumatol 40, 1069–1076 (2021). https://doi.org/10.1007/s10067-020-05228-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-020-05228-8