
Abstract
Purpose
Stoma reversal carries a risk of surgical site infection (SSI). Purse-string approximation (PSA) has been reported as an attractive alternative to conventional primary wound closure for stoma reversal, but its efficacy is still under debate.
Methods
Patients undergoing elective stoma reversal were randomized to undergo PSA or primary closure with a drain (PCD). All patients received preoperative bowel cleansing and antimicrobial prophylaxis. The primary endpoint was the incidence of wound healing at the stoma site 30 days after surgery. The secondary endpoint was the 30-day SSI rate after surgery.
Results
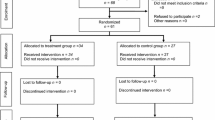
A total of 159 patients (PCD group, n = 79; PSA group, n = 80) were eligible for this study. The incidence of wound healing at the stoma site was 92.4% in the PCD group and 62.5% in the PSA group [difference (95% confidence interval − 29.9% (− 42.9 to − 16.9%)]. The 30-day SSI rate at the stoma site, as the secondary endpoint, was 8.9% in the PCD group and 5.0% in the PSA group (P = 0.35).
Conclusions
These results suggest that PCD may remain the standard procedure for stoma reversal surgery.

Similar content being viewed by others


References
Tan WS, Tang CL, Shi L, Eu KW. Meta-analysis of defunctioning stomas in low anterior resection for rectal cancer. Br J Surg. 2009;96:462–72.
Chude GG, Rayate NV, Patris V, Koshariya M, Jagad R, Kawamoto J, et al. Defunctioning loop ileostomy with low anterior resection for distal rectal cancer: should we make an ileostomy as a routine procedure? A prospective randomized study. Hepatogastroenterology. 2008;55:1562–7.
Lahat G, Tulchinsky H, Goldman G, Klauzner JM, Rabau M. Wound infection after ileostomy closure: a prospective randomized study comparing primary vs. delayed primary closure techniques. Tech Coloproctol. 2005;9:206–8.
Milanchi S, Nasseri Y, Kidner T, Fleshner P. Wound infection after ileostomy closure can be eliminated by circumferential subcuticular wound approximation. Dis Colon Rectum. 2009;52:469–74.
Hackam DJ, Rotstein OD. Wound infection during stoma closure. Can J Surg. 1995;38:191.
Murray BW, Cipher DJ, Pham T, Anthony T. The impact of surgical site infection on the development of incisional hernia and small bowel obstruction in colorectal surgery. Am J Surg. 2011;202:558–60.
Wong KS, Remzi FH, Gorgun E, Arrigain S, Church JM, Preen M, et al. Loop ileostomy closure after restorative proctocolectomy: outcome in 1,504 patients. Dis Colon Rectum. 2005;48:243–50.
Li LT, Brahmbhatt R, Hicks SC, Davila JA, Berger DH, Liang MK. Prevalence of surgical site infection at the stoma site following four skin closure techniques: a retrospective cohort study. Dig Surg. 2014;31:73–8.
Berne TV, Griffith CN, Hill J, LoGuidice P. Colostomy wound closure. Arch Surg. 1985;120:957–9.
Gruessner U, Clemens M, Pahlplatz PV, Sperling P, Witte J, Rosen HR, et al. Improvement of perineal wound healing by local administration of gentamicin-impregnated collagen fleeces after abdominoperineal excision of rectal cancer. Am J Surg. 2001;182:502–9.
Haase O, Raue W, Böhm B, Neuss H, Scharfenberg M, Schwenk W. Subcutaneous gentamycin implant to reduce wound infections after loop-ileostomy closure: a randomized, double-blind, placebo-controlled trial. Dis Colon Rectum. 2005;48:2025–31.
Banerjee A. Pursestring skin closure after stoma reversal. Dis Colon Rectum. 1997;40:993–4.
Sutton CD, Williams N, Marshall LJ, Lloyd G, Thomas WM. A technique for wound closure that minimizes sepsis after stoma closure. ANZ J Surg. 2002;72:766–7.
Mirbagheri N, Dark J, Skinner S. Factors predicting stomal wound closure infection rates. Tech Coloproctol. 2013;17:215–20.
Li LT, Hicks SC, Davila JA, Kao LS, Berger RL, Arita NA, et al. Circular closure is associated with the lowest rate of surgical site infection following stoma reversal: a systematic review and multiple treatment meta-analysis. Colorectal Dis. 2014;16:406–16.
Lim JK, Saliba L, Smith MJ, McTavish J, Raine C, Curtin P. Normal saline wound dressing—is it really normal? Br J Plast Surg. 2000;53:42–5.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20:250–78.
Ishibashi K, Ishida H, Kuwabara K, Ohsawa T, Okada N, Yokoyama M, et al. Short-term intravenous antimicrobial prophylaxis for elective rectal cancer surgery: results of a prospective randomized non-inferiority trial. Surg Today. 2014;44:716–22.
Ishibashi K, Kuwabara K, Ishiguro T, Ohsawa T, Okada N, Miyazaki T, et al. Short-term intravenous antimicrobial prophylaxis in combination with preoperative oral antibiotics on surgical site infection and methicillin-resistant Staphylococcus aureus infection in elective colon cancer surgery: results of a prospective randomized trial. Surg Today. 2009;39:1032–9.
Lopez MP, Melendres MF, Maglangit SA, Roxas MF, Monroy HJ 3rd, Crisostomo AC. A randomized controlled clinical trial comparing the outcomes of circumferential subcuticular wound approximation (CSWA) with conventional wound closure after stoma reversal. Tech Coloproctol. 2015;19:461–8.
Makuch R, Simon R. Sample size requirements for evaluating a conservative therapy. Cancer Treat Rep. 1978;62:1037–40.
Dunnett CW, Gent M. Significance testing to establish equivalence between treatments, with special reference to data in the form of 2 × 2 tables. Biometrics. 1977;33:593–602.
Reid K, Pockney P, Pollitt T, Draganic B, Smith SR. Randomized clinical trial of short-term outcomes following purse-string versus conventional closure of ileostomy wounds. Br J Surg. 2010;97:1511–7.
Dusch N, Goranova D, Herrle F, Niedergethmann M, Kienle P. Randomized controlled trial: comparison of two surgical techniques for closing the wound following ileostomy closure: purse string vs direct suture. Colorectal Dis. 2013;15:1033–40.
Lee JT, Marquez TT, Clerc D, Gie O, Demartines N, Madoff RD, et al. Pursestring closure of the stoma site leads to fewer wound infections: results from a multicenter randomized controlled trial. Dis Colon Rectum. 2014;57:1282–9.
Camacho-Mauries D, Rodriguez-Díaz JL, Salgado-Nesme N, González QH, Vergara-Fernández O. Randomized clinical trial of intestinal ostomy takedown comparing pursestring wound closure vs conventional closure to eliminate the risk of wound infection. Dis Colon Rectum. 2013;56:205–11.
O’Leary DP, Carter M, Wijewardene D, Burton M, Waldron D, Condon E, et al. The effect of purse-string approximation versus linear approximation of ileostomy reversal wounds on morbidity rates and patient satisfaction: the ‘STOMA’ trial. Tech Coloproctol. 2017;21:863–8.
Cohen PR, Martinelli PT, Schulze KE, Nelson BR. The purse-string suture revisited: a useful technique for the closure of cutaneous surgical wounds. Int J Dermatol. 2007;46:341–7.
Tremolada C, Blandini D, Beretta M, Mascetti M. The “round block” purse-string suture: a simple method to close skin defects with minimal scarring. Plast Reconstr Surg. 1997;100:126–31.
Williams LA, Sagar PM, Finan PJ, Burke D. The outcome of loop ileostomy closure: a prospective study. Colorectal Dis. 2008;10:460–4.
Yoon SI, Bae SM, Namgung H, Park DG. Clinical trial on the incidence of wound infection and patient satisfaction after stoma closure: comparison of two skin closure techniques. Ann Coloproctol. 2015;31:29–33.
Acknowledgements
We thank Professor Tomoyuki Kawada, Department of Public Health, Nippon Medical School, for his valuable assistance with the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interest to declare.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Amamo, K., Ishida, H., Kumamoto, K. et al. Purse-string approximation vs. primary closure with a drain for stoma reversal surgery: results of a randomized clinical trial. Surg Today 49, 231–237 (2019). https://doi.org/10.1007/s00595-018-1729-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-018-1729-5