
Abstract
Background
Few data are available on disability and quality of life (QOL) after surgery versus conservative management for unruptured brain arteriovenous malformations (uAVMs).
Objective
The aim of this study was to test the hypothesis that QOL and disability are worse after surgery ± preoperative embolisation for uAVM compared with conservative management.
Methods
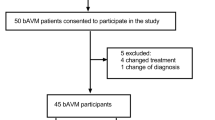
We included consecutive patients diagnosed with uAVM from a prospective population-based study in Scotland (1999–2003; 2006–2010) and a prospective hospital-based series in Australia (2011–2015). We assessed outcomes on the modified Rankin Scale (mRS) and the Short Form (SF)-36 at ~ 12 months after surgery or conservative treatment and compared these groups using continuous ordinal regression in the two cohorts separately.
Results
Surgery was performed for 29% of all uAVM cases diagnosed in Scotland and 84% of all uAVM referred in Australia. There was no statistically significant difference between surgery and conservative management at 12 months among 79 patients in Scotland (mean SF-36 Physical Component Score (PCS) 39 [SD 14] vs. 39 [SD 13]; mean SF-36 Mental Component Score (MCS) 38 [SD 14] vs. 39 [SD 14]; mRS > 1, 24 vs. 9%), nor among 37 patients in Australia (PCS 51 [SD 10] vs. 49 [SD 6]; MCS 48 [SD 12] vs. 49 [SD 10]; mRS > 1, 19 vs. 30%). In the Australian series, there was no statistically significant change in the MCS and PCS between baseline before surgery or conservative management and 12 months.
Conclusions
We did not find a statistically significant difference between surgery ± preoperative embolisation and conservative management in disability or QOL at 12 months.

Similar content being viewed by others


References
Al-Shahi Salman R, White PM, Counsell CE, du Plessis J, van Beijnum J, Josephson CB, Wilkinson T, Wedderburn CJ, Chandy Z, St George EJ, Sellar RJ, Warlow CP, Scottish Audit of Intracranial Vascular Malformations Collaborators (2014) Outcome after conservative management or intervention for unruptured brain arteriovenous malformations. JAMA 311:1661–1669
Bayliss EA, Bayliss MS, Ware JE (2004) Predicting declines in physical function in persons with multiple chronic medical conditions: what we can learn from the medical problem list. Health Qual Life Outcomes 2:47. https://doi.org/10.1186/1477-7525-2-47
Bervini D, Morgan MK, Ritson EA, Heller G (2014) Surgery for unruptured arteriovenous malformations of the brain is better than conservative management for selected cases: a prospective cohort study. J Neurosurg 121:878–890
Davidson AS, Morgan MK (2010) How safe is arteriovenous malformation surgery? A prospective, observational study of surgery as first-line treatment for brain arteriovenous malformations. Neurosurgery 66:498–504
Della Puppa A, Rustemi O, Scienza R (2015) Quality of life of patients affected by unruptured brain AVMs. J Neurosurg 122:984–985
Iansek R, Elstein AS, Balla JI (1983) Application of decision analysis to management of cerebral arteriovenous malformation. Lancet 1(8334):1132–1135
Lai EHP, Lun SLC (2002) Impact on the quality of life of patients with arteriovenous malformations during the latent interval between gamma knife radiosurgery and lesion obliteration. J Neurosurg 97(SUPPL. 5):471–473
Magro E, Gentric J-C, Darsault TE, Ziegler D, Bojanowski MW, Raymond J (2017) Response to ARUBA: a systematic review and critical analysis for the design of future arteriovenous malformation trials. J Neurosurg 126:486–494
Mahoney FI, Barthel DW (1965) Functional evaluation: the Barthel Index. Md State Med J 14:61–65
Manuguerra M, Heller GZ (2010) Ordinal regression models for continuous scales. Int J Biostat 6:Article 14
Mast H, Young WL, Koennecke HC, Sciacca RR, Osipov A, Pile-Spellman J, Hacein-Bey L, Duong H, Stein BM, Mohr JP (1997) Risk of spontaneous haemorrhage after diagnosis of cerebral arteriovenous malformation. Lancet 350:1065–1068
Mohr JP, Moskowitz AJ, Stapf C, Hartmann A, Lord K, Marshall SM, Mast H, Moquete E, Moy CS, Parides M, Pile-Spellman J, Al-Shahi Salman R, Weinberg A, Young WL, Estevez A, Kureshi I, Brisman JL (2010) The ARUBA trial: current status, future hopes. Stroke 41(8):e537–e540
Mohr JP, Overby JR, von Kummer R, Stefani MA, Libman R, Stapf C, Parides MK, Pile-Spellman J, Moquete E, Moy CS, Vicaut E, Moskowitz AJ, Harkness K, Cordonnier C, Biondi A, Houdart E, Berkefeld J, CJM K, Barreau X, Kim H, Hartmann A, International ARUBA investigators (2017) Functional impairments for outcomes in a randomized trial of unruptured brain AVMs. Neurology 89(14):1499–1506
Mohr JP, Parides MK, Stapf C, Moquete E, Moy CS, Overbey JR, Al-Shahi Salman R, Vicaut E, Young WL, Houdart E, Cordonnier C, Stefani MA, Hartmann A, von Kummer R, Biondi A, Berkefeld J, Klijn CJ, Harkness K, Libman R, Barreau X, Moskowitz AJ, international ARUBA investigators (2014) Medical management with or without interventional therapy for unruptured brain arteriovenous malformations (ARUBA): a multicentre, non-blinded, randomised trial. Lancet 383:614–621
Moon K, Levitt MR, Nakaji P, Albuquerque FC, Zabramski JM, McDougall CG, Spetzler RF (2015) Safety and efficacy of surgical resection of unruptured low-grade arteriovenous malformations from the modern decade. Neurosurgery 77:948–953
O’Donnell J, Morgan MK (2015) Response. J Neurosurg 122(4):985–986
Potts MB, Lau D, Abla AA, Kim H, Young WL, Lawton MT (2015) Current surgical results with low-grade arteriovenous malformations. J Neurosurg 122:912–920
Quinn TJ, Dawson J, Walters MR, Lees KR (2009) Reliability of the modified Rankin Scale. A systematic review. Stroke 40:3393–3395
Reponen E, Tuominen H, Hernesniemi J, Korja M (2016) Modified Rankin Scale and short-term outcome in cranial neurosurgery: a prospective and unselected cohort study. World Neurosurg 91:567–573
Rohn B, Haenggi D, Etminan N, Kunz M, Turowski B, Steiger HJ (2014) Epilepsy, headache, and quality of life after resection of cerebral arteriovenous malformations. J Neurol Surg A Cent Eur Neurosurg 75(4):282–288
Rohn B, Hänggi D, Etminan N, Turowski B, Steiger HJ (2017) Relief of epilepsy and headache and quality of life after microsurgical treatment of unruptured brain AVM—audit of a single-center series and comprehensive review of the literature. Neurosurg Rev 40(1):59–65
Schramm J, Schaller K, Esche J, Bostrom A (2017) Microsurgery for cerebral arteriovenous malformations: subgroup outcomes in a consecutive series of 288 cases. J Neurosurg 125:1056–1063
Shah S, Cooper B (1993) Issues in the choice of activities of daily living assessment. Aust Occup Ther J 40(2):77–82
Spetzler RF, Martin NA (1986) A proposed grading system for arteriovenous malformations. J Neurosurg 65(4):476–483
Spetzler RF, Ponce FA (2011) A 3-tier classification of cerebral arteriovenous malformations. J Neurosurg 114(3):842–849
van der Schaaf IC, Brilstra EH, Rinkel GJ, Bossuyt PM, van Gijn J (2002) Quality of life, anxiety, and depression in patients with an untreated intracranial aneurysm or arteriovenous malformation. Stroke 33(2):440–443
Van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJA, Van Gijn J (1988) Interobserver agreement for the assessment of handicap in stroke patients. Stroke 19(5):604–607
Ware JE Jr, Bayliss MS, Rogers WH, Kosinski M, Tarlov AR (1996) Differences in 4-year health outcomes for elderly and poor, chronically ill patients treated in HMO and fee-for-service systems. Results from the Medical Outcomes Study. JAMA 276:1039–1047
Ware JE Jr, Kosinski MA (2002) SF-36 physical and mental health summary scales: a manual for users of version 1, 2nd edn. QualityMetric Incorporated, Lincoln
Ware JE Jr, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30(6):473–483
Wedderburn CJ, van Beijnum J, Bhattacharya JJ, Counsell CE, Papanastassiou V, Ritchie V, Roberts RC, Sellar RJ, Warlow CP, Al-Shahi Salman R (2008) Outcome after interventional or conservative management of unruptured brain arteriovenous malformations: a prospective, population-based cohort study. Lancet Neurol 7(3):223–230
Wong J, Slomovic A, Ibrahim G, Radovanovic I, Tymianski M (2017) Microsurgery for ARUBA trial (A Randomized Trial of Unruptured Brain Arteriovenous Malformations)-eligible unruptured brain arteriovenous malformations. Stroke 48:136–144
Funding
The Australian series was funded by the Macquarie University Post-Graduate Research Fund and Australian Government Research Training Program Scholarship. The Scottish study was funded by the Medical Research Council (grants G84/5176, G108/613, and G1002605), the Chief Scientist Office of the Scottish Government (grants K/MRS/50/C2704 and CZB/4/35), and the Stroke Association (grant TSA04/01). The sponsor had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Conflict of interest
The authors declared that they have no competing interests.
Rights and permissions
About this article

Cite this article
O’Donnell, J.M., Al-Shahi Salman, R., Manuguerra, M. et al. Quality of life and disability 12 months after surgery vs. conservative management for unruptured brain arteriovenous malformations: Scottish population-based and Australian hospital-based studies. Acta Neurochir 160, 559–566 (2018). https://doi.org/10.1007/s00701-017-3451-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-017-3451-2